

Abstract
Trends in cocaine use over the past 2 decades were compared across levels of education in a population-based US sample of adults. Significant inverse associations between educational achievement and cocaine use after 1990 were driven by dramatic decreases in persistent cocaine use among more highly educated adults, whereas persistent cocaine use remained relatively unchanged among those who did not finish high school. This emerging health disparity highlights the need for improved interventions that target persistent cocaine users with low educational achievement.
There has been a dramatic decrease in the prevalence of cocaine use over the past 2 decades.1–5 Few studies have examined changing disparities in cocaine use among individuals of varying educational achievement. Associations with lower individual educational achievement6 and lower parental educational achievement have been reported in recent cross-sectional studies of cocaine use.7 Miech et al. report an inverse association between current cocaine use and individual educational achievement over time,8 but the nature of this changing association remains relatively unexplored.
Current disparities in cocaine use may be attributable to increased use by those with lower educational achievement or decreased use by those with higher educational achievement, or both. The high price of powder cocaine in the early 1980s restricted its use,9 but after 1985, there was an epidemic-like growth in the prevalence of the cheaper alternative, crack,10–13 mostly in impoverished urban areas.14–16 Soon after, highly publicized cocaine-related deaths increased the perception of risk associated with cocaine use,9,14,17 and the perception of risk was inversely related to cocaine use.18 We examined the emergence of this inverse association between cocaine use and educational achievement over time through analyses of the past 2 decades of the National Survey on Drug Use and Health (NSDUH).
METHODS
We used data from the 1979–2002 NSDUH (formerly known as the National Household Survey on Drug Abuse) to investigate cocaine use and educational achievement among adults aged 19–50 years. Educational achievement was stratified into 3 categories: non–high school graduate, high school graduate, and college graduate. Past-year cocaine use (powder, crack, free base, and coca paste), was divided into recent-onset19–24 and persistent23 use. Recent-onset users reported first usage within 24 months of the interview; persistent users reported use in the past year and first usage more than 24 months before the interview.
We estimated smoothed functions of cocaine use over time using application of generalized additive models, which are graphical scatter plot smoothers that allow for non-linearities in the data and the sharing of data between neighboring data points.25,26 Multivariable logistic regression analyses were conducted within, not between, survey years to provide the relative odds of cocaine use among adults with higher educational achievement as compared with adults with lower educational achievement. We used models to control for the potential confounding effects of demographics (gender, race, and age). Inverse probability survey weights and variance adjustments27–43 were applied to regression models with Stata version 8.0 (StataCorp, College Station, Tex).
RESULTS
The proportion of recent-onset cocaine use diminished steadily for all levels of educational achievement (Figure 1 ▶). From 1979 to 1982, the relative odds of recent-onset cocaine use were significantly greater for college and high school graduates versus non–high school graduates (odds ratio [OR] range = 1.8–2.6; P < .05). These differences narrowed significantly, and throughout the 1990s the proportion of recent-onset cocaine use was rare within each level of educational achievement (range = 0.2%–0.5%).
FIGURE 1—
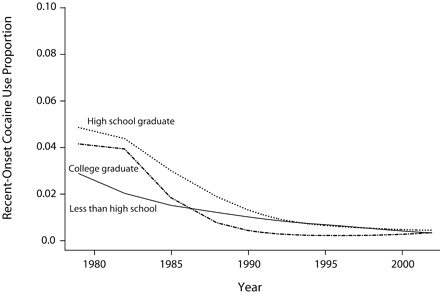
Weighted proportion of US adults aged 19–50 years who reported recent-onset (i.e., within the past 24 months) cocaine use between 1979 and 2002, by educational attainment level: National Survey on Drug Use and Health.
Non–high school graduates had a relatively constant proportion of persistent cocaine use over all survey years (Figure 2 ▶). By contrast, the proportion of persistent cocaine use among college graduates peaked in 1982 (OR = 1.9; 95% confidence interval [CI] = 0.8, 4.4) and then dramatically decreased and fell below that of non–high school graduates from 1990 to 2002 (OR range = 0.2–0.5; P< .05). High school graduates behaved similarly to college graduates in terms of persistence of cocaine use.
FIGURE 2—
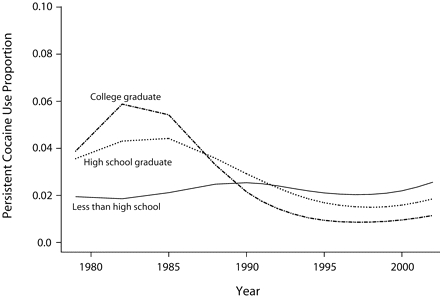
Weighted proportion of US adults aged 19–50 years who reported persistent cocaine use between 1979 and 2002, by educational attainment level: National Survey on Drug Use and Health.
