

Abstract
Large osteoarthritic cysts can sometimes be difficult to distinguish from primary osseous and soft tissue tumours. We present such a case involving a cyst arising from the hip joint and eroding the acetabulum which presented as a soft tissue malignancy referred to a tertiary bone and soft tissue tumour centre. We discuss the diagnostic problems it may pose, and present a literature review of the subject.
Keywords: Osteoarthritic cyst
Osteoarthritis is a degenerative joint disease and one of the recognised characteristics is that of cyst formation. Cysts more commonly develop in degenerative diseases involving weight-bearing joints such as the hip.1 There have been several reported cases of large symptomatic subchondral cysts secondary to osteoarthritis including the knee2 and facet joint.3 Two cases of large cysts associated with osteoarthritis involving the femur4,4 demonstrate that these subchondral lucencies can be so pronounced they may be confused with soft tissue malignancy. We describe a case of a patient with an osteoarthritic cyst arising from the right hip joint and the diagnostic problems it may pose.
Case report
A 60-year-old man was referred from his local hospital to a tertiary bone and soft tissue tumour centre with an incidental finding of a large soft tissue lesion identified following radiological investigations of right hip pain. He initially presented with a 6-month history of right hip pain associated with weight loss. On examination of the hip, there was painful restricted movement indicative of arthritis with no clinical evidence of regional lymph-adenopathy or malignancy.
Plain radiographs of the pelvis (Fig. 1) showed a large cystic lesion arising superolaterally over the right hip eroding the acetabulum. There were features of advanced osteoarthritis of the right hip with evidence of osteophyte formation and loss of joint space. A reactive area of bone formation occupying the lateral aspect of the acetabulum and extending into soft tissue was noted but features were not typical of a neoplastic process. Subsequent magnetic resonance imaging (MRI) demonstrated a lobulated cystic lesion arising superolateral to the hip joint and eroding the adjacent acetabulum. Rim enhancement was demonstrated following administration of gadolinium and features were consistent with an acetabular labral cyst. In view of the size of the lesion, the patient underwent a computer tomography (CT) guided biopsy of the lesion for definitive diagnosis (Fig. 2).
Figure 1.

Radiograph of right hip demonstrating large cystic lesion.
Figure 2.
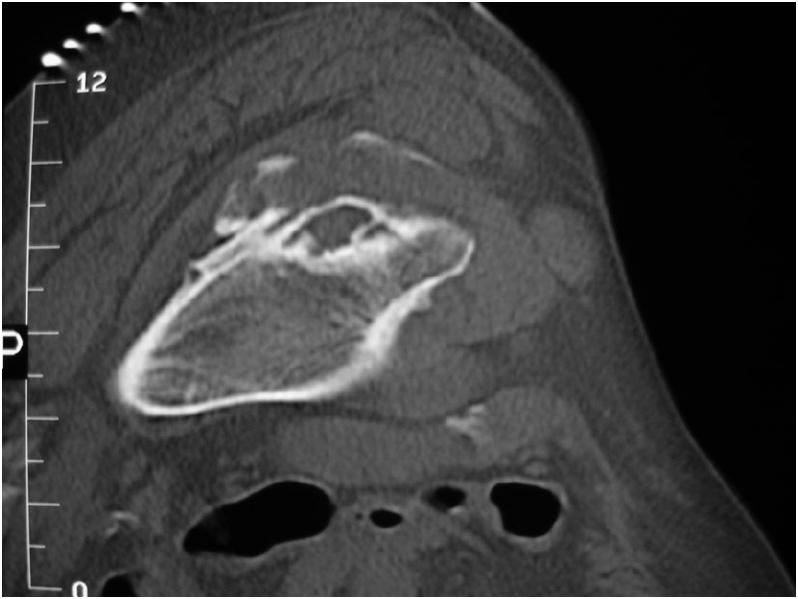
Axial computed tomographic image showing cystic lesion associated with right hip joint.
Histological features were consistent, although not diagnostic, of a degenerative process such as a geode. A primary total hip replacement was recommended in view of the findings.
The patient underwent a primary total hip replacement and tissue specimens sent from the operation excluded the diagnosis of malignancy.
Discussion
The term cyst denotes a fluid-filled cavity with an epithelial lining but subchondral cavities associated with degenerative joint disease typically do not possess an epithelial lining. The nomenclature subchondral geode, which denotes a hollow rock, may be a more appropriate term for such lesions and will be the term used from hereon.
