

Abstract
Objectives. We evaluated a previously reported association between residence in a damp and moldy dwelling and the risk of depression and investigated whether depression was mediated by perception of control over one’s home or mold-related physical illness.
Methods. We used survey data from 8 European cities. A dampness and mold score was created from resident- and inspector-reported data. Depression was assessed using a validated index of depressive symptoms.
Results. Dampness or mold in the home was associated with depression (odds ratio [OR]=1.39, 1.44, and 1.34, for minimal, moderate, and extensive exposure, respectively, compared with no exposure). This association became attenuated when perception of control (OR=1.34, 1.40, and 1.24; global P=.069) or a physical health index (OR = 1.32, 1.37, and 1.15; global P= .104) was included in the model. The mediation effects of perception of control over one’s home and by physical health appeared to be additive.
Conclusions. Dampness and mold were associated with depression, independent of individual and housing characteristics. This association was independently mediated by perception of control over one’s home and by physical health.
Little is known regarding pathways between housing conditions and mental health.1 Studies have found independent associations between general housing quality, at both the neighborhood and individual levels, with psychological distress2 and depression.3–5 Dose–response associations have been found between the number of housing problems and residents’ emotional problems6 and between the degree of housing improvement and alleviation of psychological distress.7 Several specific housing characteristics, including overcrowding,8–10 noise,11,12 indoor air quality,13 housing type,7 and floor level1,14 have also been associated with residents’ mental health.
We studied a less intuitive association, that of damp and moldy conditions within a dwelling and depressive symptoms. Molds are fungi that are found in many environments but grow best in warm, damp, and humid conditions.15 Therefore, dwellings that have problems with dampness also commonly have problems with mold. Although the physical health sequelae of residence in a damp and moldy dwelling have been relatively well investigated,15–17 the effect of living in such an environment on mental health has not.
Two studies that used both objective and subjective measures of dampness and mold produced results showing associations with depression and with reports of emotional distress.18,19 Residence in damp housing was also linked with reported problems with physical energy, sleep, and social isolation.20 However, these studies did not include multivariate analyses. Of the 3 studies that included multivariate analyses, 2 found independent associations between residence in damp and moldy housing and mental distress,21,22 but the third did not.23
Investigators have hypothesized that the psychological and financial stress of keeping a house clean in the face of recurrent mold may result in a degree of anxiety or depression.18,21 Housing is inextricably linked to one’s perception of control.24 Individuals faced with high demands but low control experience elevated risk of anxiety and depression.25,26 Thus, a sense of high demand and compromised control over one’s living environment may mediate a potential link between residence in a damp and moldy dwelling and depression. Perception of control has been studied in the context of crowding and noise within a home10,11,27 but not with respect to dampness and mold growth.
Physical health is another likely mediator of the potential link between residence in a damp and moldy dwelling and risk of depression. Residence in a damp and moldy dwelling is linked with poor physical health outcomes, including respiratory problems,17 asthma,16,18 diarrhea,18 nausea,28 and headaches.20 Such recurring conditions may be associated with anxiety and depression, thus mediating the potential association between exposure to dampness or mold and depression.
All extant studies of dampness or mold and mental health have been conducted in the United Kingdom. Methodological shortcomings of some of these studies make it difficult to convincingly assert an association between dampness and mold and mental health. Moreover, the hypothesized pathways through which dampness and mold may lead to psychological symptoms are unsubstantiated. Our study advances the field in 3 ways: (1) we examined whether the reported association between dampness and mold and depressive symptoms could be replicated in areas outside the United Kingdom, (2) we accounted for a larger number of individual and housing characteristics than was previously possible, and (3) we examined whether the individuals’ perception of control over their housing conditions and their mold-related physical health mediate a possible association between dampness and mold and depressive symptoms.
METHODS
Study Sample and Measures
The Large Analysis and Review of European Housing and Health Status (LARES) project was a cross-sectional survey on place of residence, housing conditions, and health conducted by the World Health Organization.29–31 This survey was carried out in 8 European cities (Angers, France; Bonn, Germany; Bratislava, Slovakia; Budapest, Hungary; Ferreira do Alentejo, Portugal; Forli, Italy; Geneva, Switzerland; and Vilnius, Lithuania) in 2002 and 2003. The participant sample in each city was randomly generated from resident registries, the local tax registry, or the national health insurance registry.32 The number of residents sampled reflected city size and expected participation rate.
