

Abstract
Purpose:
To determine the in vitro motion of the scaphoid and lunate during wrist circumduction and wrist dart-throw motions and to see how these motions change after the ligamentous stabilizers of the scaphoid and lunate are sectioned in a manner simulating scapholunate instability.
Methods:
Twenty-one fresh-frozen cadaver forearms were moved through a dart-throw motion and a circumduction motion using a wrist joint simulator. Scaphoid and lunate motion were measured with the wrist ligaments intact and after sectioning of the scapholunate interosseous ligament, the scaphotrapezium ligament, and the radioscaphocapitate ligament.
Results:
In the intact wrist the scaphoid and lunate moved more during circumduction than during the dart-throw motion. With ligamentous sectioning the scaphoid flexed more and the lunate extended more during both the circumduction and dart-throw motions. During the circumduction motion both before and after sectioning the global motion of the scaphoid was greater than that of the lunate. After sectioning the scaphoid motion increased and the lunate motion decreased.
Conclusions:
The scaphoid and lunate motions were observed to change remarkably after ligamentous sectioning. The observed changes in carpal motion correlate with the clinical observation that after ligamentous injury arthritic changes occur in the radioscaphoid joint and not in the radiolunate joint. Analysis of the injured wrist in positions that combine flexion-extension and radial-ulnar deviation may allow noninvasive diagnosis of specific wrist ligament injuries.
Keywords: Carpal motion, wrist circumduction motion, wrist dart-throw motion, kinematics, scapholunate interosseous ligament, scaphoid, lunate
Many activities involving the wrist are motions that require a combination of wrist flexion-extension and radial-ulnar deviation. These motions frequently include a dart-throw type of motion.1 Although the in vivo and in vitro motions of the wrist carpal bones during planar wrist flexion-extension and planar wrist radial-ulnar deviation have been studied,2−13 a dart-throw motion only now is being studied in an organized biomechanical fashion.14−16 For this study we chose to study a dart-throw motion with a limited (20° total) radial-ulnar deviation motion, which may not be indicative of the motion used in throwing a ball or other activities with extreme ranges of motion. In some activities such as stirring a bowl, wrist circumduction is the primary motion. The purpose of this study was to determine the in vitro motion of the scaphoid and lunate during these functional arcs of wrist motion. A second purpose was to see how these motions change after the ligamentous stabilizers of the scaphoid and lunate are sectioned in a manner simulating scapholunate instability.
Methods
A wrist-joint motion simulator17 was used to move 21 fresh-frozen cadaver wrists through cyclic dart-throw and cyclic circumduction motions. The average age of the specimens was 67 years (range, 31−87 y) and there were 11 male and 10 female specimens. Each wrist was moved by pulling on the wrist flexors and extensors by hydraulic cylinders under computer control, using both force feedback and position control. The dart-throw motion corresponded to a cyclic motion with the wrist starting at 30° of wrist extension and 10° of radial deviation and moving to 30° of wrist flexion and 10° of ulnar deviation and then back to wrist extension and radial deviation for 6 cycles. This dart motion corresponds to the arc C shown in a previous publication.15 The circumduction motion corresponded to an elliptic motion having the same extremes of motion as the dart-throw motion but with the wrist first in 10° of radial deviation, moving to 30° of flexion (with no radial-ulnar deviation), then to 10° of ulnar deviation (with no flexion-extension), to 30° of extension (with no radial-ulnar deviation), and back to radial deviation. This also was repeated for 6 cycles. In each arm the motions of the scaphoid and lunate were measured using electromagnetic motion sensors (Fastrak; Polhemus, Colchester, VT) mounted onto carbon fiber rods cemented into the dorsal aspect of each bone. The motion of the third metacarpal was measured by directly attaching a sensor to the third metacarpal and was assumed equivalent to the motion of the wrist. The motion data were measured continuously during smooth motions of the wrist between the predetermined end points for both circumduction and the dart-throw motions.
Kinematic data were collected with the wrist soft tissues intact. The scapholunate interosseous ligament, the scaphotrapezium ligament, and the radioscaphocapitate ligament then were sectioned as described previously18 and each wrist was moved through 1,000 cycles of wrist flexion-extension to simulate the clinical situation of instability occurring several weeks after the acute injury because of continued use. Kinematic data again were collected and defined as unstable. The neutral scaphoid, lunate, and wrist positions were defined with the intact wrist being held under computer control at neutral flexion-extension and neutral radial-ulnar deviation under low tendon loading. For each dart-throw and circumduction motion the extremes of the angular motion of each carpal bone were determined.