DISCUSSION
Our findings indicated an inverse association between cocaine use and educational achievement. This association was attributable to both dramatic decreases in the persistence of use among adults with high educational achievement and the relatively constant persistence of use among adults with low educational achievement. It is of interest that recent-onset cocaine use steadily decreased over time and remained relatively rare among adults regardless of their level of educational achievement. These results could not be explained by changes in the demographic (race or gender) distribution within levels of education over time. Potential biases in results include misclassification of some college students as being only high school graduates as well as potential measurement error associated with self-reported drug use.44,45
Our results are consistent with Link and Phelan’s “fundamental causes of disease” framework, which suggests that as unhealthy behaviors are identified, people of higher educational achievement better understand the risks and have more resources to engage in protective efforts and modify behavior.46 This framework is supported by studies on smoking behavior that were conducted after the 1960s when individuals of high socioeconomic status were more likely to quit smoking because of known risks47,48 and less likely to suffer coronary heart disease49 than were those of low socioeconomic status. The persistent use of cocaine among non–high school graduates may reflect a lower perception of risks or, more likely, a difference in trends of adopting new behaviors to benefit their health compared with those with higher education. In relation to health disparities and public health, these results highlight the need for improved intervention programs that target adults with lower levels of educational achievement who persist in their cocaine use, not just the prevention of first use.
Acknowledgments
This research was supported by the National Institute on Drug Abuse (training grant T32DA07292).
The authors express their gratitude to Richard Miech, who offered comments on earlier drafts of the article.
Human Participant Protection No protocol approval was needed for this research. The National Survey on Drug Use and Health is a publicly available data set with no personal identifiers.
Peer Reviewed
Contributors V. S. Harder was the lead researcher on this study, conducted all analyses, and wrote all drafts of the article. H. D. Chilcoat was research adviser during the conception of the research questions, assisted with the study as it progressed, and offered critiques on all article drafts.
References
- 1.Abelson HI, Miller, JD. A decade of trends in cocaine use in the household population. In: Kozel NJ and Adams EH, eds. Cocaine Use in America: Epidemiologic and Clinical Perspectives. NIDA Research Monograph 61, DHHS No. (ADM) 85–1414. 1985;35–49. [PubMed]
- 2.Anthony JC. Epidemiological research on cocaine use in the USA. Ciba Found Symp. 1992;166:20–33. [PubMed] [Google Scholar]
- 3.Trinkoff AM, Ritter C, Anthony JC. The prevalence and self-reported consequences of cocaine use: an exploratory and descriptive analysis. Drug Alcohol Depend. 2001;26:217–225. [DOI] [PubMed] [Google Scholar]
- 4.Bachman J, O’Malley P, Schulenberg J, Johnston L, Bryant A, Merline A. The decline of substance use in young adulthood: Changes in social activities, roles, and beliefs. Mahwah, NJ: Lawrence Erlbaum Associates, Inc; 2002.
- 5.Secondary school students. Bethesda, Md; National Institutes of Health; 2004. NIH Publication No. 04–5507.
- 6.Chatterji P. Illicit druguse and educational attainment. Health Econ. 2006;15:489–511. [DOI] [PubMed] [Google Scholar]
- 7.Goodman E, Huang B. Socioeconomic status, depressive symptoms, and adolescent substance use. Arch Pediatr Adolesc Med. 2002;156:448–453. [DOI] [PubMed] [Google Scholar]
- 8.Miech RA, Chilcoat H, Harder VS. The increase in the association of education and cocaine use over the 1980s and 1990s: evidence for a “historical period” effect. Drug Alcohol Depend. 2005;79:311–320. [DOI] [PubMed] [Google Scholar]
- 9.Grinspoon L, Bakalar JB. Cocaine: A Drug and Its Social Evolution. Rev. ed. New York, NY: Basic Books, Inc; 1985.
- 10.Johnson BD. The crack era in New York City. Addict Recovery. 1991:24–27.
- 11.Johnson BD, Lewis C, Golub A. Crack onset in the 1980s in New York City. In: Vamos P, Corriveau PJ, eds. Drugs and Society to the Year 2000; Proceedings of the XIV World Congress of Therapeutic Communities. Montreal, Canada: Portage Program for Drug Dependencies, Inc. 1992;365–369.
- 12.Cornish JW, O’Brien CP. Crack cocaine abuse: an epidemic with many public health consequences. Annu Rev Public Health. 1996;17:259–273. [DOI] [PubMed] [Google Scholar]
- 13.Cohn V. Crack use. NIDA Notes. 1986;4:6–7. [Google Scholar]
- 14.Fagan J, Chin K. Initiation into crack and cocaine: A tale of two epidemics. Contemp Drug Probl. 1989;16: 579–617. [Google Scholar]
- 15.Hamid A. The political economy of crack-related violence. Contemp Drug Probl. 1990;17:31–79. [Google Scholar]
- 16.Williams T. Crackhouse: Notes From the End of the Line. Reading, Mass: Addison-Wesley Publishing Co; 1992.
- 17.Waldorf D, Reinarman C, Murphy S. Cocaine Changes: The Experience of Using and Quitting. Philadelphia, Pa: Temple University Press; 1991.
