

Abstract
Aortic arch aneurysm, pseudocoarctation, and coronary artery stenosis are extremely rare in Behçet's syndrome. We present the case of a 25-year-old man with Behçet's syndrome who underwent coronary artery bypass grafting for severe stenosis in the proximal left anterior descending coronary artery and concomitant surgical correction of a saccular aneurysm that was causing pseudocoarctation of the aortic arch. The surgery was successful.
Key words: Aortic aneurysm, thoracic/complications/diagnosis/surgery; Behcet syndrome/complications/diagnosis/surgery; coronary artery bypass; coronary disease/diagnosis/etiology/surgery; coronary stenosis/etiology/surgery; vascular surgical procedures/methods
Behçet's syndrome is a systemic, generalized, chronic, inflammatory disorder that is characterized by aphthous stomatitis, genital ulcers, and ocular lesions. Another manifestation is extensive vasculitis of the arteries and veins.1 Arterial complications of Behçet's syndrome rarely affect the thoracic aorta, and coronary artery stenosis is also extremely uncommon.1,2 Herein, we report the case of a patient with Behçet's syndrome who underwent concurrent surgery for an aortic arch aneurysm, pseudocoarctation of the aorta, and coronary artery stenosis.
Case Report
In October 2005, a 25-year-old man with Behçet's syndrome was referred to our hospital for surgery to repair an aneurysm of the aortic arch. He had an acute anterior MI on the day of his admission. The patient had experienced rapidly progressive hoarseness; his only risk factor for cardiac disease, other than Behçet's, was smoking. The diagnosis of Behçet's syndrome had been made on the basis of the patient's oral aphtha, erythema nodosum, and a positive pathergy test. He had been undergoing systemic corticosteroid therapy. Coronary angiography showed 95% stenosis of the left anterior descending coronary artery (LAD). Computed tomographic angiography (Fig. 1) showed that a saccular aneurysm of the aortic arch was compressing the left subclavian artery and the distal aortic arch, forming a pseudocoarctation of the arch. The aneurysmal sac appeared to contain mural thrombus.
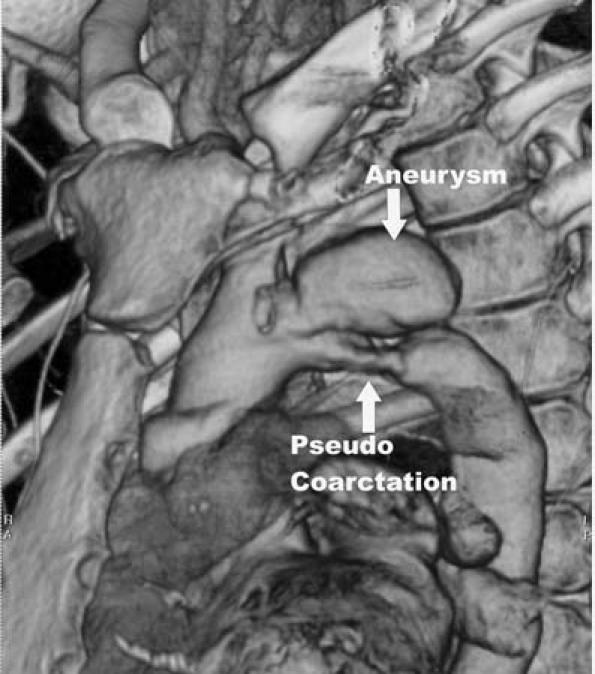
Fig. 1 Computed tomographic angiography shows the saccular aneurysm and the pseudocoarctation of the aortic arch.
The right upper brachial and right femoral arteries were cannulated before median sternotomy was performed. Upon opening, we encountered severe adhesions in the left pleuropericardial space. The left internal mammary artery had no pulse and appeared to be fibrotic due to the adhesions and the aneurysmal compression of the left subclavian artery. After cannulation of the superior and inferior venae cavae, distal anastomosis of the aorta–LAD bypass was performed on fibrillation by means of a saphenous vein graft and 8–0 Prolene sutures. The heart was then defibrillated, and the neck of the aneurysm was exposed via careful dissection. Because the surrounding aortic tissues were quite inflamed, meticulous care was taken to preserve the vagus and phrenic nerves. Retrograde femoral perfusion and selective antegrade cerebral perfusion from the upper brachial artery were initiated at flow rates of 2.5 to 3.5 L/(min·m2) and 600 cc/(min·m2), respectively. Cold blood cardioplegic solution was used to induce cardiac arrest. The aneurysm was opened; the effluent blood from the retrograde perfusion was suctioned from the distal arch and returned to the oxygenator. The neck of the aneurysm was resected, and a 28-mm preclotted woven Dacron graft was trimmed to form a patch. Aortoplasty was performed with use of 4–0 Prolene sutures in order to form a proper shape (Fig. 2). Before the aorta was closed, the air was removed carefully. The duration of selective antegrade cerebral perfusion was 40 minutes. During the combined aneurysmectomy and aortoplasty, the patient's rectal and septal temperatures were lowered to 18 °C and 5 °C, respectively. Total perfusion time was 230 min. The proximal anastomosis of the LAD graft was completed during the rewarming period.
