

Abstract
Behçet's syndrome is a chronic multisystem disease that presents with recurrent oral and genital ulceration and recurrent uveitis. Cardiac involvement is an extremely rare manifestation of this disorder.
A 33-year-old man with Behçet's syndrome was admitted to our department with a history of cough, fever, chest pain, hemoptysis, and weight loss. Transthoracic and transesophageal echocardiography revealed a right ventricular thrombus. After 1 month of treatment with warfarin, cyclophosphamide, and corticosteroid, the intracardiac thrombus resolved.
Key words: Behcet's syndrome/complications/drug therapy; diagnosis, differential; echocardiography, transesophageal; heart ventricles/ultrasonography; immunosuppressive agents/therapeutic use; Mediterranean region/epidemiology; Middle East/epidemiology; thrombosis/etiology; vasculitis; warfarin/therapeutic use
Behçet's syndrome is recognized as a multisystem disorder that affects mainly young adults in Mediterranean, Middle Eastern, and Far Eastern countries. Because there is no laboratory test for Behçet's, diagnosis is very difficult; however, characteristic clinical features—such as orogenital aphtae, ocular and skin lesions, arthritis, and neurologic, gastrointestinal, vascular, and pulmonary symptoms—aid in diagnosis. Various cardiovascular manifestations, such as pancarditis, acute myocardial infarction, conduction system disturbances, and valvular diseases, have been reported but are rare. Intracardiac thrombus formation, as seen in our patient, is exceptional even among cardiovascular cases of Behçet's.1
We report a case of right ventricular thrombus that resolved completely under corticosteroid, cyclophosphamide, and oral anticoagulant therapy.
Case Report
In August 2004, a 33-year-old man who had previously received a diagnosis of Beh-çet's syndrome was admitted to our hospital with a 1-month history of cough, fever, chest pain, hemoptysis, and weight loss (10 kg). He had experienced thrombophlebitis in 2001, and again in 2003. His physical examination produced normal results, as did a pathergy test. The erythrocyte sedimentation rate was 97 mm/hr at the end of the 1st hour. Human leukocyte antigen B5 was present; D-dimer, fibrinogen, C-reactive protein, and complement 3 levels were at upper-normal limits, but the patient was negative for factor V Leiden, prothrombin mutation, anticardiolipin antibodies, antiendothelial cell antibodies, von Willebrand factor, and lupus anticoagulant. Protein C and S levels were within normal limits. Chest radiographic and electrocardiographic results were also normal. A bilateral lower-extremity ultrasonographic examination revealed normal arteries, but in the venous system there was wall thickening and luminal contraction secondary to the thrombophlebitis; venous flow was normal. Transthoracic and transesophageal echocardiography showed a right intraventricular thrombus of 25 × 14-mm diameter (Figs. 1A and B). A thoracic spiral computed tomographic scan showed a filling defect in the right pulmonary artery at the interlobar lung surfaces, which might have been caused by the thrombus.
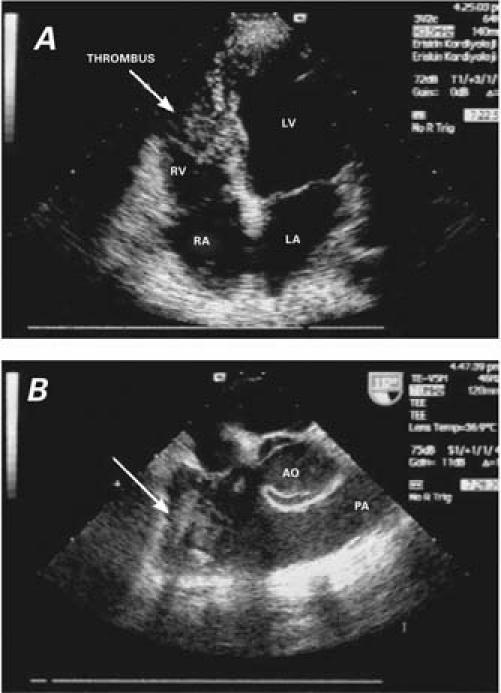
Fig. 1 The right intraventricular thrombus (arrow) is shown A) by transthoracic echocardiography (apical 4-chamber view) and B) by transesophageal echocardiography.
AO = aorta; LA = left atrium; LV = left ventricle; PA = pulmonary artery; RA = right atrium; RV = right ventricle
The patient was given immunosuppressive therapy: methylprednisolone (50 mg) daily and 750 mg/m2 cyclophosphamide monthly. In addition, warfarin was administered to keep the PT-INR (prothrombin time-internationalized ratio) at 2.5 or above. One month later, the right ventricular thrombus had disappeared on transthoracic and transesophageal echocardiography (Figs. 2A and B). The patient was still being monitored, without recurrence, 24 months later.
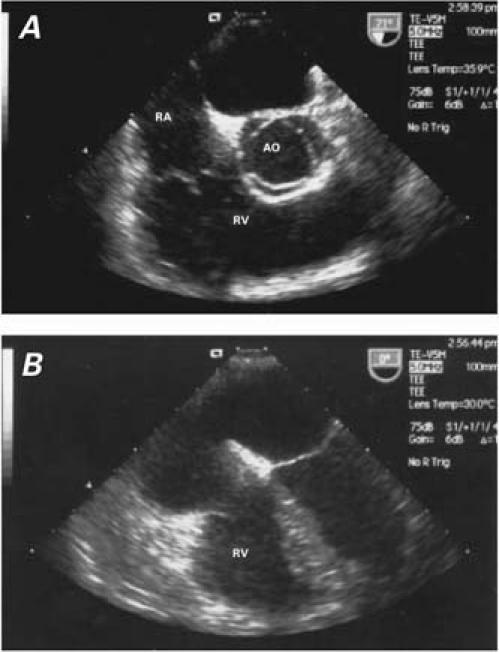
Fig. 2 One month after therapy, the thrombus has completely disappeared, as indicated by these transesophageal images (A and B).
