

Abstract
Aims
Rapid onset of analgesia is essential in the treatment of acute pain. There is evidence that conditions of stress cause delayed and decreased pain relief from oral analgesic products through impaired absorption. The aim was to determine the effect of surgery for removal of wisdom teeth on the plasma concentration-time profile of ibuprofen enantiomers.
Methods
Racemic ibuprofen, 200 mg in one group (n=7) and 600 mg in another group (n=7) was administered 1 week before (control) and again after (test) surgical removal of wisdom teeth. Serum concentrations of ibuprofen enantiomers were measured for 6 h.
Results
During the control phase, S- and R-ibuprofen concentrations were within the suggested therapeutic range. Surgery resulted in a 2 h delay in the mean time to peak concentration, significant decreases in serum ibuprofen concentration following both doses, and a fall to sub-optimal serum concentrations following the 200 mg dose. During the first 2 h after the 200 mg dose, dental extraction resulted in a significant reduction of the area under serum drug concentration (AUC (0, 2 h) mg l−1 h) from 5.6±2.9 to 1.6±1.8 (P<0.01) and from 5.5±3.0 to 2.1±2.0 (P<0.05) for S and R-ibuprofen, respectively. Similar observations were made following the 600 mg dose for AUC (0, 2 h) of S-ibuprofen (from 14.2±6.1 to 7.2±5.5 mg l−1 h, P<0.05) with no significant difference for R-ibuprofen (from 14.4±9.5 to 5.8±7.1). AUC (0, 6 h) was also significantly reduced by surgery. The pattern of stereoselectivity in serum ibuprofen concentration was reversed by surgery such that the S enantiomer was predominant in the control phase but not in the post-surgery phase, which is suggestive of reduced metabolic chiral inversion.
Conclusions
Surgery for wisdom tooth removal resulted in substantial decreases in the serum concentration of ibuprofen enantiomers and a prolongation in the time to peak concentration. Reduced absorption and altered metabolism are the likely cause of these changes. Thus, dental patients may experience a delayed response and possible treatment failure when taking ibuprofen for pain relief after surgery. Our observation may have implications for the treatment of other diseases.
Keywords: pain relief, dental surgery, onset of analgesia, ibuprofen enantiomers, chiral inversion
Introduction
In the treatment of acute pain rapid absorption of orally administered analgesics is desirable. For ibuprofen [1] and ketoprofen [2], there appears to be a positive relationship between plasma concentration and analgesic activity. Hence any delay in absorption or reduction in the circulating drug concentration may result in treatment failure. Therefore, analgesic formulations with enhanced absorption rates may be more effective in treating acute pain. However, none of the widely available solid dosage forms of the non-steroidal antiinflammatory drug (NSAID) class has been claimed to be superior over competing products with respect to onset of action. This is despite differences in apparent rate of absorption. In a retrospective analysis of plasma ibuprofen concentration-time curves generated over a period of 10 years in our laboratory, we have observed erratic absorption in patients experiencing pain but not in healthy volunteers. Therefore, in a prospective study, we measured the serum concentrations of ibuprofen in 14 subjects each receiving ibuprofen 1 week prior to and shortly after third molar tooth extraction, an accepted model of assessing acute pain [3]. Although the intention of this study was not to evaluate the pharmacodynamics of ibuprofen, we also recorded the pain intensity experienced by each patient at the time of ibuprofen administration.
Methods
The study was approved by the University Committee on Human experiments. Patients who were scheduled to undergo surgery for removal of third molar teeth participated in the study, and their characteristics are listed in Table 1. The subjects, who took no other medication for at least 72 h prior to the study, were randomly assigned to two groups, each receiving 200 mg (n=7) or 600 mg (n=7) single doses of racemic ibuprofen. Ibuprofen was given on two occasions, 1 week before surgery and on the day of surgery.
Table 1.
Patient characteristics (mean±s.d.).

