

A 49-year-old female was admitted to our hospital because of an acute anteroseptal wall myocardial infarction. The patient had no previous coronary artery or heart disease. Chest pain with radiation to the left shoulder associated with severe transpiration and nausea had been present since one hour before presentation. After transportation to the catheterisation laboratory she underwent a primary percutaneous coronary intervention (PCI) procedure of the left anterior descending coronary artery which was occluded after the first septal branch. A bare metal stent (Vision, Guidant) was implanted. The other coronary arteries showed no significant lesions.
After returning to the department the patient developed pain between her shoulder blades. Cardiac ultrasound showed severe wall motion abnormalities of the apical and anteroseptal segments. Because of the pain between her shoulder blades, additional cardiac ultrasound images were performed from a suprasternal view of the aortic arch showing signs of a possible ascending aortic dissection (figures 1 and 2).
Figure 1.
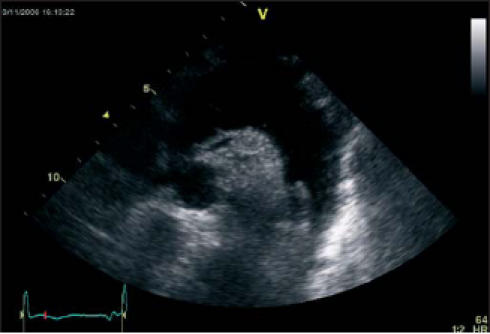
Cardiac ultrasound image of the aortic arch showing a possible dissection.
Figure 2.
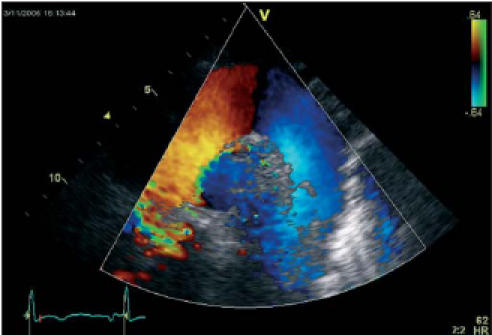
Cardiac ultrasound image with colour Doppler flow of the aortic arch showing flow in the false lumen.
An emergency CT angiogram of the thoracic aorta was performed. No aortic dissection was seen on the CT images. The only CT finding explaining the ultrasound images was the presence of a left coronary artery guiding catheter in the aortic arch (figures 3 and 4).
Figure 3.
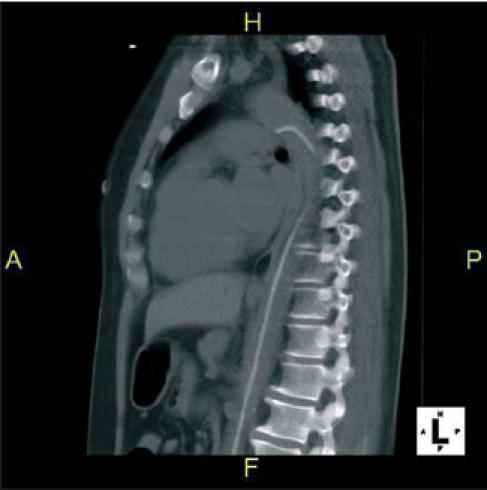
Saggital two-dimensional CT image showing the left coronary guiding catheter in the aortic lumen.
Figure 4.
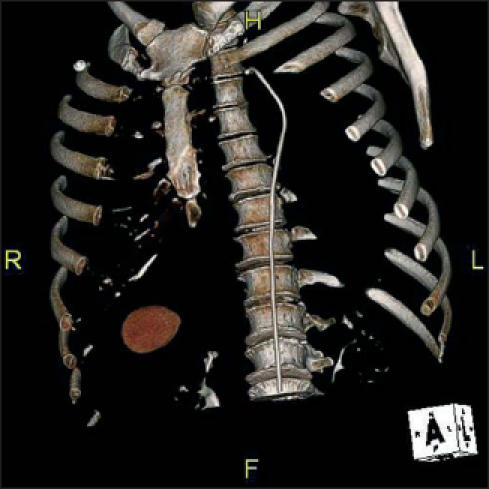
Three-dimensional CT reconstruction clearly showing the left coronary guiding catheter.
Dissection of the ascending aorta after a PCI procedure is a rare complication occurring in about 0.07% of patients,1 and after primary PCI in 0.19%.2 However, this complication is very lethal causing an in-hospital mortality of 20%3 so it is crucial that this diagnosis is not missed. Because of the new and severe back pain in this patient, additional ultrasound images of the aortic arch were performed and suggestive for aortic dissection. Fortunately, these images were created by a guiding catheter which was not pulled back far enough into the abdominal aorta.
In this section a remarkable ‘image’ is presented and a short comment is given.
We invite you to send in images (in triplicate) with a short comment (one page at the most) to Bohn Stafleu van Loghum, PO Box 246, 3990 GA Houten, e-mail: l.jagers@bsl.nl.
‘Moving images’ are also welcomed and (after acceptance) will be published as aWeb Site Feature and shown on our website: www.cardiologie.nl
This section is edited by M.J.M. Cramer and J.J. Bax.
References
- 1.Carter AJ, Brinker JA. Dissection of the ascending aorta with coronary angiography. Am J Cardiol 1994;73:922-3. [DOI] [PubMed] [Google Scholar]
- 2.Moles VP, Chappuis F, Simonet F, et al. Aortic dissection as complication of percutaneous transluminal coronary angioplasty. Cathet Cardiovasc Diagn 1992;26:8-11. [DOI] [PubMed] [Google Scholar]
- 3.Kazui T, Washigama N, Bashar AH, et al. Surgical outcome of acute type A aortic dissection: Analysis of risk factors. Ann Thorac Surg 2002;74:75-81. [DOI] [PubMed] [Google Scholar]