Once a residence was selected for the LARES survey, a trained interviewer visited that household to conduct the survey. The survey included a questionnaire on housing conditions (administered only to the resident who received the surveyor), a self-completed health questionnaire (administered to all the residents of the dwelling), and the interviewer’s own assessment of the conditions of the home and the immediate environment. Response rates varied across cities. For example, in Forli, Italy, 50% of the households participated and 96% of residents of those households completed the health questionnaire; by contrast, the corresponding figures in Vilnius, Lithuania, were 63% and 83%, respectively.32
The main outcome for our study was depressive symptoms, measured by an index based on the presence of 4 symptoms of depression (sleep disturbance, decreased interest in activities, low self-esteem, and decreased appetite) during the 2 weeks prior to the interview.33 Respondents with 3 or 4 self-reported depressive symptoms were classified (and are referred to here) as depressed. This measure correlates highly with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria for major depression.33,34 A secondary outcome was the respondents’ report of whether a physician had diagnosed anxiety or depression in the 12 months preceding the interview.
We computed a dampness and mold index for each dwelling, based on both respondent and surveyor data. Both the respondent and the interviewer indicated whether there were problems with mold or dampness in the dwelling, in which rooms these problems occurred, and to what extent. Self-reported and interviewer data were moderately correlated (Spearman correlation = 0.58) and were combined with equal weight in an overall index that ranged from 0 to 100. A discrete measure of dampness and mold exposure with 4 levels (none, minimal, moderate, and extensive) was then computed and used in the analyses. In the analyses, we controlled for city of residence, survey respondent characteristics (age, gender, marital status, education, employment, smoking, and environmental tobacco smoke at home), and housing characteristics (ownership, size, tenure, crowding, ventilation, natural light, and heating).
We evaluated 2 potential mediators of the association between exposure to dampness or mold and depression. Perception of control over one’s home was based on respondents’ answer to the statement “I feel in control of my home,” measured on a 5-point Likert scale (reverse coded). In addition, an index of physical health was created by summing the presence of 6 conditions that can be related to mold exposure (cold or throat illness, wheezing, asthma attack, other respiratory problems, fatigue, and headache), determined by whether the respondent reported receiving such a diagnosis from a physician within the 12 months preceding the interview. This list of conditions was derived from literature on health effects of mold exposure.15
The distinction between variables considered to be confounders and those considered to be mediators is in their causal role and interpretation. In confounding, the exposure and the confounder are correlated because the former is a causal consequence of the latter or because the 2 variables share a common cause. For example, in this study, the amount of natural light in a dwelling could be considered to be a confounder. This is because lack of light is both a determinant of mold growth and an independent risk factor for depressive symptoms. A reduction of the effect of dampness or mold on depression because of adjustment for light is interpreted as eliminating bias.
In mediation, the exposure and the mediator are also correlated, but the mediator is in the causal pathway from exposure to outcome (i.e., direction of causation is from exposure to mediator to outcome). For example, it is known that mold can contribute to or exacerbate certain physical health conditions, and physical health is also known to influence the development of depressive symptoms. A reduction in the effect of dampness or mold on depression because of adjustment for mold-related health is interpreted as the indirect dampness or mold effect. If, after adjustment, a dampness or mold effect still remains, it can be interpreted as an independent (direct) effect that does not involve that specific mediator.
Statistical Analyses
We analyzed data only for adult LARES respondents (aged 18 years or older). We used logistic regression to model depression as a function of dampness or mold exposure and other individual and housing variables. Because multiple residents were surveyed in many dwellings, we used a generalized estimating equations (GEE) approach, using the robust (sandwich) variance estimator to account for possible clustering. GEEs typically use the correlation coefficient to quantify the correlation between outcomes. However, in our analyses, we used the alternating logistic regression method,35 a GEE variation that uses the odds ratio (OR) instead of the correlation coefficient, because the former is a more appropriate measure of association between dichotomous outcomes. We fit 4 multivariable models that included the following variables: (1) only mold and covariates; (2) mold, covariates, and perception of control; (3) mold, covariates, and mold-related physical health conditions; and (4) mold, covariates, perception of control, and mold-related physical health conditions.
We estimated the relative mediation effect as the proportion of the dampness or mold effect on depression that was accounted for by a potential mediator36:
where RME is the relative mediation effect, ORunadjusted denotes the estimated OR for dampness or mold from the model that did not include any mediators (total effect, model 1), and ORadjusted denotes the corresponding OR from the model that included 1 or both mediators (direct effect, models 2–4). Several methods for testing and construction of confidence intervals for the RME have been proposed.37,38 Because these were not yet fully developed, we chose to use the bootstrap (percentile method, with 1000 re-samples) method.39 All analyses were conducted in SAS version 8.2 (SAS Institute Inc, Cary, NC).