Teeth were extracted under local anaesthetic (xylocaine 2% with adrenaline 1:100 000) and ibuprofen was administered as soon as pain intensity had become moderate or severe. All surgery was performed by the same surgeon. Patients remained supine during the first 2 h after surgery. Nuprin 200 mg tablets (Bristol-Myers-Sqibb, Princeton, NJ) were crushed gently and placed in hard gelatin capsules. In all cases, three capsules were administered (200 mg dose: 1 ibuprofen and 2 placebo or 600 mg dose: 3 ibuprofen capsules). Doses were given with 250 ml tap water and between 08.00 h to 10.00 h after an overnight fast. Food was not allowed for 2 h post-dose. Venous blood samples were taken before dosing, and then at 0.25, 0.5, 0.75, 1, 2, 3, 4, 5 and 6 h post-dose through an inserted catheter. Baseline pain intensity was recorded on a scale from 0 to 4 according to previously reported methods [2, 3].
Serum concentration of ibuprofen enantiomers was measured using a validated reversed-phase h.p.l.c. method involving liquid extraction and chiral derivatization [4]. The minimum quantifiable concentration was 0.25 μg ml−1 of each enantiomer based on 1 ml plasma (CV<10%).
tmax was the time corresponding to the highest concentration (Cmax) observed. AUC (from time of administration until 2 and 6 h post-dose) was calculated using the trapezoidal rule.
The significance of differences between pharmacokinetic indices observed during pre-surgery and post-surgery periods, and between the enantiomers in the same treatment period were examined using a two tailed paired Student’s t-test. Statistical significance was set at P<0.05.
Results
Following ibuprofen administration 1 week prior (control phase) to the scheduled surgery, patients exhibited serum concentration-time data (Figures 1 and 2 and Table 2) similar to those previously reported in healthy volunteers [5, 6]. Mean tmax was approximately 2 h (range, 0.75–4 h) and during the post-absorptive phase, serum concentrations of the S enantiomer exceeded those of the R enantiomer in all patients (P<0.05).
Figure 1.
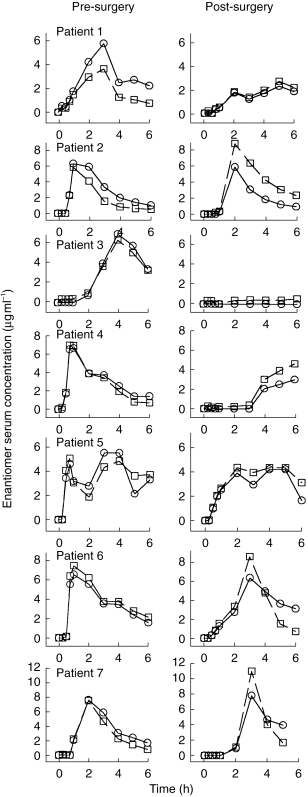
Individual serum ibuprofen enantiomer concentration-time curves following oral administration of 200 mg racemic ibuprofen 1 week before (Pre-surgery, control) and at the time of first experienced moderate to severe pain (Post-surgery). S-ibuprofen (○), R-ibuprofen (□).
Figure 2.

Individual serum ibuprofen enantiomer concentration-time curves following oral administration of 600 mg racemic ibuprofen 1 week before (Pre-surgery, control) and at the time of first experienced moderate to severe pain (Post-surgery). S-ibuprofen (○), R-ibuprofen (□).
Table 2.
Maximum serum concentration (Cmax) and the time to Cmax (tmax), and the area under serum drug concentration-time curve (AUC) of ibuprofen enantiomers. Racemic ibuprofen (200 or 600 mg) was administered orally 1 week before (Pre-surgery, control) and at the time of first experienced moderate to severe pain (Post-surgery, test) resulting from removal of a wisdom tooth.

During the post-surgery period, the ibuprofen concentration-time curves were consistent with erratic absorption (Figures 1 and 2). Surgery resulted in a significant reduction in the absorption rate as indicated by an average 2 h prolongation in the tmax (range, 2–6 h, P<0.02) of both enantiomers and a reduced Cmax of the S enantiomer (P<0.03). Surgery also caused a significant reduction in AUC (0, 2 h), occurring in all but one patient (Figure 3). AUC (0, 6 h) was also significantly reduced for the S enantiomer (P<0.03) but not for the R enantiomer as compared with the control phase. Consequently, the R enantiomer became predominant in plasma and the ratio of AUC of S to R enantiomer was significantly reduced (P<0.005) during the post-surgery period (Figure 4).