Each motion then was visualized in the transverse plane as from the fingertips. The third metacarpal circumduction motion appears as an oval (Fig. 1) and the dart-throw motion appears as a diagonal line (Fig. 2). For each circumduction motion the 2-dimensional centroid of the motion in the transverse plane and the area of the motion as viewed in the transverse plane were computed. The centroid of motion can be considered as the center point of the motion. The area of motion is computed from the area within the oval or enclosed region of bone motion. The area of motion might be considered an indicator of the overall global motion of the bone. Differences were tested using a 1-way repeated-measures analysis of variance at a p value of less than .05.
Figure 1.
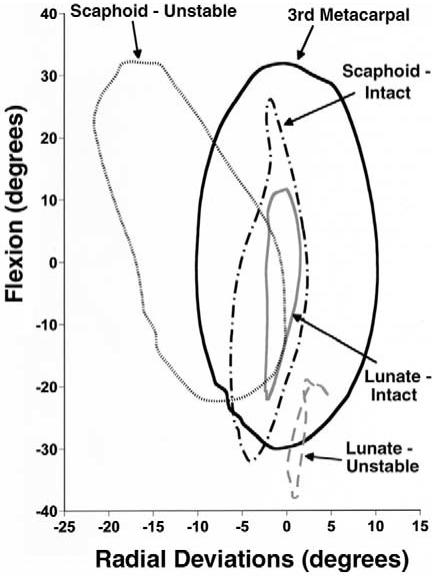
Motion of the third metacarpal, scaphoid, and lunate for a wrist circumduction motion viewed from the fingertips in the transverse plane with all wrist structures intact (intact) and with the scapholunate interosseous ligament, scaphotrapezium ligament, and radioscaphocapitate ligament sectioned and after 1,000 cycles of wrist motion (unstable). The motion of the wrist is viewed as an oval. The area within the oval is considered to be representative of the global wrist motion. The areas within the scaphoid and lunate motions also are computed. Flexion and radial deviation are positive.
Figure 2.
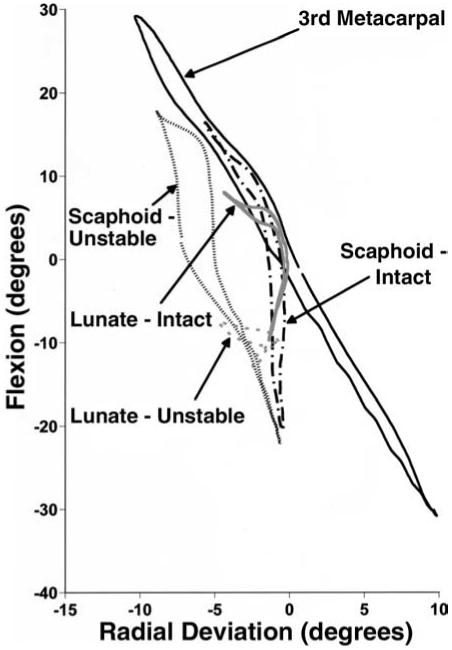
Motion of the third metacarpal, scaphoid, and lunate for a wrist dart-throw motion viewed from the finger-tips in the transverse plane with all wrist structures intact (intact) and with the scapholunate interosseous ligament, scaphotrapezium ligament, and radioscaphocapitate ligament sectioned and after 1,000 cycles of wrist motion (unstable). Flexion and radial deviation are positive.
Results
In the intact wrist the angular extremes of scaphoid and lunate flexion and extension were greater statistically during the circumduction motion (Table 1, Fig. 1) than during the dart-throw motion (Table 2, Fig. 2). The extremes of radial and ulnar deviation, however, were relatively small during both motions and were not statistically different between motions, perhaps because of the relatively small amount of wrist radial-ulnar deviation angulations during these motions. After ligamentous sectioning during the circumduction motion (Fig. 1) the unstable scaphoid statistically flexed more and extended less, and the unstable lunate statistically flexed less and extended more. Also the scaphoid statistically radially deviated less and ulnarly deviated more and the lunate statistically radially deviated more. After ligamentous sectioning during the dart-throw motion (Fig. 2) the unstable scaphoid statistically flexed more and the unstable lunate statistically flexed less and extended more. Also the scaphoid statistically deviated more ulnarly.