RESULTS
LARES data were available for 6919 adults aged 18 years or older. We excluded 225 respondents with missing data on depression or dampness and mold, 258 with missing data on either perception of control or physical health status, and 554 who had no data on 1 or more covariates. Therefore, the analyses we present are based on data for 5882 adult respondents from 2982 households (range = 1–7 respondents per household). The fraction of missing data was relatively higher for Ferreira do Alentejo, Portugal, and lower for Bratislava, Slovakia. Compared with the analysis sample, the excluded respondents included older individuals (particularly, those aged older than 70 years), as well as persons with low levels of education, persons who were unemployed or retired, and persons who were without heat in any of their rooms. Prevalence of dampness or mold and depression was also somewhat higher in the excluded data (52% had some dampness or mold in the home, compared with 43% in the analysis sample, and 11% were classified as depressed, compared with 9% in the analysis sample).
Table 1 ▶ presents a detailed summary of the study sample characteristics. Respondents were aged between 18 and 104 years (median = 46), the numbers of men and women were similar, and most had at least a secondary education (typically 12 years of school). The majority of respondents (57%) lived in homes with no dampness or mold; 526 (9%) respondents reported 3 or 4 depressive symptoms. All individual and housing characteristics shown in Table 1 ▶ were significantly associated with depression in univariable analyses (P< .01). Both perception of control and mold-related physical health were strongly associated with mold in univariable analyses, as were all 6 individual conditions that composed the physical health index (all P values < .001).
TABLE 1—
Characteristics of the Study Sample from 8 European Cities: Large Analysis and Review of European Housing and Health Status, 2002–2003
| Total, No. (%) | Depression Prevalence, % | |
| Dampness or mold in homea | ||
| None | 3371 (57.3) | 6.5 |
| Minimal | 833 (14.2) | 9.7 |
| Moderate | 926 (15.7) | 11.6 |
| Extensive | 752 (12.8) | 15.8 |
| City of residence | ||
| Angers, France | 587 (10.0) | 4.4 |
| Bonn, Germany | 584 (10.0) | 2.7 |
| Bratislava, Slovakia | 707 (12.0) | 8.2 |
| Budapest, Hungary | 766 (13.0) | 11.8 |
| Ferreira do Alentejo, Portugal | 666 (11.3) | 23.3 |
| Forli, Italy | 806 (13.7) | 5.5 |
| Geneva, Switzerland | 468 (8.0) | 4.3 |
| Vilnius, Lithuania | 1298 (22.0) | 9.0 |
| Age, y | ||
| 18–29 | 1410 (24.0) | 6.4 |
| 30–39 | 1000 (17.0) | 6.3 |
| 40–49 | 1115 (19.0) | 9.0 |
| 50–59 | 978 (16.6) | 10.3 |
| 60–69 | 735 (12.5) | 8.7 |
| ≥ 70 | 644 (10.9) | 16.8 |
| Gender | ||
| Men | 2712 (46.1) | 6.9 |
| Women | 3170 (53.9) | 10.7 |
| Marital status | ||
| Married | 3943 (67.0) | 8.8 |
| Separated/divorced/widowed | 721 (12.3) | 14.6 |
| Single | 1218 (20.7) | 6.1 |
| Educationb | ||
| Primary | 1148 (19.5) | 16.6 |
| Secondary | 3054 (51.9) | 8.7 |
| Postsecondary | 1680 (28.6) | 4.2 |
| Employment | ||
| Employed outside the home | 3031 (51.5) | 6.4 |
| Not employed outside the home | 626 (10.5) | 13.9 |
| Student | 519 (8.8) | 4.1 |
| Retired | 1459 (24.8) | 13.7 |
| Other | 247 (4.2) | 9.3 |
| Smoking | ||
| Noc | 3976 (67.6) | 8.7 |
| Occasionally | 651 (11.1) | 7.2 |
| 5–15 cigarettes/day | 694 (11.8) | 8.1 |
| > 15 cigarettes/day | 561 (9.5) | 14.1 |
| Environmental tobacco smoke in the home | ||
| No | 3995 (67.9) | 7.6 |
| Yes | 1887 (32.1) | 11.8 |
| Home ownership | ||
| Own | 4379 (74.4) | 9.6 |
| Rent | 1503 (25.6) | 7.1 |
| Home size, m2 | ||
| 0–49 | 825 (14.0) | 11.4 |
| 50–99 | 3301 (56.1) | 8.6 |
| 100–149 | 1398 (23.8) | 9.4 |
| ≥150 | 358 (6.1) | 4.5 |
| Duration of residency, y | ||
| 0–10 | 2389 (40.6) | 6.6 |
| 11–20 | 1433 (24.4) | 9.2 |
| > 20 | 2060 (35.0) | 11.5 |
| Crowding, no. of residents per room | ||
| < 0.50 | 1739 (29.6) | 8.3 |
| 0.51–1.00 | 3157 (53.7) | 7.8 |
| > 1.00 | 986 (16.7) | 13.7 |
| Ventilation | ||
| No | 2300 (39.1) | 10.4 |
| Yes, forced | 1226 (20.8) | 6.9 |
| Yes, free | 2356 (40.1) | 8.7 |
| Natural lightd | ||
| Enough | 4501 (76.5) | 8.0 |
| Not enough | 1381 (23.5) | 12.0 |
| Heating | ||
| In all rooms | 4638 (78.9) | 6.5 |
| Not in all rooms | 1244 (21.1) | 17.9 |
| Perception of controle | ||
| Strongly agree | 1991 (33.8) | 7.6 |
| Agree | 2193 (37.3) | 7.5 |
| Neither agree nor disagree | 1038 (17.6) | 12.0 |
| Disagree | 529 (9.0) | 11.0 |
| Strongly disagree | 131 (2.2) | 20.6 |
| Mold-related physical health, no. of conditions | ||
| 0 | 3347 (56.9) | 5.8 |
| 1 | 1574 (26.8) | 8.6 |
| 2 | 592 (10.1) | 15.9 |
| 3–6 | 369 (6.3) | 28.2 |
aSelf-reported and interviewer-observed data were combined with equal weight in an overall index that ranged from 0 to 100. A discrete measure of dampness and mold exposure with 4 levels (none, minimal, moderate, and extensive) was then computed and used in the analyses.