Figure 3.

Individual area under serum ibuprofen concentration vs time curves calculated for the first 2 h after oral administration of 200 or 600 mg racemic ibuprofen 1 week before (Pre- surgery, control) and at the time of first experienced moderate to severe pain (Post-surgery). For each dose, patients are identified with same symbol. Means were significantly different for S (P<0.01) and R (P<0.05) after 200 mg and for S (P<0.05) after 600 mg.
Figure 4.

Ratio (S:R) of area under plasma concentration curve-times (AUC) of the pharmacologically active S enantiomer over that of the R enantiomer following either 200 mg or 600 mg racemic ibuprofen 1 week before (Pre-surgery) and at the time of first experienced moderate to severe pain (Post-surgery). P<0.005 for 200 mg and <0.007 for 600 mg data. Horizontal lines represent a ratio of 1 (S=R).
Discussion
It has been reported that the attainment of an ibuprofen (S+R) concentration range of 11–30 μg ml−1 1 h post-dose is needed for complete pain relief in 50% of patients following extraction of the third molar [1]. A concentration of 1–10 μg ml−1 provided relief in less than 20% of patients. In the present study, these analgesic concentrations were achieved during the control period at least 2 h after both 200 and 600 mg doses. This was not the case during the post-surgical phase. In patients who received 200 mg ibuprofen, a commonly recommended analgesic dose, even the mean peak concentration of ibuprofen (S+R, 9.2 μg ml−1), which was attained 4 h post-dose, did not reach the suggested therapeutic range (Figure 1) [1]. Following the 600 mg dose, the mean peak concentration (24.5 μg ml−1) did reach a concentration at which 50% of patients should experience relief but not until after 3 h post-dose (Figure 2). Since rapid attainment of therapeutic analgesic concentrations is crucial, any delay in absorption or a reduction in the circulating concentrations may result in treatment failure. It is evident from the present data that patients undergoing dental surgery exhibit reduced serum concentration of the pharmacologically important S enantiomer. Despite high inter-subject variability in serum concentrations particularly during the post-surgery phase (Figures 1 and 2), a decrease in the AUC (0, 2 h) occurred in 13 out of 14 patients after surgery (Figure 3). The observed low serum drug concentration and the observed variability during the first 2 h post-dose may explain the discrepancy in the effectiveness of a single 200 mg dose ibuprofen [7, 8].
Our data suggest that doses which produce satisfactory serum analgesic concentrations in healthy subjects may not prove efficacious in a patient with pain. Consequently, higher doses may be required but may result in increased risk of side effects.
The mechanism responsible for the observed reduced serum ibuprofen concentration is unclear. In other stress related conditions it has been suggested that postoperative fatigue may impair nutritional intake [9], that exercise-induced stress may shift blood flow away from the gastrointestinal tract, and alter gut motility and secretion[10], that haemorrhagic shock may depress gut facilitated absorptive capacity [11], that decreased portal blood flow may reduce drug absorption [12], and that migraine depresses gut motility [13]. It is not unreasonable to suggest that the trauma of dental pain and surgery may decrease gastric emptying and secretion mediated perhaps by vagal suppression. A delayed gastric emptying is expected to prolong drug delivery to the intestine, the main site of absorption for many drugs. Absorption of the drug in the stomach may also be reduced due to diminished gastric juice secretion and movement of the organ, both of which may interfere with the processes of disintegration and dissolution.
In order to obtain sustained local analgesia in dental patients, adrenaline is added to the local anaesthetic. Adrenaline is also released in response to stress and is known to cause contraction of the pyloric sphincter which may decrease gastric emptying [14]. However, the usual local dose of 0.5 to 2 ml of 1:100 000 adrenaline (0.005–0.02 mg) injected approximately 2 h prior to the ibuprofen dose is unlikely to cause the observed decreased absorption of ibuprofen [15].