Table 1.
Wrist Circumduction Motion
| Angular Extremes | Scaphoid, degrees (SD) | Lunate, degrees (SD) | Third Metacarpal, degrees |
|---|---|---|---|
| Intact maximum flexion | 26.0 (3.6) | 18.0 (6.5) | 30.0 |
| Intact maximum extension | −28.2 (2.9) | −17.6 (6.3) | 30.0 |
| Intact maximum radial deviation | 3.5 (1.4) | 2.8 (1.4) | 10.0 |
| Intact maximum ulnar deviation | −4.5 (2.5) | −3.9 (1.9) | 10.0 |
| Unstable maximum flexion | 33.8 (4.8) | 0.8 (9.7) | 30.0 |
| Unstable maximum extension | −21.8 (9.0) | −23.5 (9.0) | 30.0 |
| Unstable maximum radial deviation | −0.3 (7.3) | 4.4 (2.7) | 10.0 |
| Unstable maximum ulnar deviation | −16.6 (7.9) | −3.1 (2.6) | 10.0 |
Flexion and radial deviation are defined as positive.
Table 2.
Wrist Dart-Throw Motion
| Angular Extremes | Scaphoid, degrees (SD) | Lunate, degrees (SD) | Third Metacarpal, degrees |
|---|---|---|---|
| Intact maximum flexion | 17.6 (4.8) | 10.8 (7.3) | 30.0 |
| Intact maximum extension | −19.0 (4.0) | −8.5 (4.6) | 30.0 |
| Intact maximum radial deviation | 2.8 (1.5) | 1.8 (1.5) | 10.0 |
| Intact maximum ulnar deviation | −3.3 (2.3) | −5.2 (5.0) | 10.0 |
| Unstable maximum flexion | 28.2 (5.2) | −0.8 (10.9) | 30.0 |
| Unstable maximum extension | −17.6 (7.2) | −18.4 (8.6) | 30.0 |
| Unstable maximum radial deviation | 0.8 (5.9) | 2.1 (2.4) | 10.0 |
| Unstable maximum ulnar deviation | −13.3 (7.5) | −3.7 (2.5) | 10.0 |
Flexion and radial deviation are defined as positive.
During the intact dart-throw motion the scaphoid and lunate generally followed the path of wrist motion defined by radial deviation in extension and ulnar deviation in flexion. With ligamentous sectioning the path of the scaphoid and lunate became variable.
During the circumduction motion (Table 3, Fig. 1) the area of motion of the scaphoid before or after ligament sectioning statistically was greater than the motion of the lunate before or after ligament sectioning. The global motion of the scaphoid after sectioning was greater statistically than before sectioning whereas the converse was true for the lunate. The lunate statistically moved less after sectioning. The centroid of scaphoid motion statistically moved ulnarly and into flexion after ligament sectioning whereas the centroid of the lunate moved toward extension.
Table 3.
Wrist Circumduction Motion
| Carpal Status | Area (SD) | Xbar (SD) | Ybar (SD) |
|---|---|---|---|
| Scaphoid: intact wrist | 215.5 (100.6) | −0.3 (1.6) | −2.7 (4.4) |
| Scaphoid: unstable wrist | 626.1 (206.3) | −7.2 (5.8) | 5.0 (5.0) |
| Lunate: intact wrist | 126.8 (83.7) | −0.6 (1.1) | 2.1 (4.4) |
| Lunate: unstable wrist | 54.4 (38.1) | −0.1 (2.1) | −8.5 (7.5) |
Area, total motion of carpal bone = area of circumduction motion (degree2); positive Xbar, centroid movement toward radial deviation (degree); positive Ybar, centroid movement toward flexion (degree)
Qualitatively after ligamentous sectioning, increased scaphoid dorsal-volar motion was observed in 9 of 21 arms such that the scaphoid would ride up onto the dorsal rim of the radius during part of the wrist motion. After ligamentous sectioning a gap also was observed between the scaphoid and lunate in 16 of the 21 arms, suggesting an increase in the radial-ulnar motion of the scaphoid.
Discussion
The purpose of this study was to understand better how the scaphoid and lunate move during wrist dart-throw and circumduction motions. In the intact specimen the motion of the scaphoid and lunate generally follow the motion of the wrist or third metacarpal but to a lesser magnitude. After ligament sectioning the scaphoid and lunate motions were observed to change remarkably.