bIncludes exsmokers and never smokers.
cDepending on the country, a completed primary education is 4 to 6 years of schooling and a completed secondary education is 9 to 10 years of schooling.
dBased on self-reports.
ePerception of control was measured on a 5-point scale (higher scores correspond to perceiving less control).
Results from multivariable analyses are shown in Table 2 ▶. The first model included 3 categories for dampness or mold as well as individual and housing characteristics. As a whole, mold in the home was significantly associated with depressive symptoms (global P value = .032). Inclusion of perception of control attenuated the association between mold and depressive symptoms (model 2, P= .069), and perception of control itself was highly significant (P= .001). Inclusion of the physical health index also attenuated the association between mold and depressive symptoms (model 3, P= .104), particularly the effect of the highest levels of exposure. The physical health index itself was significant (P= .001). Finally, inclusion of both mediators substantially attenuated the association between mold and depressive symptoms (model 4, P= .215); both mediators remained significant (P= .001 for both). The attenuation of the estimated log ORs between the models without and with a mediator represents the relative mediation effects (Table 3 ▶).
TABLE 2—
Multivariate Logistic Regression Results for Depression in 4 Models, With and Without Mediators: Large Analysis and Review of European Housing and Health Status, 2002–2003
| Model 1, No Mediators, OR (95% CI) | Model 2,Perception of Control, OR (95% CI) | Model 3,Mold-Related Physical Health, OR (95% CI) | Model 4,Both Mediators, OR (95% CI) | |
| Dampness or molda | ||||
| Minimal vs none | 1.39 (1.02, 1.89) | 1.34 (0.98, 1.82) | 1.32 (0.98, 1.79) | 1.28 (0.94, 1.74) |
| Moderate vs none | 1.44 (1.08, 1.92) | 1.40 (1.05, 1.87) | 1.37 (1.02, 1.83) | 1.34 (1.01, 1.79) |
| Extensive vs none | 1.34 (0.97, 1.85) | 1.24 (0.90, 1.72) | 1.15 (0.83, 1.61) | 1.09 (0.78, 1.52) |
| Age (10-y increment) | 1.12 (1.01, 1.24) | 1.13 (1.02, 1.25) | 1.11 (1.00, 1.23) | 1.12 (1.01, 1.24) |
| Gender (Female vs male) | 1.62 (1.33, 1.98) | 1.64 (1.34, 2.00) | 1.43 (1.17, 1.76) | 1.44 (1.17, 1.78) |
| Crowding, no. of residents per room | ||||
| 0.51–1.00 vs ≤0.50 | 1.10 (0.84, 1.46) | 1.01 (0.77, 1.34) | 1.08 (0.82, 1.43) | 1.00 (0.76, 1.33) |
| > 1.00 vs ≤0.50 | 1.81 (1.26, 2.60) | 1.55 (1.07, 2.26) | 1.78 (1.24, 2.56) | 1.55 (1.07, 2.25) |
| Natural lightb (Not enough vs enough) | 1.31 (1.04, 1.66) | 1.28 (1.01, 1.61) | 1.19 (0.94, 1.51) | 1.16 (0.92, 1.47) |
| Perception of controlc (1-point increment) | 1.28 (1.16, 1.41) | 1.26 (1.14, 1.38) | ||
| Mold-related physical healthd (1-point increment) | 1.52 (1.40, 1.64) | 1.51 (1.39, 1.63) | ||
Note. OR = odds ratio; CI = confidence interval. All models also included city of residence, marital status, education, employment, smoking status, environmental tobacco smoke exposure at home, home ownership, home size, duration of tenure, crowding, ventilation, and type of heating in home.
aSelf-reported and interviewer-observed data were combined with equal weight in an overall index that ranged from 0 to 100. A discrete measure of dampness and mold exposure with 4 levels (none, minimal, moderate, and extensive) was then computed and used in the analyses.
bBased on self-reports.
cPerception of control was measured on a 5-point scale (higher scores correspond to perceiving less control).
dThe mold-related physical health index was a summation of 6 conditions (cold or throat illness, wheezing, asthma attack, other respiratory problems, fatigue, and headache).