The present data demonstrates unequivocally that pain and/or the trauma of surgery result in pathophysiological changes that may render oral analgesics less effective. Injectable ketorolac is extensively used as an analgesic in severe pain. However, the effectiveness of ketorolac is probably due to its intramuscular route of administration, which ensures that its absorption does not depend on gastrointestinal variables. Orally administered ketorolac does not appear to be more advantageous over other NSAIDs such as ibuprofen [16].
In addition to a reduced serum concentration, dental extraction resulted in reversal of the serum ibuprofen enantiomers concentration ratio (Figure 4). This may be a result of a change in the metabolic chiral inversion of R-ibuprofen to the pharmacologically more important S enantiomer. This process is therapeutically significant as it constitutes 60% of the total clearance of R-ibuprofen [5] and thus may augment pharmacological activity through formation of active S-ibuprofen. The inhibition of chiral inversion in patients during dental surgery is a feasible explanation of our findings (Figure 4). Reversed stereoselectivity in plasma ibuprofen concentrations has also been observed in two other groups of patients, namely adults with liver cirrhosis [18] and infants (6–18 months) recovering from minor genito-urinary surgery [19]. Both of these patient groups are likely to have reduced biotransformation capacities compared with healthy adults. It is not known whether reversal of the S:R plasma concentration ratio in infants [19] is age-related or, as we have observed in adults, is caused by surgery. Delayed absorption of ibuprofen was also observed in these infants [19]. Other mechanisms, such as an alteration in absorption or enhanced clearance of S-ibuprofen, may also contribute to the observed stereoselective changes in the plasma concentration of the enantiomers. The former is rather unlikely as ibuprofen is absorbed passively, a processes that is not usually stereoselective [17]. Enhanced clearance of S-ibuprofen cannot be ruled out based on the present data.
Conventional non-stereospecific assays would not have detected a reduction in the AUC (0, 6 h) of S-ibuprofen following the 600 mg dose since there was no significant difference between the AUC (0, 6 h) values of the sum of the two enantiomers during the two periods. This observation highlights the importance of considering stereochemical aspects of pharmacokinetics [17].
In conclusion, the plasma concentrations of ibuprofen were found to be substantially lower and took longer to reach their maximum values in patients who had undergone surgery for third molar tooth extraction. Furthermore, plasma concentrations of the pharmacologically important S enantiomer decreased relative to the R enantiomer. Thus, delay onset of analgesia and even treatment failure may occur in dental patients taking normal doses of the drug. This finding may also have implications for other drugs and other diseases or treatment interventions.
Acknowledgments
This work was supported, in part, by a grant from Arthritis Society of Canada.