These observations are based on the motions tested in this study in which the motion end points were limited to 30° of flexion, 30° of extension, 10° of radial deviation, and 10° of ulnar deviation. A study that examines a larger range of motion may provide different findings. The dart-throw motion tested in this study based on these end points is thought to represent a functional arc of wrist motion used in activities of daily living.1 Other dart-throw motions in which there are equal amounts of wrist flexion and ulnar deviation and extension and radial deviation15 have been shown in the intact wrist to have less carpal motion than the dart motion studied here.
Measurement of scaphoid and lunate motion can be affected if the cable to the electromagnetic motion sensor (Fastrak) is positioned poorly, causing the composite rod cemented into the carpal bone to twist. Before each experiment each wrist was moved through a range of motions and the cable was taped in a position to allow sufficient slack to prevent a torque from being applied to the sensor. The composite rods were placed into holes in the dorsal aspect of the carpal bones so that there was no interference with the dorsal capsular structures and so that the rods did not impinge with each other or the dorsal radius. The wrists in which impingement occurred were not included in this study.
A limitation of this study was the manner in which the areas and centroid locations were calculated for the circumduction motions. In 4 of the 21 arms a small portion of the circumduction motion for the scaphoid and lunate appeared as a figure of eight. The motion was not a single area but 2 or more areas. The methods used to compute the area and centroid would have subtracted this smaller area from the major area. Therefore these arms were deleted from the statistical analysis of the area measurements.
Little data have been presented on how the scaphoid and lunate move during wrist circumduction. Previously we showed14 that during circumduction the scaphoid, lunate, and triquetrum generally follow the path of wrist motion. Other investigators such as Salvia et al19 measured the amount of global wrist motion during circumduction but not the individual carpal bone motions.
More research has been performed on how the carpal bones move during a dart-throw motion.15,16 Ishikawa et al16 examined changes in carpal kinematics during wrist flexion-extension, radial-ulnar deviation, and the dart-throw motion. Similar percent contributions of the lunate toward wrist motion were seen in the dart-throw motions of their study as compared with the current study. The benefit of the current study, however, was to provide comparisons between the dart-throw and circumduction motions and between the intact and the unstable wrist conditions for each arm.
The increased scaphoid motion (both angular and translational) and decreased lunate motion after ligament sectioning correlate well with clinical observations of carpal changes after wrist injury. These findings may help explain the clinical observation that after ligamentous injury to the wrist, arthritic changes occur in the radioscaphoid joint but not in the radiolunate joint. Early diagnosis of these injuries may prevent these arthritic changes. Analysis of the injured wrist in positions that combine flexion-extension and radial-ulnar deviation motion may allow noninvasive diagnosis of specific wrist ligament injuries.
Acknowledgments
Supported by extramural research from the National Center for Injury Prevention and Control (R49/CCR216814-03) from the Centers for Disease Control and Prevention; and by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1R01 AR050099-01).
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
References
- 1.Palmer AK, Werner FW, Murphy D, Glisson R. Functional wrist motion: a biomechanical study. J Hand Surg. 1985;10A:39–46. doi: 10.1016/s0363-5023(85)80246-x. [DOI] [PubMed] [Google Scholar]
- 2.Berger RA, Crowninshield RD, Flatt AE. The three-dimensional rotational behaviors of the carpal bones. Clin Orthop. 1982;167:303–310. [PubMed] [Google Scholar]