TABLE 3—
Mediation Effects of Perception of Control and Mold-Related Physical Health for the Association Between Dampness and Mold and Depression: Large Analysis and Review of European Housing and Health Status, 2002–2003
| Perception of Controla | Mold-Related Physical Healthb | Both Mediators | ||||
| RME, % | P | RME, % | P | RME, % | P | |
| Dampness/mold | ||||||
| Minimal vs none | 12 | .037 | 15 | .109 | 26 | .041 |
| Moderate vs none | 6 | .101 | 13 | .126 | 19 | .054 |
| Extensive vs none | 26 | .068 | 52 | .074 | 71 | .072 |
Note. RME = relative mediation effect.
aPerception of control was measured on a 5-point scale (higher scores correspond to perceiving less control).
bThe mold-related physical health index was a summation of 6 conditions (cold or throat illness, wheezing, asthma attack, other respiratory problems, fatigue, and headache).
Across all 4 models, the effects of most of the covariates changed little. In the final model, age (P= .040), gender (P= .001), education (P= .006), employment (P= .001), environmental tobacco smoke (P= .009), and crowding (P= .001) were all significant.
Our results did not change materially when perception of control was modeled as a dichotomous variable or with multiple indicator terms, or when mold-related health status was included as a dichotomous variable (results not shown). Comparable results were also obtained when depression was defined as physician-diagnosed chronic anxiety or depression in the past 12 months, as reported by survey participants.
There was wide variability in the geographic and weather conditions across the 8 survey cities. For example, relative average humidity ranged between 65% in Ferreira do Alentejo, Portugal, and 81% in Angers, France, and Vilnius, Lithuania. The prevalence of any mold ranged from 26% in Bratislava, Slovakia, to 81% in Ferreira do Alentejo, Portugal, and the prevalence of depression ranged from 3% in Bonn, Germany, to 23% in Ferreira do Alentejo, Portugal (see the figure available as an online supplement at http://apha.org). Figure 1 ▶ is a graph of the association (ORs) between dampness and mold and depression (model 1, no mediator) across the 8 cities. Although the mold effects were stronger in Geneva, Switzerland, and Bonn, Germany, than in the other cities, the overall association between dampness and mold and depression appeared relatively homogeneous (P= .151 for the city-by-mold interaction).
FIGURE 1—
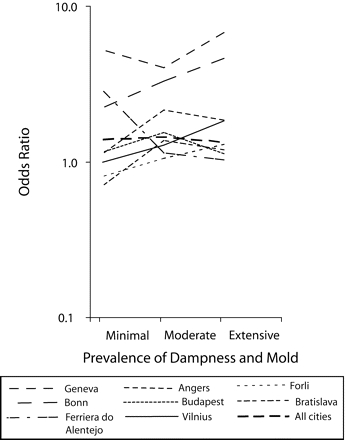
Estimated odds ratios of association between dampness or mold and depression: Large Analysis and Review of European housing and Health Status Study, Angers, France; Bonn, Germany; Bratislava, Slovakia; Budapest, Hungary; Ferreira do Alentejo, Portugal; Forli, Italy; Geneva, Switzerland; and Vilnius, Lithuania, 2002–2003.
Note. The depression index is derived from 4 measures: sleep disturbance, decreased interest in activities, low self-esteem, and decreased appetite
DISCUSSION
To our knowledge, we conducted the first study outside of the United Kingdom to examine the association between residence in a damp or moldy dwelling and depressive symptoms. In line with previous work, we found that older individuals, women, and unemployed respondents were more likely to report depressive symptoms than were younger individuals, men, and employed respondents, respectively. We also found a positive association between crowded conditions at the home (specifically, more than 1 resident per room) and risk of depression. Our findings are also consistent with earlier reports of a link between housing conditions and mental health,1–3,5–14 specifically an association between dampness and mold and depression.18–21 This association was independent of several key correlates of housing conditions and depression.
However, such an association may not be causal, but rather attributable to residual confounding by variables that were either assessed with error or not measured in our study. For example, socioeconomic status was assessed through self-reports and likely involved some misclassification. In view of the moderate strength of the association between dampness and mold and depression, it is important that future studies pay special attention to accurate measurement of depression risk factors that are correlated with housing conditions. This is particularly timely, because evidence is accruing that mental health outcomes are as relevant to housing conditions as are physical health outcomes.