References
- 1.Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol Ther. 1986;40:1–7. doi: 10.1038/clpt.1986.129. [DOI] [PubMed] [Google Scholar]
- 2.Seymour RA, Kelly PJ, Hawkesford JE. Pharmacokinetics and efficacy of low-dose ketoprofen in prospective dental pain. Clin Drug Invest. 1998;15:279–284. doi: 10.2165/00044011-199815040-00003. [DOI] [PubMed] [Google Scholar]
- 3.Goldstein DJ, Brunelle RL, George RE, et al. Picenadol in large multicenter dental pain study. Pharmacotherapy. 1994;14:54–59. doi: 10.1002/j.1875-9114.1994.tb02789.x. [DOI] [PubMed] [Google Scholar]
- 4.Wright MR, Sattari S, Brocks DR, Jamali F. An improved assay for the enantiomers of ibuprofen. J Chromatogr. 1992;583:259–265. doi: 10.1016/0378-4347(92)80562-5. [DOI] [PubMed] [Google Scholar]
- 5.Lee EJD, Williams K, Graham G, Champion D. Stereoselective disposition of ibuprofen enantiomers in man. Br J Clin Pharmacol. 1985;19:669–674. doi: 10.1111/j.1365-2125.1985.tb02694.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jamali F, Mehvar R, Russell AS, Sattari S, Yakimets WW, Koo Koo. Human pharmacokinetics of ibuprofen enantiomers following different doses and formulations: intestinal chiral inversion. J Pharm Sci. 1992;81:221–225. doi: 10.1002/jps.2600810306. [DOI] [PubMed] [Google Scholar]
- 7.Kiersch TA, Halladay SC, Koschik M. A double-blind, randomized study of naproxen sodium, ibuprofen, and placebo in postoperative dental pain. Clin Ther. 1993;15:845–854. [PubMed] [Google Scholar]
- 8.Seymour RA, Ward-Booth P, Kelly PJ. Evaluation of different doses of soluble ibuprofen and ibuprofen tablets in postoperative dental pain. Br J Oral Maxillofac Surg. 1996;34:110–114. doi: 10.1016/s0266-4356(96)90147-3. [DOI] [PubMed] [Google Scholar]
- 9.Christensen T, Kehlet H. Postoperative fatigue. World J Surg. 1993;17:220–115. doi: 10.1007/BF01658930. [DOI] [PubMed] [Google Scholar]
- 10.Brouns F, Beckers E. Is the gut an athletic organ?, absorption and exercise. Sports Med. 1993;15:242–257. doi: 10.2165/00007256-199315040-00003. [DOI] [PubMed] [Google Scholar]
- 11.Singh G, Chaudry KI, Chaudry IH. ATP-MgCl2 restors gut absorptive capacity early after trauma-hemorrhagic shock. Am J Physiol. 1993;264:R977–R983. doi: 10.1152/ajpregu.1993.264.5.R977. [DOI] [PubMed] [Google Scholar]
- 12.Sodeyama M, Kirk SJ, Regan MC, Barbul A. The effect of hemorrhagic shock on intestinal amino acid absorption in vivo. Circ Shock. 1992;38:153–156. [PubMed] [Google Scholar]
- 13.Tfelt-Hansen P, Henry P, Mulder LJ, Scheldewaert RG, Schoenon J, Chazot G. The effectiveness of combined oral lysine acetylsalicylate and metoclopramide compared with oral sumatriptan for migraine. Lancet. 1995;346:923–926. doi: 10.1016/s0140-6736(95)91554-0. [DOI] [PubMed] [Google Scholar]
- 14.Tack JF, Wood JD. Actions of noradrenaline on myenteric neurons in the guinea pig gastric antrum. J Auton Nerv Syst. 1992;41:67–77. doi: 10.1016/0165-1838(92)90128-4. [DOI] [PubMed] [Google Scholar]
- 15.Malamed SF, Quinn CL. Local anesthesia. Toronto: Mosby Year Book; 1990. p. 239. [Google Scholar]
- 16.Forbes JA, Kehm CJ, Grodin CD. Evaluation of ketorolac, ibuprofen, acetaminophen, and an acetaminophen-codeine combination in postoperative oral surgery pain. Pharmacotherapy. 1990;10:94S–105S. [PubMed] [Google Scholar]
- 17.Brocks D, Jamali Jamali, F F. Stereochemical aspects of pharmacotherapy. Pharmacotherapy. 1995;15:551–564. doi: 10.1002/j.1875-9114.1995.tb02863.x. [DOI] [PubMed] [Google Scholar]
- 18.Li G, Treiber G, Maier K, Walker S, Klotz U. Disposition of ibuprofen in patients with liver cirrhosis, stereochemical considerations. Clin Pharmacokin. 1993;25:154–163. doi: 10.2165/00003088-199325020-00008. [DOI] [PubMed] [Google Scholar]
- 19.Rey E, Pariente-Khayat A, Gouyet L, et al. Stereoselective disposition of ibuprofen enantiomers in infants. Br J Clin Pharmacol. 1994;38:373–375. doi: 10.1111/j.1365-2125.1994.tb04369.x. [DOI] [PMC free article] [PubMed] [Google Scholar]