

Abstract
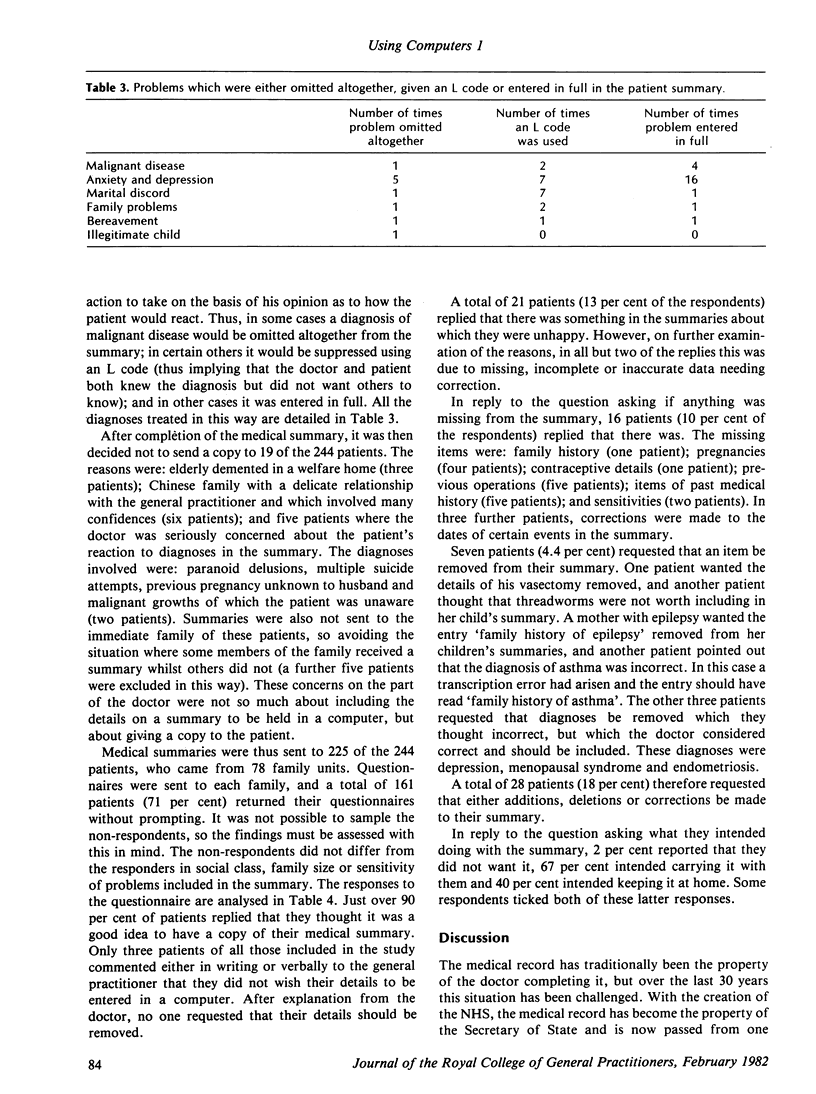
Medical summaries were prepared by a general practitioner for inclusion in a computer system. Both the medical records and a patient-filled questionnaire were used. A representative sample of the practice population were then sent their summaries. In creating the summaries the general practitioner felt the need to exclude 11 diagnoses whenever they appeared (5 per cent of the patients), and to suppress one or more diagnoses in a further 14 per cent of patients. In 2 per cent of summaries the general practitioner felt unable to give a copy to the patient because he was afraid of an adverse reaction by the patient or immediate relatives.
