

Abstract
We hypothesized that among overweight women smokers, those with childhood onset of weight problems may be more likely to engage in unhealthy eating and dieting behaviors, including smoking to control weight. Data were collapsed from 89 currently overweight (BMI≥25) women smokers who were recruited to participate in smoking research projects that focused on weight, body image, and food intake. We compared those who reported first becoming overweight before Junior High School (n=22) with those who recalled first experiencing weight problems during Junior High School or later (n=67). Women with Childhood Onset weight problems reported first trying cigarettes at a significantly younger age than those with Later Onset (13 vs. 15 years of age, respectively), and they reported more nicotine withdrawal symptoms during smoking abstinence, with a significantly greater likelihood of endorsing anger/irritability and trouble concentrating. No group differences were evident for cigarettes per day or other indicators of nicotine dependence (e.g., FTND). Although it is unclear whether having weight problems during childhood contributes directly to smoking initiation, our results provide evidence that childhood weight problems may serve as a marker for earlier smoking experimentation and may also complicate cessation efforts due to its association with elevated withdrawal symptomatology. Future longitudinal studies with prospective measures of weight, dieting, and smoking initiation may be helpful in establishing causal pathways in different subgroups of smokers.
Keywords: childhood, weight problems, smoking, nicotine withdrawal, weight concerns, dieting
A number of studies suggest that weight concerns are associated with the onset of cigarette smoking (Tomeo, Field, Berkey, Colditz & Frazier, 1999). In particular, dieting behaviors, disordered eating symptoms, and weight concerns are most strongly associated with smoking initiation by female adolescents (French, Perry, Leon & Fulkerson, 1994; Potter, Pederson, Chan, Abut & Koval; 2004).
Furthermore, among adolescents, frequent consumption of high fat “junk food” (OR=1.6) is a risk factor for smoking initiation and, interestingly, being overweight is a risk factor for continued smoking during adolescence (OR = 3.5; O’Loughlin, Paradis, Renaud, & Sanchez Gomez, 1998). Little is known, however, about the possible impact of childhood weight problems on smoking history and patterns in adults. To explore this issue, we studied overweight adult women smokers to determine whether age of onset of weight problems might differentially impact smoking patterns. We hypothesized that women reporting childhood onset of weight problems would report earlier initiation of smoking and greater severity of nicotine dependence and associated symptoms.
Method
Participants
Data were compiled from women smokers recruited to participate in four nicotine research studies focused on weight, body image, and food intake. Informed consent was obtained for collection of baseline data, and individuals who did not qualify for subsequent participation in a laboratory experiment were paid for completing the questionnaire battery. For the present report, we analyzed data from the subsample of 89 women who participated in these studies who were currently overweight (Body Mass Index, BMI ≥25). We compared those who reported first experiencing weight problems (or perceiving themselves to be overweight) before Junior High School (n=22) with those who recalled first experiencing weight problems during Junior High School or later (n=67).
Participants had a mean age of 35.5 years (SD. = 9.9) and had completed a mean of 13.9 years of college (SD. = 2.5); 80.9% of respondents were Caucasian. Demographic and weight-related characteristics of the sample are presented in Table 1.
Table 1.
Characteristics of study participants
| Childhood Onset n=22 | Later Onset n=67 | p | |
|---|---|---|---|
| Age | 32.9 (1.8) | 36.4 (1.2) | ns |
| Education | 14.3 (0.5) | 13.8 (0.3) | ns |
| Race (% Caucasian) | 77.3% | 82.1% | ns |
| Age 1st had weight problem | 7.9 (0.9) | 22.4 (1.3) | n/a (grouping variable) |
| Current BMI | 36.9 (2.0) | 29.6 (0.5) | .001 |
| Depression (CES-D Score) | 15.3 (2.0) | 13 (1.3) | ns |
| Anxiety (STAI-Trait Score) | 42.1 (2.0) | 41.5 (1.5) | ns |
Data are presented as M (SEM) or percentages, as appropriate
Procedures
At baseline, all women completed the Weight & Dieting History questionnaire (from Dr. Marcus’ laboratory), which retrospectively assesses history of weight change, weight loss attempts, perception of being overweight, binge eating, and weight of family members. All women also completed the Centers for Epidemiologic Studies of Depression Scale (CES-D; Radloff, 1977), the Speilberger Trait Anxiety Scale (STAI-T; Speilberger et al., 1983) and the University of Michigan Smoking History Questionnaire (which assesses onset, duration, quantity, and frequency of smoking, nicotine dependence, and withdrawal symptoms; it also includes the Fagerstrom Test of Nicotine Dependence, or FTND; Heatherton et al., 1991).