Our results suggest that perception of control over one’s housing environment may partially mediate the association between residence in a damp or moldy dwelling and depression. This is consistent with extensive evidence linking perception of control with health40 as well as with previously described causal models of a robust link between low control and bouts of depression.25,41 An individual’s physical health, particularly chronic respiratory problems, seems to represent a slightly stronger mediator of the association between exposure to a damp or moldy housing environment and depression.
The mediation effects of perception of control and physical health appeared to be additive in our study. The joint mediation effects by these 2 variables approximately equaled the sum of their individual mediation effects (Table 3 ▶). We suspect that such additivity may indicate that the 2 variables lie on 2 distinct causal pathways that link dampness and mold in the home and depression. Future methodological work on the assessment and interpretation of joint mediation effects of 2 or more factors would be very useful in this context. However, even with the 2 mediators we have not accounted for the entire association between mold and depressive symptoms. This suggests the possibility of a direct pathologic effect of mold exposure. Recent reports of a link between residence in damp and moldy dwellings and cognitive impairment, including depression, give some credence to this hypothesis.42–47 Exposure to toxigenic molds may dysregulate emotions through a hypoactivation of the frontal cortex.42 However, a causal association has not been established and any neurological effects of mold are likely to be compounded by the stress of chronic illness (from mold) and the stress of dealing with mold.44,45
The cross-sectional design of our study does not allow inference regarding causality. A reverse-causality scenario, in which depression is the causal agent, is also consistent with our results. Although earlier works argue against the hypothesis that those in emotional dire straits drift toward poor housing,48–50 it is possible that depressed individuals tend to their home in a manner that allows mold growth. Longitudinal studies are needed to investigate the relative strength of this explanation and those supported by our results. We emphasize that these explanations are not mutually exclusive.
We used detailed self-reported and interview data to construct an index of dampness or mold exposure. Although this index was not intended as a measure of long-term exposure, most respondents had lived in the same home for more than 10 years, and the dampness and mold score is intended to reflect more than a transient mold growth. Although this index probably captured current dampness and mold conditions in the home fairly accurately, it may not necessarily reflect a long-term exposure. In addition, we measured depression with a validated index of depressive symptoms that correlate well with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria.33,34 Nevertheless, because this index relies on self-reported depressive symptoms without independent verification, it likely results in some degree of misclassification. However, another measure of depression, physician diagnosis in the past 12 months, showed very similar associations with exposure to dampness or mold.
A strength of our study is its relatively large and diverse sample. Previous research focused primarily on residents of areas known for housing problems.18,19,21,23 In contrast, the LARES data were obtained from a wide range of neighborhoods in 8 different cities. Although the 8 cities are quite diverse in geography, weather, culture, and a host of individual and housing variables, the association between dampness and mold and depression was relatively homogeneous, suggesting good generalizability of our findings.
Our study underscores the importance of housing conditions as determinants of mental health and the importance of housing as a medium for universal health promotion efforts.51 Our findings suggest that damp or moldy housing conditions are linked to a moderately elevated risk of depression. Future research should seek to confirm whether this link is causal and, if so, to what extent it is mediated by perception of control or physical health. If the association proves to be causal, the mechanism will likely involve the psychological and physiological consequences of living in poor housing conditions and potentially a direct pathological effect of mold.
Acknowledgments
We are grateful to Xavier Bonnefoy of the World Health Organization for supporting this study by providing data from the Large Analysis and Review of European Housing and Health Status. We also thank Richard Reading and Allison Kelsey for their valuable comments on earlier versions of the article.
Human Participant Protection This study entailed secondary analysis of data and did not require approval from Brown Medical School’s institutional review board.
Peer Reviewed
Contributors E.D. Shenassa originated the study, contributed to the data analysis plan, and cowrote the article. C. Daskalakis conceived the data analysis plan, analyzed the data, contributed to the conceptual development of the study, and cowrote the article. A. Liebhaber contributed to data analysis and article development. M. Braubach contributed to the development of the Large Analysis and Review of European Housing and Health Status instruments and provided feedback regarding various aspects of the survey. M.J. Brown contributed to the conceptual development of the study.
