

Abstract
Aims
To assess whether frequency of placebo administration is associated with duodenal ulcer healing.
Methods
A systematic literature review of randomized clinical trials was undertaken. 79 of 80 trials that met the inclusion criteria. The pooled 4 week placebo healing rate of all duodenal ulcer trials that employed a four times a day regimen was compared with the rate obtained from trials with a twice a day regimen.
Results
The pooled 4 week healing rate of the 51 trials with a four times a day regimen was 44.2% (805 of 1821 patients) compared with 36.2% (545 of 1504 patients) in the 28 trials with a twice a day regimen (difference, 8.0% [equal effects model]; 95% confidence interval, 4.6% to 11.3%). Depending on the statistical analysis, the rate difference ranged from 6.0% (multivariable random effects model) to 8.0% (equal effects model). A number of sensitivity analyses showed comparable differences between the two regimens. Most of these sensitivity analyses were not significant, probably because a number of trials were excluded resulting in a loss of power.
Conclusions
We found a relation between frequency of placebo administration and healing of duodenal ulcer. We realize that the comparison was based on nonrandomized data. However, we speculate that the difference between regimens was induced by the difference in frequency of placebo administration. A better knowledge of various placebo effects is required in order to make clinically relevant assessments of treatment effects derived from placebo-controlled trials.
Keywords: duodenal ulcer, placebo effect
Introduction
The term placebo has been defined as ‘any therapeutic procedure which has an effect on a patient, symptom, syndrome or disease, but which is objectively without specific activity for the condition being treated’ [1]. According to this definition, the placebo effect is ‘the psychological or psychophysiological effect produced by placebos’. A common method in the evaluation of placebo effects is to equate the results in the placebo group of a clinical trial to the placebo effect [2, 3]. However, the natural course of disease, regression towards the mean, measurement bias, and (unidentified) parallel interventions, may also play a role in the response in the placebo arm of a clinical trial [2].
Before Helicobacter pylori eradication became standard treatment, other medical therapies for duodenal ulcers were available from the late 1970s, when the H2-receptor antagonist cimetidine was introduced [4, 5]. Since then, various drugs with different mechanisms of action have been tested in a large number of randomized clinical trials [6]. The dosage regimens of the drugs changed over the years, starting with a four times a day regimen in the early trials of the H2-receptor antagonists, through a twice daily regimen, ending in a once daily regimen in the later trials of the H2-receptor antagonists and proton pump inhibitors. Many trials have directly compared active drugs, but there are also numerous placebo controlled trials. Of the placebo controlled trials, by far the most have evaluated a four times a day or a twice a day administration.
Several authors have commented that randomized controlled trials in duodenal ulcer have given substantially different placebo healing rates [7–9]. It has not been postulated that in duodenal ulcers the frequency of placebo administration might influence the healing process. By means of a systematic review we aimed to examine the influence of frequency of placebo administration on duodenal ulcer healing. Therefore we calculated the pooled ulcer healing rate of the placebo arms of all randomized clinical trials with a four times a day regimen and compared this with the pooled placebo healing rate in trials with a twice a day regimen.
Methods
Published trials were located by various strategies, including extensive computer searches of Medline (1966–97), Embase (1974–97), and the Cochrane Library (1997, issue 4), checking reference lists of articles and text books, manufacturers of ulcer medication, and correspondence with gastroenterologists. Criteria for inclusion of the trials in this systematic review were (a) randomization, (b) double-blind methodology, (c) only uncomplicated ulcers (complication defined as bleeding, stenosis or recent perforation), (d) ulcers assessed by endoscopy at baseline and at the end of treatment, (e) healed ulcer as endpoint, ( f ) placebo administration four times a day (with each meal and at bedtime) or twice a day (in the morning and at bedtime), ( g) placebo group taking tablets or capsules (not liquid preparations), (h) 4 week healing rate reported and (i) presentation as full paper, not as abstract. There was no language restriction. If it was not possible to separate duodenal from gastric ulcer in the case of mixed ulcers or if duodenal ulcers and prepyloric ulcers were reported together and the percentage of prepyloric ulcers was greater than 30%, the trial was excluded. In case of multiple publications of the same trial, the earliest full publication determined the year of publication, but the information from all publications was used. As most of the trials reported 4 week healing rates, we excluded trials that did not report 4 week healing rates. Trials assessing the efficacy of any of the following drugs were not included in the review: proton pump inhibitors because the expected benefit from the experimental treatment is not in the same range as the other drugs, possibly resulting in different expectations of both patients and physicians; colloidal bismuth subcitrate because it has mainly been evaluated as liquid preparations; pirenzepine because it has mainly been evaluated using a three times a day regimen.