Subchondral geodes are common entities in osteoarthritis but the aetiology is still a matter of debate. There are two theories proposed with regard to the pathogenesis of subchondral geodes in these cases. Intrusion of synovial fluid through the cartilage secondary to elevated intra-articular pressure6,7 has been proposed as a possible aetiology. However, this does not explain cases in which subchondral geodes are not in continuity with the joint. The other mechanism by which geodes are thought to form is that based on stress-induced bone resorption.1,8 In this theory, it is believed that stress-induced micro-fractures lead to secondary effects such as osteoclast resorption and thus geode formation.
Geodes are often multiple and variable in size whereas solitary and large geodes are unusual. Thus, difficulties arise in diagnosis when large geodes become the dominant radiological feature in degenerative joint disease. There has been one documented case of a patient commencing a course of radiotherapy for a suspected diagnosis of liposarcoma when subsequent findings demonstrated the lesion to be a geode.4 This high-lights the need for clinicians to be aware of such radiographic presentations of geodes in osteoarthritis.
Plain radiographs demonstrating subchondral geodes in the presence of osteoarthritis often have clues to indicate the geodes are part of a degenerative process as opposed to a neoplasm. These features include the presence of multiple, small geodes with subchondral sclerosis, marginal osteophytes and loss of joint space. Primary osseous lesions that may be a differential diagnosis of a cystic lesion around the hip joint include giant cell tumours, intra-osseous ganglia and chondroblastomas.
Giant cell tumours are lobulated cyst-like lesions and, radiographically, have a multiloculated appearance with a non-sclerotic margin associated with thinning of the overlying cortex. Intra-osseous ganglia are solitary, subchondral, cystic lesions that may be unilocular or multilocular in nature with a well-defined sclerotic margin. Chondroblastomas present radiographically as lytic lesions with varying degree of central or peripheral sclerosis and subchondral geodes may mimic such lesions. Unless the conditions co-exist, there will be absence of the radiographic hallmarks of osteoarthritis with all these lesions.
Conclusions
Knowledge of the radiographic appearances, along with clinical information obtained during history and examination should enable the clinician to differentiate benign entities from more aggressive processes such as tumour. However, in cases of osteoarthritis where diagnosis is in doubt as a result of the presence of a large geode, referral to a tertiary centre is recommended for review by specialist radiologists and surgeons for a definitive diagnosis and appropriate management.
References
- 1.Ondrouch AS. Cyst formation in osteoarthritis. J Bone Joint Surg Br. 1963;45:755–60. [PubMed] [Google Scholar]
- 2.Bianchi S, Abdelwahab IF, Zwass A, Rettagliata F, Federici E, Ricci G. Expansile subchondral degenerative bone cyst secondary to osteoarthritis. Can Assoc Radiol J. 1995;46:308–10. [PubMed] [Google Scholar]
- 3.Shirado O, Kaneda K. Large osteoarthritic bone cyst of the facet joint causing low back pain and sciatica. Orthopedics. 1997;20:472–5. doi: 10.3928/0147-7447-19970501-19. [DOI] [PubMed] [Google Scholar]
- 4.Cohen AP, McWilliams TG. Giant geode (pseudocyst) formation of the femoral neck in a case of osteoarthritis. Rheumatology (Oxford) 2000;39:443–4. doi: 10.1093/rheumatology/39.4.443. [DOI] [PubMed] [Google Scholar]
- 5.Beingessner DM, Spouge AR, Thain LM, Rorabeck CH. Musculoskeletal case 7. Presentation. Large femoral geode associated with osteoarthritis of the hip joint. Can J Surg. 1999;42:414–432. [PMC free article] [PubMed] [Google Scholar]
- 6.Landells JW. The bone cysts of osteoarthritis. J Bone Joint Surg Br. 1953;35:643–9. doi: 10.1302/0301-620X.35B4.643. [DOI] [PubMed] [Google Scholar]
- 7.Freund E. The pathological significance of intra-articular pressure. Edinb Med J. 1940;47:192–203. [PMC free article] [PubMed] [Google Scholar]
- 8.Durr HD, Martin H, Pellengahr C, Schlemmer M, Maier M, Jansson V. The cause of subchondral bones cysts in osteoarthrosis: a finite element analysis. Acta Orthop Scand. 2004;75:554–8. doi: 10.1080/00016470410001411. [DOI] [PubMed] [Google Scholar]