References
- 1.Evans GW, Wells N, Moch A. Housing and mental health: a review of the evidence and methodological and conceptual critique. J Soc Issues. 2004;59:475–500. [Google Scholar]
- 2.Kearns RA, Smith CJ. Housing stressors and mental health among marginalised urban populations. Area. 1993;25:267–278. [Google Scholar]
- 3.Ellaway A, Macintyre S. Does housing tenure predict health in UK because it exposes people to different levels of housing related hazards in the home or its surroundings? Health Place. 1998;4:141–150. [DOI] [PubMed] [Google Scholar]
- 4.Galea S, Ahern J, Rudenstine S, Wallace Z, Vlahov D. Urban built environment and depression: a multilevel analysis. J Epidemiol Community Health. 2005;59: 822–827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Evans GW. Saltzman H, Cooperman JL. Housing quality and children’s socioemotional health. Environ Behav. 2001;33:389–399. [Google Scholar]
- 6.Hunt SM. Emotional distress and bad housing. Health Hyg. 1990;11:72–79. [Google Scholar]
- 7.Evans GW, Wells NM, Chan HE, Saltzman H. Housing quality and mental health. J Consult Clin Psychol, 2000;68:526–530. [DOI] [PubMed] [Google Scholar]
- 8.Braubach M, Bonnefoy XR. Housing and health: the Eastern European challenge. Open House Int. 2001; 26:8–22. [Google Scholar]
- 9.Cox VC, Paulus PB, McCain G. The relationship between crowding and health. In: Baum A, Singer JE, eds. Advances in Environmental Psychology. Vol. 4. Hillsdale, NJ: Erlbaum; 1982:271–290.
- 10.Gove WR, Hughes M, Galle OR. Overcrowding in the home: an empirical investigation of its possible pathological consequences. Am Sociol Rev. 1979;44:59–80. [PubMed] [Google Scholar]
- 11.Hatfield J, Job RF, Hede AJ, et al. Human response to environmental noise: the role of perceived control. Int J Behav Med. 2002;9:341–359. [DOI] [PubMed] [Google Scholar]
- 12.Cohen S, Krantz DS, Evans GW, Stokols D. Community noise, behavior, and health: the Los Angeles noise project. In: Baum A, Singer JE, eds. Advances in Environmental Psychology. Vol. 4. Hillsdale, NJ: Erlbaum; 1982:295–317.
- 13.Evans GW. The built environment and mental health. J Urban Health. 2003;80(4):536–555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gillis AR. High-rise housing and psychological strain. J Health Soc Behav. 1977;18:418–431. [PubMed] [Google Scholar]
- 15.Institute of Medicine. Damp Indoor Spaces and Health. Washington, DC: National Academies Press; 2004. [PubMed]
- 16.Zock JP, Jarvis D, Luczynska C, Sunyer J, Burney P. Housing characteristics, reported mold exposure, and asthma in the European Community Respiratory Health Survey. J Allergy Clin Immunol, 2002;110:285–292. [DOI] [PubMed] [Google Scholar]
- 17.Dales RE, Burnett R, Zwanenburg H. Adverse health effects among adults exposed to home dampness and molds. Am Rev Respir Dis. 1991;143:505–509. [DOI] [PubMed] [Google Scholar]
- 18.Hyndman SJ. Housing dampness and health amongst British Bengalis in east London. Soc Sci Med. 1990;30:131–41. [DOI] [PubMed] [Google Scholar]
- 19.Martin CJ, Platt SD, Hunt SM. Housing conditions and ill health. BMJ (Clin Res Ed). 1987;294:1125–1127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Packer CN, Stewart-Brown S, Fowle SE. Damp housing and adult health: results from a lifestyle study in Worcester, England. J Epidemiol Community Health. 1994;48:555–559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hopton JL, Hunt SM. Housing conditions and mental health in a disadvantaged area in Scotland. J Epidemiol Community Health. 1996;50:56–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Platt S, Martin C, Hunt S. The mental health of women with children living in deprived areas of Great Britain: the role of living conditions, poverty and unemployment. In: Goldberg D, Tantam D, eds. The Public Health Impact of Mental Disorder. Toronto, Ontario: Hogrefe and Huber; 1990.
- 23.Platt SD, Martin CJ, Hunt SM, Lewis CW. Damp housing, mould growth, and symptomatic health state. BMJ. 1989;298:1673–1778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dunn JR, Hayes MV. Social inequality, population health, and housing: a study of two Vancouver neighborhoods. Soc Sci Med. 2000;51:563–587. [DOI] [PubMed] [Google Scholar]
- 25.Griffin JM, Fuhrer R, Stansfeld SA, Marmot M. The importance of low control at work and home on depression and anxiety: do these effects vary by gender and social class? Soc Sci Med, 2002;54:783–798. [DOI] [PubMed] [Google Scholar]
- 26.Shenassa ,, ED. Society, physical health and modern epidemiology. Epidemiology. 2001;12:467–470. [DOI] [PubMed] [Google Scholar]
- 27.Baum A, Singer JE, Baum CS. Stress and the environment. In: Evans GW, ed. Environmental Stress. Cambridge, England: Cambridge University Press; 1982: 15–44.
