

Abstract
Torted appendices are a rare occurrence but should be considered when encountering a haemorrhagic congested appendix on laparoscopy. As adhesions are rarely present, laparoscopic excision is usually a feasible option.
Keywords: Laparoscopy, Torsion, Appendix, Appendicitis
Case report
A 29-year-old woman was admitted to our accident and emergency department with a 24-h history of right iliac fossa pain and anorexia. Her inflammatory markers were elevated. Laparoscopy the following day revealed a turgid, congested, gangrenous appendix in the pelvic position. It was twisted 360° just distal to its base (Fig. 1). The base proximal to the twist was normal. There was no evidence of inflammation or adhesions to the mass. There was a minimal amount of free fluid and an otherwise normal laparoscopy. Appendix was transected between endoclips. The specimen was removed in an Endocatch. The pathology showed 110 × 45 × 14 mm haemorrhagic appendix with a 10-mm breach in the wall extruding mucus. Focal necrotic areas were present in the wall with patchy areas of inflammation. There was no evidence of malignancy. She made an unremarkable recovery and was discharged the following day.
Figure 1.
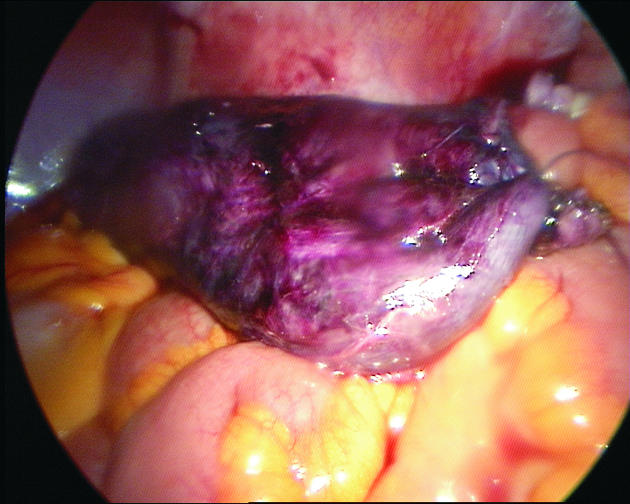
Torted appendix.
Discussion
Torsion of the vermiform appendix is extremely rare. The first reported case was in 1918.1 Since then there have been less than 30 cases reported in the literature. The only other laparoscopic case found in the literature was reported recently.2 The majority are in the paediatric population. There does not seem to be a gender predilection.3
The presentation is identical to acute appendicitis and can only be definitely diagnosed at the time of operation.4 Ultrasound investigation may be useful in women to rule out other differential diagnoses.3
The direction of twist is usually counter-clockwise and the site is either at the base or up to a centimetre distal. The pathophysiology of the condition is unclear. Postulated theories suggest either a primary or secondary phenomenon. Features favouring a primary cause are a long, fan-shaped meso-appendix with a narrow base and pelvic position. Secondary causes are attributed to a luminal obstruction (e.g. faecolith leading to a mucocoele), inflammation or, rarely, a mucinous cystadenoma, causing distension and a subsequent torsion.5
Our case was a mucocoele with a narrow base in the pelvic position, illustrating that primary and secondary factors in combination may play a role in the aetiology.
Torted appendices are a rare occurrence but should be considered when encountering a haemorrhagic, congested appendix on laparoscopy. As adhesions are rarely present, laparoscopic excision is usually a feasible option.
References
- 1.Payne JE. A case of torsion of the appendix. Br J Surg. 1918;6:327. [Google Scholar]
- 2.Bowling CB, Lipscomb GH. Torsion of the appendix mimicking ovarian torsion C. Obstet Gynecol. 2006;107:466–7. doi: 10.1097/01.AOG.0000164066.65435.49. [DOI] [PubMed] [Google Scholar]
- 3.Gopal K, Kumar S, Grewal H. Torsion of the vermiform appendix. J Pediatr Surg. 2005;40:446–7. doi: 10.1016/j.jpedsurg.2004.10.027. [DOI] [PubMed] [Google Scholar]
- 4.Merrett ND, Lubowski DZ, King DW. Torsion of the vermiform appendix: a case report and review of literature. Aust NZ J Surg. 1992;62:981–3. doi: 10.1111/j.1445-2197.1992.tb07661.x. [DOI] [PubMed] [Google Scholar]
- 5.Moten AL, Williams RS. Torsion of the appendix. Med J Aust. 2002;177:632. doi: 10.5694/j.1326-5377.2002.tb04990.x. [DOI] [PubMed] [Google Scholar]