Relevant data for the evaluation were extracted from text, tables, and figures of the publications. In many trials the ulcer healing rate was computed by dividing the number of patients with a healed ulcer by the total number of evaluable and compliant patients. Our analyses are based on these reported healing rates. Differences in healing rates between placebo regimens were assessed by equal, fixed, and random effects models [10]. The equal and fixed effects models assume all trials to be similar in that they share the same underlying healing rate, observed differences between healing rates are thus considered to be only due to chance. In the equal effects model, for each treatment regimen the pooled healing rate is computed as follows: the total number of healed patients divided by the total number of patients, this means that an n-weighted mean healing rate is computed. In the fixed and random effects analyses the logit of the healing rate is modelled. In the fixed effects model each study is weighted by the inverse of its sampling variance. Adjusting for differences between trials was employed in a multivariable fixed effects analysis using linear regression analysis with trial characteristics as independent variables and the logit of the healing rate as dependent variable [11]. For univariate random effects analysis the model as proposed by DerSimonian & Laird was used [12]. Random effects models incorporate potential heterogeneity of the healing rate among different studies by assuming that each study estimates a unique healing rate. A multivariable random effects analysis was carried out using a mixed linear model with study as random factor and all others as fixed factors. In the multivariable analyses, for trials with missing data, a dummy variable was added to the model and the overall mean substituted as observed value. Homogeneity of observed healing rates was assessed using chi-square tests of independence [10]. Differences between treatment regimens are presented as means with 95% confidence intervals (CI). Unless specified, all analyses are based on the multivariable random effects model.
Results
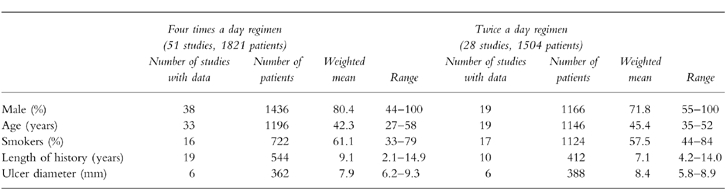
Eighty trials met the inclusion criteria. One trial was excluded because only patients were included who were refractory to histamine H2-receptor blocker therapy [13]. This left 79 trials, reported in 78 publications, for our review (appendix). Fifty-one studies employed a four times a day regimen, 28 employed a twice a day regimen. Trials with twice a day regimens were more often carried out in the United States (Table 1); patient characteristics showed some differences between the two placebo regimens (Table 2).
Table 1.
Characteristics of studies included in the systematic review of four times a day vs twice a day placebo administration in duodenal ulcer healing.
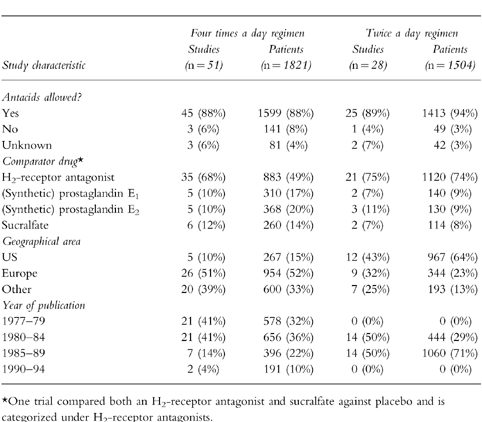
Table 2.
Characteristics of patients with duodenal ulcer included in the placebo groups of the trials of duodenal ulcer healing, by treatment regimen.
In the four times a day regimen, 805 of 1821 patients (44.2%) were healed after 4 weeks of placebo treatment, while in the group that took a placebo twice a day 545 of 1504 patients (36.2%) were healed (difference, 8.0% [equal effects model]; 95% CI 4.6%, 11.3%). Table 3 shows equal, fixed, and random effect estimates of the difference in healing rate between the two dosage regimens. The multivariable fixed effect model, adjusted for differences between trials with regard to geographical area of study (United States vs all other regions), experimental drug (H2-receptor antagonist vs all other drugs), antacids allowed (yes vs no/unknown), gender, age, and smoking, yielded a 7.4% difference (95% CI 3.3%, 11.3%). Estimating variation between study outcomes, revealed significant heterogeneity for both placebo regimens (P<0.001), so random effects analyses were also performed. The univariate random effects model gave a 7.0% difference (95% CI 0.9%, 13.4%). Incorporating the same set of trial and patient characteristics as in the fixed effects analysis, the multivariable random effects model yielded a 6.0% difference (95% CI 0.3%, 12.7%) in healing rates.
Table 3.
Differences in healing rate between groups with four times (51 trials, 1821 patients) and twice a day placebo administration (28 trials, 1504 patients) in randomized clinical trials of duodenal ulcer.

Limiting the analysis to studies that were carried out in the United States a 10.7% difference was observed (95% CI −3.2%, 20.5%). Excluding trials that were published before 1980 did not change the difference between treatment regimens (6.4%; 95% CI −2.3%, 15.5%). Within the subgroup of studies that evaluated an H2-receptor antagonist against placebo, a 3.0% difference was found (95% CI −1.1%, 8.6%). Both treatment regimens had 11 studies with more than 50 patients in the placebo group. In these larger trials the difference was 5.3% (95% CI −7.0%, 14.2%).