- 18.Bachman JG, Johnston LD, O’Malley PM. Explaining the recent decline in cocaine use among young adults: further evidence that perceived risks and disapproval lead to reduced drug use. J Health Soc Behav. 1990;31:173–184. [PubMed] [Google Scholar]
- 19.Chen CY, Anthony JC. Possible age-associated bias in reporting of clinical features of drug dependence: epidemiological evidence on adolescent-onset marijuana use. Addiction. 2003;98:71–82. [DOI] [PubMed] [Google Scholar]
- 20.Chen CY, Anthony JC. Epidemiological estimates of risk in the process of becoming dependent upon cocaine: cocaine hydrochloride powder versus crack cocaine. Psychopharmacology (Berl). 2004;172: 78–86. [DOI] [PubMed] [Google Scholar]
- 21.Storr CL, Zhou H, Liang KY, Anthony JC. Empirically derived latent classes of tobacco dependence syndromes observed in recent-onset tobacco smokers: epidemiological evidence from a national probability sample survey. Nicotine Tob Res. 2004;6:533–545. [DOI] [PubMed] [Google Scholar]
- 22.Anthony JC, Petronis K. Early-onset drug use and risk of later drug problems. Drug Alcohol Depend. 1995;40:9–15. [DOI] [PubMed] [Google Scholar]
- 23.O’Brien MS, Anthony JC. Risk of becoming cocaine dependent: epidemiological estimates for the United States, 2000–2001. Neuropsychopharmacology. 2005;30:1006–1018. [DOI] [PubMed] [Google Scholar]
- 24.Chen CY, O’Brien MS, Anthony JC. Who becomes cannabis dependent soon after onset of use? Epidemiological evidence from the United States: 2000–2001. Drug Alcohol Depend. 2005;79:11–22. [DOI] [PubMed] [Google Scholar]
- 25.Hastie TJ. Generalized additive models. In: Chambers JM and Hastie TJ, eds. Statistical Models in S. Pacific Grove, Calif: Wadsworth & Brooks/Cole; 1991:249–307.
- 26.Hastie TJ, Tibshirani RJ. Generalized Additive Models. London, England: Chapman and Hall; 1994.
- 27.National Institute on Drug Abuse. National Household Survey on Drug Abuse: Main Findings 1979. Rock-ville, Md: Department of Health and Human Services; 1980. DHHS publication 976.
- 28.National Institute on Drug Abuse. National Household Survey on Drug Abuse: Main Findings 1982. Rock-ville, Md: Department of Health and Human Services; 1983. DHHS publication 1263.
- 29.National Household Survey on Drug Abuse: Main Findings 1985. National Institute on Drug Abuse (NIDA). Rockville, MD: Department of Health and Human Services; 1988. DHHS publication 1586.
- 30.National Institute on Drug Abuse. National Household Survey on Drug Abuse: Main Findings 1988. Rock-ville, Md: Department of Health and Human Services; 1990. DHHS publication 1682.
- 31.National Institute on Drug Abuse. National Household Survey on Drug Abuse: Main Findings 1990. Rock-ville, Md: Department of Health and Human Services; 1991. DHHS publication 1788.
- 32.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1991. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1993. DHHS publication SMA 93–1980.
- 33.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1992. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1995. DHHS publication SMA 94–3012.
- 34.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1993. Rockville, MD: Office of Applied Studies, Department of Health and Human Services; 1995. DHHS publication SMA 95–3020.
- 35.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1994. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1996. DHHS publication SMA 96–3085.
- 36.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1995. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1997. DHHS publication SMA 97–3127.
- 37.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1996. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1998. DHHS publication SMA 98–3200.
- 38.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1997. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 1998. DHHS publication SMA 98–3250.
- 39.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1998. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 2000. DHHS publication SMA 00–3381.
- 40.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 1999. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 2000. DHHS publication SMA 00–3466.
- 41.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 2000. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 2001. DHHS publication SMA 00–3642.
- 42.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 2001. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 2002. DHHS publication SMA 00–3381.
- 43.Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings 2002. Rockville, Md: Office of Applied Studies, Department of Health and Human Services; 2003. DHHS publication SMA 00–3381.
- 44.Biemer PP, Wiesen C. Measurement error evaluation of self-reported drug use: a latent class analysis of the US National Household Survey on Drug Abuse. J R Statist Soc A. 2002;165:97–119. [Google Scholar]
- 45.Harrison L, Hughes A. The Validity of Self-Reported Drug Use: Improving the Accuracy of Survey Estimates. Rockville, Md: National Institute on Drug Abuse; 1997. [PubMed]
- 46.Link BG, Phelan J. Social conditions as fundamental causes of disease. J Health Soc Behav. 1995;Spec No: 80–94. [PubMed]
- 47.Ernster V. Trends insmoking, cancer risk, and cigarette promotion. Cancer. 1988;62:1702–1712. [DOI] [PubMed] [Google Scholar]
- 48.Novotny TE, Warner KE, Kendrick JS, Remington P. Smoking by blacks and whites: Socioeconomic and demographic differences. Am J Public Health. 1988;78: 1187–1189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Beaglehole R. International trends in coronary heart diseasemortality, morbidity, and risk factors. Epidemiol Rev. 1990;12:1–16. [DOI] [PubMed] [Google Scholar]