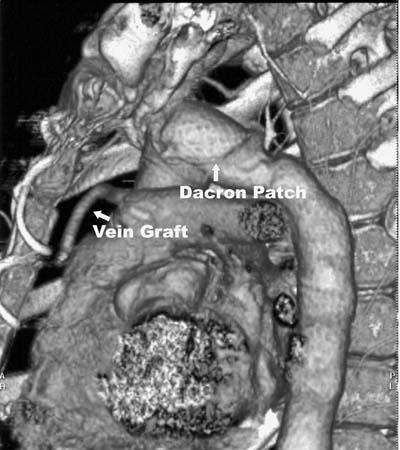
Fig. 2 Postoperative computed tomographic angiography shows the patch closure and the aorta–left anterior descending coronary artery bypass graft.
The patient's postoperative course was uneventful. Postoperative medical therapy consisted of cyclophosphamide, colchicine, prednisolone, aspirin, β-blocker, and valsartan. Twenty-two months after the operation, he was doing well, and no evidence of aneurysmal dilatation was observed on computed tomographic scans.
Discussion
Arterial involvement is a rare complication of Behçet's syndrome, and aneurysms, when they occur, are usually located in the abdominal aorta or in the femoral or pulmonary arteries.1 Thoracic aortic aneurysms are rare.2 Coronary aneurysms are more frequent than ste-notic lesions, and coronary artery disease is extremely uncommon in Behçet's syndrome. Coronary occlusion is attributed to fibrous intimal thickening as a result of local vasculitis.3 During coronary artery bypass grafting (CABG), the use of arterial grafts is recommended, as is the avoidance of aortic manipulation, in order to decrease the risk of pseudoaneurysmal formation.3,4 Some researchers recommend the use of free arterial grafts in these patients, due to the risk of left subclavian arteri-al occlusion after CABG.5 However, in our patient, we used a saphenous vein graft, because the left internal mammary artery—the usual conduit of choice— was nonfunctional due to the severe adhesions and the compression of the left subclavian artery by the aneurysm. Regardless of graft type, the surgical treatment of Behçet's patients is challenging, because the surgeon is handling fragile and inflamed coronary arteries.
The patch-closure technique for an aneurysm of the distal aortic arch in a Behçet's patient has been reported.2 The interposition of a Dacron tube graft is another appropriate method, except that closing a defect in the anterior wall of the aortic arch via patching is much easier. The use of a tube graft necessitates a separate anastomosis and longer suture lines, which can result in even more potential false-aneurysm sites in inflamed aortic tissue. We prefer the patch-closure technique because, after resection, a single patch with a suture line over the neck of a saccular aneurysm enables linear flow in this region.
Retrograde perfusion from the femoral artery is widely used during surgery on diseased aortas. However, this perfusion technique would have been ineffective in our patient because of the aneurysmally formed coarctation of the distal arch. Therefore, we provided cerebral protection by means of selective antegrade cerebral perfusion via the brachial artery. This is a safe and easy method to apply, and it circumvents the effects on the brain of low flow or total circulatory arrest.6 Either brachial/axillary or femoral artery cannulation permits unencumbered access to all of the ascending aorta and the aortic arch, and such cannulation also moves the perfusion cannula away from the diseased aortic segment.
Patients who have Behçet's syndrome should be closely monitored for vascular involvement. In the presence of angina pectoris or of an aneurysmal process, the possibility of coronary artery disease should be investigated, even in younger Behçet's patients. Moreover, when a patient has coronary artery disease, the entire arterial system should be scanned for aneurysmal dilatation. Meticulous outpatient follow-up is important in order to detect postoperative pseudoaneurysmal formation and to tailor the patient's medical therapy.
Footnotes
Address for reprints: Hasmet Bardakci, MD, Turkiye Yuksek Ihtisas Hastanesi, Kalp Damar Cerrahisi Klinigi, 06100 Sihhiye Ankara, Turkey. E-mail: hasmetbardakci@yahoo.com
References
- 1.Hirose H, Takagi M, Noguchi M, Miyagawa N, Narimatsu M, Yamada T, et al. Coronary revascularization and abdominal aortic aneurysm repair in a patient with Behcet's diseases. J Cardiovasc Surg (Torino) 1998;39:751–5. [PubMed]
- 2.Yasuura K, Ogawa Y, Sawazaki M, Matsuura A, Okamoto H, Seki A, et al. Successful resection of a distal aortic arch aneurysm in a patient with Behcet's disease using an “aortic no-touch” technique and hypothermic total-body retrograde perfusion. Thorac Cardiovasc Surg 1992;40:219–21. [DOI] [PubMed]
- 3.Song MH, Watanabe T, Nakamura H. Successful off-pump coronary artery bypass for Behcet's disease. Ann Thorac Surg 2004;77:1451–4. [DOI] [PubMed]
- 4.Ipek G, Omeroglu SN, Mansuroglu D, Kirali K, Uzun K, Sismanoglu M. Coronary artery bypass grafting in a 26-year-old man with total occlusion of the left main coronary artery related to Behcet disease. J Thorac Cardiovasc Surg 2001;122: 1247–9. [DOI] [PubMed]
- 5.Iyisoy A, Kursaklioglu H, Kose S, Yesilova Z, Ozturk C, Saglam K, Demirtas E. Acute myocardial infarction and left subclavian artery occlusion in Behcet's disease: a case report. Mt Sinai J Med 2004;71:330–4. [PubMed]
- 6.Tasdemir O, Saritas A, Kucuker S, Ozatik MA, Sener E. Aortic arch repair with right brachial artery perfusion. Ann Thorac Surg 2002;73:1837–42. [DOI] [PubMed]