Data Analysis
The Weight & Dieting History questionnaire queries weight status (extremely underweight, underweight, normal weight, overweight, and extremely overweight) during preschool, elementary school, junior high school, high school, and beyond. Those who reported being overweight or extremely overweight during preschool or elementary school and persistently thereafter (junior high school, high school, and currently) were categorized as having Childhood Onset of weight problems. Those who were currently overweight but who reported becoming so only during junior high school or later were classified as Later Onset.
Note that a variety of onset and offset patterns are not captured by this algorithm. For example, someone who reported being overweight during childhood, normal weight during high school, and overweight currently would not be classified. Because these various patterns were each of low frequency (including remitted childhood weight problems, n=4), these groups are not included in this report.
Throughout this report, we refer to our age of onset variable as being onset of “weight problems” rather than “obesity” or “overweight” because these retrospective data could not be verified; it is possible that some women who recalled being overweight during childhood may have been normal weight but perceived themselves to be overweight. Therefore, we restrict the term “overweight” or “obesity” to references to current BMI, which was more reliably assessed.
Childhood and Later Onset groups were compared on mood, anxiety, weight- and smoking-related variables using t-tests and Chi-square analyses as appropriate. In addition, supplemental analyses of covariance (ANCOVA) of significant variables, controlling for current BMI, were also conducted.
Results
Compared to the Later Onset group, the Childhood Onset group had a significantly higher mean BMI (t[23.4]=3.6, p<.001, see Table 1). Women in the Childhood Onset group were significantly more likely to be currently obese (i.e., BMI ≥30; 73% vs. 39%, χ2= 7.6, df=1, p<.01) and to have a history of binge eating (59% vs. 34%, χ2= 4.2, df=1, p<.05).
Women with Childhood Onset weight problems reported first trying cigarettes at a significantly younger age than those with Later Onset (M (SEM) of 13.0 (.68) vs. 14.9 (.45) years of age, respectively, t[86]=− 2.3, p<.05). Women with Childhood Onset weight problems reported more nicotine withdrawal symptoms during smoking abstinence (M (SEM) of 3.7 (.59) vs. 2.4 (.29) years of age, respectively, t[87]= −2.1, p<.05; See Table 1), with a significantly greater likelihood of endorsing anger/irritability (72% vs. 42%, χ2= 4.9, df=1, p<.05) and trouble concentrating (61% vs. 27%, χ2= 6.6, df=1, p=.01; See Table 2). No group differences were evident for cigarettes per day or other indicators of nicotine dependence (e.g., FTND).
Because the study groups differed on current BMI (See Table 1), which might have some bearing on withdrawal symptomatology (but, presumably, not age of first experimentation with cigarettes), a supplemental ANCOVA was conducted, with weight problem onset group as the factor, number of withdrawal symptoms as the dependent variable, and BMI as the covariate. This yielded a marginally significant model F(2,86)=2.2, p=.113 in which the BMI covariate was nonsignificant, and the group effect approached significance (p=.052) ,
Discussion
Overweight women smokers with childhood-onset weight problems experimented with smoking at an earlier age than those with later-onset of becoming overweight. Although the groups did not differ on nicotine dependence, women with childhood-onset of weight problems reported greater severity of smoking withdrawal symptomatology, with a greater likelihood of anger/irritability and trouble concentrating and marginally greater likelihood of impatience/irritability and depression/sadness when abstaining from smoking. Thus, our hypothesis that the onset of weight problems during childhood would be differentially associated with smoking behavior was, by and large, supported.