- 28.Hunt SM, McKenna SP. The impact of housing quality on mental and physical health. Housing Rev. 1992;41:47–49. [Google Scholar]
- 29.World Health Organization. Large Analysis and Review of European Housing and Health Status (LARES): Preliminary Overview. Copenhagen, Denmark: WHO; 2007. Also available at: http://www.euro.who.int/Housing/activities/20020711_1. Accessed March 13, 2007.
- 30.Bonnefoy XR, Braubach M, Moissonnier B, Monolbaev K, Robbel N. Housing and health in Europe: preliminary results of a pan-European study. Am J Public Health. 2003;93:1559–1563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shenassa ED, Liebhaber A, Ezeamama A. Perceived safety of area of residence and exercise: a pan-European study. Am J Epidemiol. 2006;163:1012–1017. [DOI] [PubMed] [Google Scholar]
- 32.World Health Organization, Regional Office for Europe. Data on the representativeness of the LARES samples. Available at: www.euro.who.int/housing/activities/20041221_1. Accessed March 13, 2007.
- 33.Brody DS, Hahn SR, Spitzer DS, et al. Identifying patients with depression in the primary care setting: a more efficient method. Arch Intern Med. 1998;158: 2469–2475. [DOI] [PubMed] [Google Scholar]
- 34.Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Association; 1994.
- 35.Carey VC, Zeger S, Diggle PJ. Modelling multivariate binary data with alternating logistic regressions. Biometrika. 1993;80:517–526. [Google Scholar]
- 36.Freedman LS, Graubard BI, Schatzkin A. Statistical validation of intermediate endpoints for chronic diseases. Stat Med. 1992;11:167–178. [DOI] [PubMed] [Google Scholar]
- 37.Freedman LS. Confidence intervals and statistical power of the “validation” ratio for surrogate or intermediate endpoint. J Stat Plan Inference. 2001;96:143–153. [Google Scholar]
- 38.Li Z, Meredith MP, Hoseyni MS. A method to assess the proportion of treatment effect explained by a surrogate endpoint. Stat Med. 2001;20:3175–3188. [DOI] [PubMed] [Google Scholar]
- 39.Efron B, Tibshirani RJ. An Introduction to the Bootstrap. London, England: Chapman & Hall; 1993.
- 40.Bandura A. Self-Efficacy: The Exercise of Control. New York, NY: WH Freeman; 1997.
- 41.Brown GW, Moran PM. Single mothers, poverty and depression. Psychol Med. 1997;27:21–33. [DOI] [PubMed] [Google Scholar]
- 42.Crago BR, Gray MR, Nelson LA, Davis M, Arnold L, Thrasher JD. Pscyhological, neuropsychological, and electrocortical effects of mixed mold exposure. Arch Environ Health. 2003;58:452–463. [DOI] [PubMed] [Google Scholar]
- 43.Gordon WA, Cantor JB, Johanning E, et al. Cognitive impairment associated with toxigenic fungal exposure: a replication and extension of previous findings. Appl Neuropsychol. 2004;11:65–74. [DOI] [PubMed] [Google Scholar]
- 44.Kilburn KH. Indoor mold exposure associated with neurobehavioral and pulmonary impairment: a preliminary report. Arch Environ Health. 2003;58: 390–398. [DOI] [PubMed] [Google Scholar]
- 45.Baldo JV, Ahmad L, Ruff R. Neuropsychological performance of patients following mold exposure. Appl Neuropsychol. 2002;9:193–202. [DOI] [PubMed] [Google Scholar]
- 46.Sudakin DL. Toxigenic fungi in a water-damaged building: an intervention study. Am J Ind Med. 1998; 34:183–190. [DOI] [PubMed] [Google Scholar]
- 47.Rea WJ, Didriksen N, Simon TR, Pan Y, Fenyves EJ, Griffiths B. Effects of toxic exposure to molds and mycotoxins. Arch Environ Health. 2003;58:399–405. [DOI] [PubMed] [Google Scholar]
- 48.Shenassa ED, Stubbendick A, Brown MJ. Social disparities in housing and related pediatric injury: a multilevel study. Am J Public Health. 2004;94:633–639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Reading R, Langford IH, Haynes R, Lovett A. Accidents to preschool children: comparing family and neighbourhood risk factors. Soc Sci Med. 1999;48: 321–330. [DOI] [PubMed] [Google Scholar]
- 50.Haynes R, Reading R, Gale S. Household and neighbourhood risks for injury to 5–14 year old children. Soc Sci Med. 2003;57:625–636. [DOI] [PubMed] [Google Scholar]
- 51.Shenassa ED. Delivering the goods: the importance of screening accuracy for effective community intervention and prevention. J Community Psychol. 2002; 30:197–210. [Google Scholar]