AO = aorta; RA = right atrium; RV = right ventricle
Discussion
Cardiovascular involvement of Behçet's syndrome has ranged from 7% to 29% of reported cases.2 However, Ozkan and colleagues3 found that patients with Behçet's syndrome did not show a greater prevalence of echocardiographic abnormalities than did control subjects. Although intracardiac thrombi are known to be complications of vasculo-Behçet's (a variant of Behçet's), such thrombi are extremely rare. In 2000, Mogulkoc and associates1 reviewed all 25 cases that had been reported to date. In our search of the world medical literature, we found only 4 additional cases,4–7 not counting our own.
In the Mogulkoc review,1 surgery was performed in 12 patients but was unsuccessful in 4 of them. One patient had recurrence of an intracardiac thrombus after initial surgery and remained stable on warfarin after the 2nd surgical procedure. In 8 patients, anticoagulant or thrombolytic therapy was the 1st-line treatment. In 7, this approach was associated with complete resolution of the intracardiac thrombus, but the remaining patient had recurrence at 2 years. Two patients were treated with prednisone alone, with resolution of symptoms, but the outcomes were not recorded. Three patients received no specific therapy for intracardiac thrombus, because the thrombus was recognized only at autopsy. The reasons for death in this group were infection, massive hemoptysis, and pulmonary thromboembolism.
Gurgun and co-authors4 reported an unusual case characterized by mural cardiac thrombi in the right atrium and both ventricles, along with transient protein C and S deficiency. Goktekin and coworkers5 reported 1 case of intraventricular thrombus that recurred after surgical excision and was treated with methylprednisolone and cyclophosphamide; the patient died due to hepatic failure. Altunkeser's group6 reported a right atrial thrombus that recurred 3 months after resection; after 1 month of warfarin treatment, the recurrent thrombus disappeared. Baykan and colleagues7 reported the case of a young man whose intracardiac thrombi progressively resolved with cyclophosphamide and dexamethasone treatment. Our patient was treated successfully with methylprednisolone, cyclophosphamide, and warfarin.
The striking feature of nearly all Behçet's patients who have intraventricular thrombus is the prominent vascular involvement that defines the vasculo-Behçet's variant of the syndrome, which is observed in 3% to 46% of cases.8 Thrombophlebitis is the major feature of this variant. Arterial lesions are rare, but when they do occur, they carry a poor prognosis.
In conclusion, our patient had a large thrombus in the right ventricle, pulmonary emboli, and recurrent throm-bophlebitis. We suggest that Behçet's syndrome be kept in mind in the differential diagnosis of intracardiac thrombus. We also suggest the combination of methylprednisolone, cyclophosphamide, and warfarin as a good option to treat cardiac thrombi in patients who have Behçet's syndrome.
Footnotes
Address for reprints: Sait M. Dogan, MD, Zonguldak Karaelmas Universitesi, Tip Fakultesi, Kardiyoloji Anabilimdali, Kozlu 67600, Zonguldak, Turkey. E-mail: smdogan@yahoo.com
References
- 1.Mogulkoc N, Burgess MI, Bishop PW. Intracardiac thrombus in Behcet's disease: a systematic review. Chest 2000;118:479–87. [DOI] [PubMed]
- 2.Lie JT. Cardiac and pulmonary manifestations of Behcet syndrome. Pathol Res Pract 1988;183:347–55. [DOI] [PubMed]
- 3.Ozkan M, Emel O, Ozdemir M, Yurdakul S, Kocak H, Ozdogan H, et al. M-mode, 2-D and Doppler echocardiographic study in 65 patients with Behcet's syndrome. Eur Heart J 1992;13:638–41. [DOI] [PubMed]
- 4.Gurgun C, Sagcan A, Cinar CS, Yagdi T, Zoghi M, Tekten T, Kultursay H. Right atrial and ventricular thrombi in Behcet's disease: a case report and review of literature. Blood Coagul Fibrinolysis 2000;11:107–10. [PubMed]
- 5.Goktekin O, Korkmaz C, Timuralp B, Kudaiberdieva G, Gorenek B, Cavusoglu Y, et al. Widespread thrombosis asso-ciated with recurrent intracardiac masses in a patient with Behcet's disease. Int J Cardiovasc Imaging 2002;18:431–4. [DOI] [PubMed]
- 6.Altunkeser BB, Gormus N, Ozdemir K, Durgut K, Ozdemir A, Solak H, Gok H. A recurrent right atrial thrombus: a suggestive sign for Behcet's disease A case report. Heart Vessels 2002;16:196–7. [DOI] [PubMed]
- 7.Baykan M, Celik S, Erdol C, Baykan EC, Durmus I, Baha-dir S, et al. Behcet's disease with a large intracardiac thrombus: a case report. Heart 2001;85:E7. [DOI] [PMC free article] [PubMed]
- 8.Le Thi Huong D, Wechsler B, Papo T, Piette JC, Bletry O, Vitoux JM, et al. Arterial lesions in Behcet's disease. A study in 25 patients. J Rheumatol 1995;22:2103–13. [PubMed]