Our finding that those with Childhood Onset of weight problems were more likely to be overweight/obese in adulthood is consistent with other reports in the literature regarding the impact of childhood obesity on adult outcomes (e.g., Magarey, Daniels, Boulton, & Cockington, 2003). Our finding that the Childhood Onset group was more likely to binge eat, however, suggests that our Childhood and Adult onset groups may be qualitatively or diagnostically distinct, and that binge eating -- possibly that which begins in childhood or early adolescence -- may be the more important marker for smoking initiation. Our data do not permit further exploration of this intriguing possibility. Improved understanding of the relationships among weight history, binge eating, and smoking, however, may clarify the clinical implications of our findings. Interestingly, in related research, it has recently been suggested that binge eating and smoking may serve common functions with respect to modulation of affect and anxiety (White & Grillo, 2006).
Because overweight children share some risk factors with those at risk for smoking initiation (e.g., adverse peer influences, mood problems; Swallen et al., 2005; Janssen et al., 2004), it is perhaps not surprising that our participants with childhood onset of weight problems began experimenting with smoking at a significantly younger age than those who became overweight later in life. Longitudinal studies of larger and more diverse samples, with prospective measures of weight, dieting, and smoking initiation, may aid in establishing causal pathways in different subgroups of smokers. Ideally, future studies will include samples large enough to permit structural equation modeling and path analytic approaches that can tease apart the direct and indirect contributions of childhood weight problems to subsequent smoking behavior. Likewise, more detailed assessment of childhood weight problems in the context of clinical trials may be helpful in determining the extent to which childhood-onset may complicate cessation by virtue of its association with elevated withdrawal symptomatology.
The present study, despite the limitations inherent in retrospective assessment, is the first to our knowledge to identify differences among overweight women smokers as a function of the onset of weight problems. Our findings suggest that taking this variable into account may yield information of potential value in the prevention and treatment of smoking in women.
Figure 1.
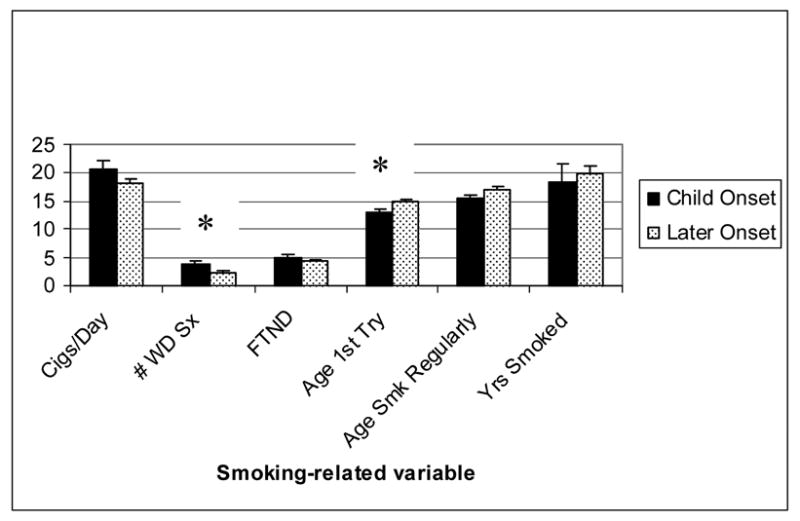
Smoking Behavior by Childhood versus Later Onset of Weight Problem
*p<.05 for Age 1st Try (“age first tried a cigarette”) and # WD Sx (Number of withdrawal symptoms during most recent period of abstinence)
Figure 2.