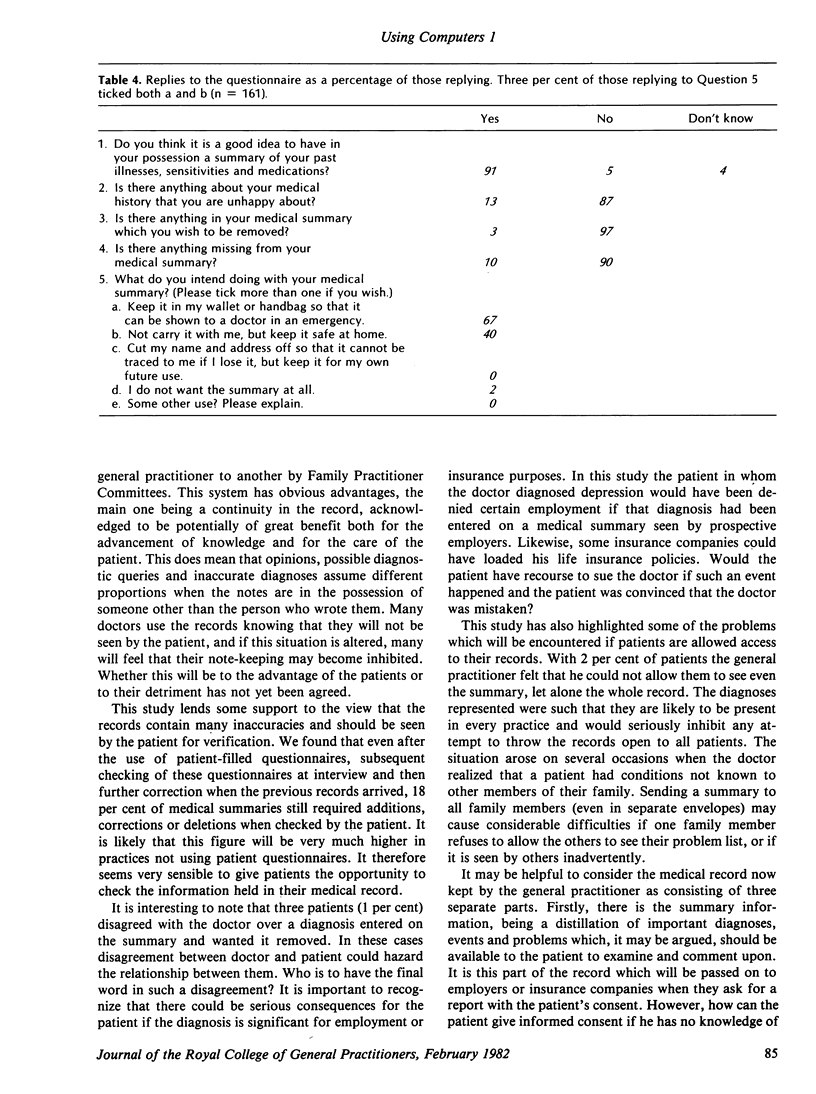
The patients' views of the usefulness of the summaries, and of their accuracy and completeness, were sought by a questionnaire. Replies were received from 71 per cent; of these, 91 per cent reported that they thought the summary useful. However, in 18 per cent of cases, the patients requested additions, corrections or deletions. Only 1 per cent of patients replied that they definitely did not like the idea of a computer containing their medical information.
Some of the benefits and difficulties both of using a computer to store medical information, and of giving the patient a copy of the medical summary, are discussed.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Jones R. V., Richards S. J. Confidentiality and medical records. J R Coll Gen Pract. 1978 Mar;28(188):137–140. [PMC free article] [PubMed] [Google Scholar]
- Rector A. L., Metcalfe D. H., Hallam L., Clayden A. D. Medical records and medical information in the U.K.--issues and prospects. Public Health. 1979 Sep;93(5):290–299. doi: 10.1016/s0033-3506(79)80080-3. [DOI] [PubMed] [Google Scholar]
- Sheldon M. G. Self-audit of prescribing habits and clinical care in general practice. J R Coll Gen Pract. 1979 Dec;29(209):703-6, 710-1. [PMC free article] [PubMed] [Google Scholar]