- 3.Ruby LK, Cooney WP, III, An KN, Linscheid RL, Chao EYS. Relative motion of selected carpal bones: a kinematic analysis of the normal wrist. J Hand Surg. 1988;13A:1–10. doi: 10.1016/0363-5023(88)90189-x. [DOI] [PubMed] [Google Scholar]
- 4.Patterson RM, Nicodemus CL, Viegas SF, Elder KW, Rosenblatt J. High-speed, three-dimensional kinematic analysis of the normal wrist. J Hand Surg. 1998;23A:446–453. doi: 10.1016/S0363-5023(05)80462-9. [DOI] [PubMed] [Google Scholar]
- 5.Kobayashi M, Berger RA, Nagy L, Linscheid RL, Uchiyama S, Ritt M, An KN. Normal kinematics of carpal bones: a three-dimensional analysis of carpal bone motion relative to the radius. J Biomech. 1997;30:787–793. doi: 10.1016/s0021-9290(97)00026-2. [DOI] [PubMed] [Google Scholar]
- 6.Wolfe SW, Neu C, Crisco JJ. In vivo scaphoid, lunate, and capitate kinematics in flexion and in extension. J Hand Surg. 2000;25A:860–869. doi: 10.1053/jhsu.2000.9423. [DOI] [PubMed] [Google Scholar]
- 7.Moojen TM, Snel JG, Ritt MJPF, Kauer JMG, Venema HW, Bos KE. Three-dimensional carpal kinematics in vivo. Clin Biomech. 2002;17:506–514. doi: 10.1016/s0268-0033(02)00038-4. [DOI] [PubMed] [Google Scholar]
- 8.Crisco JJ, Wolfe SW, Neu CP, Pike S. Advances in the in vivo measurement of carpal kinematics. Orthop Clin North Am. 2001;32:219–231. doi: 10.1016/s0030-5898(05)70244-3. [DOI] [PubMed] [Google Scholar]
- 9.Short WH, Werner FW, Green JK, Weiner MM, Masaoka S. The effect of sectioning the dorsal radiocarpal ligament and insertion of a pressure sensor into the radiocarpal joint on scaphoid and lunate kinematics. J Hand Surg. 2002;27A:68–76. doi: 10.1053/jhsu.2002.30074. [DOI] [PubMed] [Google Scholar]
- 10.Moojen TM, Snel JG, Ritt MJPF, Venema HW, Kauer JMG, Bos KE. In vivo analysis of carpal kinematics and comparative review of the literature. J Hand Surg. 2003;28A:81–87. doi: 10.1053/jhsu.2003.50009. [DOI] [PubMed] [Google Scholar]
- 11.Moritomo H, Murase T, Goto A, Oka K, Sugamoto K, Yoshikawa H. Capitate-based kinematics of the midcarpal joint during wrist radioulnar deviation: an in vivo three-dimensional motion analysis. J Hand Surg. 2004;29A:668–675. doi: 10.1016/j.jhsa.2004.04.010. [DOI] [PubMed] [Google Scholar]
- 12.Park MJ, Cooney WP, III, Hahn ME, Looi KP, An K-N. The effects of dorsally angulated distal radius fractures on carpal kinematics. J Hand Surg. 2002;27A:223–232. doi: 10.1053/jhsu.2002.32083. [DOI] [PubMed] [Google Scholar]
- 13.Goslings JC, DaSilva MF, Viegas SF, Perren SM, Patterson RM. Kinematics of the wrist with a new dynamic external fixation device. Clin Orthop. 2001;386:226–234. doi: 10.1097/00003086-200105000-00030. [DOI] [PubMed] [Google Scholar]
- 14.Werner FW, Short WH, Fortino MD, Palmer AK. The relative contribution of selected carpal bones to global wrist motion during simulated planar and out-of-plane wrist motion. J Hand Surg. 1997;22A:708–713. doi: 10.1016/S0363-5023(97)80133-5. [DOI] [PubMed] [Google Scholar]
- 15.Werner FW, Green JK, Short WH, Masaoka S. Scaphoid and lunate motion during a wrist dart throw motion. J Hand Surg. 2004;29A:418–422. doi: 10.1016/j.jhsa.2004.01.018. [DOI] [PubMed] [Google Scholar]
- 16.Ishikawa J-I, Cooney WP, III, Niebur G, An K-N, Minami A, Kaneda K. The effects of wrist distraction on carpal kinematics. J Hand Surg. 1999;24A:113–120. doi: 10.1016/S0266-7681(99)90057-8. [DOI] [PubMed] [Google Scholar]
- 17.Werner FW, Palmer AK, Somerset JH, Tong JJ, Gillison DB, Fortino MD, Short WH. Wrist joint motion simulator. J Orthop Res. 1996;14:639–646. doi: 10.1002/jor.1100140420. [DOI] [PubMed] [Google Scholar]
- 18.Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate. J Hand Surg. 2002;27A:991–1002. doi: 10.1053/jhsu.2002.35878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Salvia P, Woestyn L, David JH, Feipel V, Van S, Jan S, et al. Analysis of helical axes, pivot and envelope in active wrist circumduction. Clin Biomech. 2000;15:103–111. doi: 10.1016/s0268-0033(99)00055-8. [DOI] [PubMed] [Google Scholar]