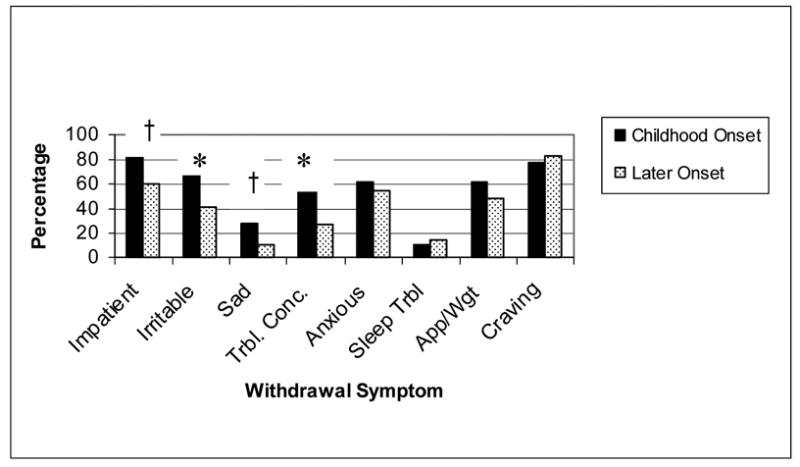
Withdrawal Symptoms on Quit Attempts for childhood versus Later Onset of Weight Problems
*p<.05 for Irritable (“angry, irritable, or frustrated”) and Trbl. Conc. (“trouble concentrating”)
†p<.10 (trend) for Impatient (“restless or impatient”) and Sad (“depressed, low, or sad mood”)
Acknowledgments
Preparation of this manuscript was supported by a grant from the National Heart Lung & Blood Institute to Dr. Pomerleau (HL52981) and by a grant from the National Institute on Drug Abuse to Drs. Marcus and Levine (R01 DA04174). Data presented in this manuscript were included in a preliminary report presented at the Annual Meeting of the Society for Research on Nicotine and Tobacco (SRNT, February, 2006).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Fagerström KO. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict Behav. 1978;3:235–41. doi: 10.1016/0306-4603(78)90024-2. [DOI] [PubMed] [Google Scholar]
- French SA, Perry CL, Leon GR, Fulkerson JA. Weight concerns, dieting behavior, and smoking initiation among adolescents: A prospective study. Am J Public Health. 1994;84:1818–1820. doi: 10.2105/ajph.84.11.1818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addiction. 1991;86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- Janssen I, Craig WM, Boyce WF, Pickett W. Associations between overweight and obesity with bullying behaviors in school-aged children. Pediatrics. 2004;113:1187–1194. doi: 10.1542/peds.113.5.1187. [DOI] [PubMed] [Google Scholar]
- Magarey AM, Daniels LA, Boulton TJ, Cockington RA. Predicting obesity in early adulthood from childhood and parental obesity. Int J Obes Relat Metab Disord. 2003;27 doi: 10.1038/sj.ijo.0802251. [DOI] [PubMed] [Google Scholar]
- O’Loughlin J, Paradis G, Renaud L, Sanchez Gomez L. One-year predictors of smoking initiation and of continued smoking among elementary schoolchildren in multiethnic, low-income, inner-city neighbourhoods. Tob Control. 1998;7:268–275. doi: 10.1136/tc.7.3.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Potter BK, Pederson LL, Chan SS, Abut JA, Koval JJ. Does a relationship exist between body weight, concerns about weight, and smoking among adolescents? An integration of the literature with an emphasis on gender. Nicotine Tob Res. 2004;6:397–425. doi: 10.1080/14622200410001696529. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. [Google Scholar]
- Speilberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press; 1983. [Google Scholar]
- Swallen KC, Reither EN, Haas SA, Meier AM. Overweight, obesity, and health-related quality of life among adolescents: The National Longitudinal Study of Adolescent Health. Pediatrics. 2005;115:340–347. doi: 10.1542/peds.2004-0678. [DOI] [PubMed] [Google Scholar]
- Tomeo CA, Field AE, Berkey CS, Colditz GA, Frazier AL. Weight concerns, weight control behaviors, and smoking initiation. Pediatrics. 1999;104:918–924. doi: 10.1542/peds.104.4.918. [DOI] [PubMed] [Google Scholar]
- White MA, Grilo CM. Psychiatric comorbidity in binge-eating disorder as a function of smoking history. J Clin Psychiatry. 2006;67:594–599. doi: 10.4088/jcp.v67n0410. [DOI] [PubMed] [Google Scholar]