

A 68-year-old woman presented with chest pain and dyspnea. The results of physical examination and electrocardiography were within normal limits, but a posteroanterior chest radiograph revealed a mass in the upper mediastinum. Subsequent computed tomography (CT) and magnetic resonance imaging (MRI) revealed a dumbbell-shaped cyst surrounding the heart (Figs. 1 and 2). The cyst occupied a large space in the mediastinum and involved both sides of the chest. The portion of the cyst in the right paracardiac region was 9 × 12 × 13 cm; the portion in the left paracardiac region was 3 × 10 × 13 cm. Those 2 components of the cyst were joined to each other in front of the ascending aorta at the aorticopulmonary level. The cyst, thought to be pericardial, was removed by open thoracotomy. Histopathologic examination revealed that the cyst was lined with a single layer of cuboidal epithelium (Fig. 3) and was filled with clear fluid; accordingly, the preoperative diagnosis was confirmed.
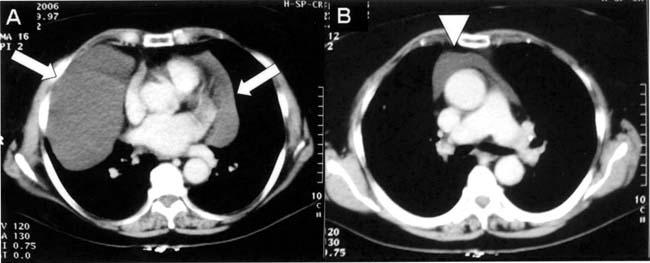
Fig. 1 Axial contrast-enhanced computed tomographic scans of the chest (mediastinal window) at the level of the left ventricle (A) and the aorticopulmonary window (B) show a non-enhanced, low-attenuated, well-circumscribed, dumbbell-shaped mass adjacent to the heart (arrows). Two components of the cyst are joined to each other in front of the ascending aorta (arrowhead) at the aorticopulmonary level.
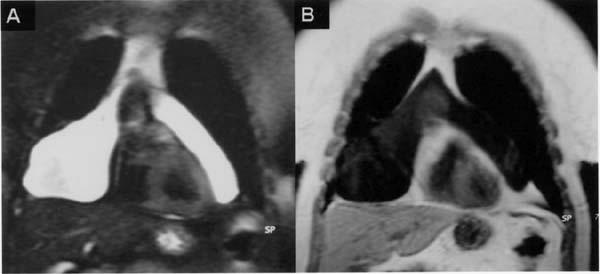
Fig. 2 Coronal magnetic resonance imaging scans show A) a hyperintense lesion on a fat-saturated T2*-weighted image, and B) a hypo-intense, non-enhancing lesion on a contrast-enhanced T1-weighted image, both consistent with a pericardial cyst.
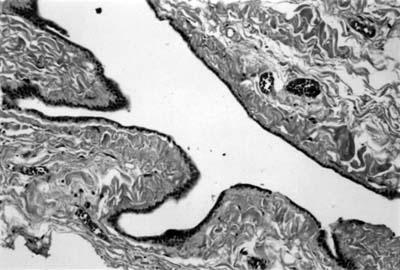
Fig. 3 Photomicrograph of a section of the cyst that is lined with single-layered cuboidal epithelium (H&E, orig. ×200).
Comment
Pericardial cysts, which constitute 11% of all mediastinal cysts,1 are usually asymptomatic and are detected incidentally. However, they can produce symptoms when they reach a large size. The most common symptoms of large cysts are retrosternal chest pain, dyspnea, and cough. Moreover, sequelae have been reported, such as cyst rupture, cardiac compression, atrial fibrillation, and even sudden death.2,3
Most pericardial cysts are situated at the right cardiophrenic angle; however, they can occur throughout the mediastinum. They are usually unilocular, well-marginated, spherical or teardrop-shaped cysts that may be attached to the pericardium directly or by a pedicle.4 Under histologic examination, pericardial cysts are seen to be lined with a single layer of mesothelial cells. Because these cysts are usually filled with a clear water-like fluid, they are sometimes called “springwater” cysts.
The imaging studies most useful for diagnosis are echocardiography, CT, and MRI. Transesophageal echocardiography is useful in showing the exact location of a pericardial cyst and in differentiating a cyst from other entities, such as a fat pad, ventricular aneurysm, aortic aneurysm, or solid tumor.5 On CT and MRI, a pericardial cyst typically appears as a non-enhanced, well-defined mass adjacent to the pericardium. The content is characterized by its water density on CT (range, 0–20 Hounsfield units) and signal intensity on MRI images (low intensity on T1-weighted, high on T2-weighted). Rarely, high signal intensity is seen on T1-weighted images, due to the high protein content of the cyst. Magnetic resonance imaging is more reliable than CT for the diagnosis of pericardial cysts, because on MRI it is possible to evaluate the lesion and its relationships with adjacent structures in several anatomic planes, without the need for contrast material.
Treatment is required in symptomatic patients or in those with an unclear diagnosis. In other patients, close follow-up is sufficient. Treatment options include surgical resection or percutaneous aspiration of the cyst.
A pericardial cyst should be suspected when a cystic lesion is detected in the mediastinum. A pericardial cyst can exist in various locations of the mediastinum and can take on unusual radiologic appearances, as in the case presented here.
Footnotes
Address for reprints: Ersin Ozturk, MD, GATA Haydarpasa Egitim Hastanesi, Radyoloji Servisi, Uskudar, Istanbul 34668, Turkey. E-mail: drersini@yahoo.com
References
- 1.Takeda S, Miyoshi S, Minami M, Ohta M, Masaoka A, Matsuda H. Clinical spectrum of mediastinal cysts. Chest 2003; 124:125–32. [DOI] [PubMed]
- 2.Vlay SC, Hartman AR. Mechanical treatment of atrial fibrillation: removal of pericardial cyst by thoracoscopy. Am Heart J 1995;129:616–8. [DOI] [PubMed]
- 3.Fredman CS, Parsons SR, Aquino TI, Hamilton WP. Sudden death after a stress test in a patient with a large pericardial cyst. Am Heart J 1994;127(4 Pt 1):946–50. [DOI] [PubMed]
- 4.Strollo DC, Rosado-de-Christenson ML, Jett JR. Primary mediastinal tumors: part II. Tumors of the middle and posterior mediastinum. Chest 1997;112:1344–57. [DOI] [PubMed]
- 5.Patel J, Park C, Michaels J, Rosen S, Kort S. Pericardial cyst: case reports and a literature review. Echocardiography 2004; 21:269–72. [DOI] [PubMed]