Discussion
The results of our review suggest a relation between frequency of placebo administration and healing of duodenal ulcer. Depending on the method of statistical analysis, the difference in mean pooled 4 week healing rates ranges from 6% to 8%, the higher healing rate observed in trials with a four times a day regimen. What might have caused the difference in healing rates between the two groups?
First, the pooled healing rates of the two treatment regimens were obtained from different trials, so it is possible that the two groups were not comparable. Patients in the trials with a four times a day regimen were slightly more often male, were somewhat younger, and were more often smokers. Male gender, younger age, and smoking have been associated with lower healing rates [6], so adjusting for these baseline characteristics would have resulted in a larger rather than smaller healing rate difference. Half of the patients in trials with a four times a day regimen originally came from trials that evaluated an H2-receptor antagonist, whereas in trials with a twice a day regimen 75% of patients came from trials that evaluated an H2-receptor antagonist. When the analysis was restricted to trials with an H2-receptor antagonist as the experimental drug, the difference was 3%. This means that adjusting for type of comparator drug in the multivariable analysis decreased the difference. The result was that the multivariable analyses which included gender, age, smoking, and type of comparator drug, yielded differences that were comparable with the univariate analyses. Moreover, the observed difference between regimens could be due to residual confounding. Although we adjusted for a number of possible confounders, we can not rule out that in this nonrandomized comparison the observed difference was caused by some unrecognized confounding factor or factors.
Second, the trials with a twice a day placebo administration were carried out from 1980 onwards, whereas trials with a four times a day administration were also conducted at the end of the 1970s. The analysis that excluded trials published up to 1980 found the same difference between regimens, although it was no longer significant, probably because 21 trials were excluded resulting in a loss of power. The same results were obtained when we restricted the analysis to trials that were published from 1985 onwards. This eliminates time dependent influences on the healing rate such as inclusion of more treatment resistant patients in later trials. Furthermore, trials with a twice a day regimen were more frequently carried out in the United States. The analysis that included only trials from the United States showed a 10% difference which just failed to achieve statistical significance. However, this analysis was based on only 17 trials which reduces statistical power enormously. Hence we think that calendar time and geographical area are not a main source of confounding.
Third, in numerous trials the statistical analysis was based on the number of evaluable patients, while some trials also excluded patients from the analysis who did not comply with the treatment regimen. In theory, patients on a four times a day regimen are more likely to be noncompliant. So analysing healing rates of compliant and evaluable patients only, could have resulted in biased healing rate estimates. However, many reports did not specify the number of excluded patients because of noncompliance. Therefore we were not able to examine the impact of noncompliance on the healing rate. Using the total number of randomized patients in the denominator instead of the number of evaluable and compliant patients did not change the healing rate difference between the two placebo regimens.
Fourth, it would be possible that the physician who decides to include a patient in a trial, makes an assessment whether an individual patient will comply with a certain drug regimen. Therefore the group of patients in the trials with a four times a day regimen might be different from the patients in the twice a day trials. In a randomized trial to evaluate the efficacy of lipid-lowering drugs in the therapy of coronary heart disease, patients in the placebo arm of the trial who complied with the prescribed treatment regimen (took at least 80% of placebo capsules) had a lower 5-year mortality compared with the noncompliers [14]. We may hypothesize that in this trial, among other reasons, the frequency of placebo administration had some effect on mortality, or that patient compliance was related to other factors which are associated with mortality. Although we consider it unlikely, similar selection bias might have occurred in the trials that employed a four times a day regimen may explaining the difference between the placebo regimens.
Fifth, the difference in healing rates could be the result of the frequency of placebo administration. Patients on the more intense regimen might have felt they were receiving more treatment. This might have induced a psychophysiological response: decreased gastric acid production, increased prostaglandin synthesis, a psychoneuroimmunological response against Helicobacter pylori, or a combination of these. Additionally, subjects on the four times a day regimen might have paid more attention to the composition and timing of meals.
Some trials have evaluated a once daily drug administration against placebo [15–19]. These trials originate mainly from the United States and were published in the late 1980s and 1990s. In one trial [15], a dose validation study of once daily cimetidine, the placebo regimen was four placebos at night. The healing rate in the placebo group was 45%. The healing rate in the remaining four trials ranged from 31% to 61%.
A number of small randomized controlled trials have evaluated the association between frequency of placebo administration and efficacy with inconsistent results [20–22]. In 1970, Rickels et al. [21] concluded that ‘… the dosage of the placebo may be a significant and determining factor in the placebo response, although this is not clearly determined.’ Since then, little research on this subject has been carried out, with the exception of a study by Ilnyckyj et al. who recently demonstrated that the placebo response in ulcerative colitis is greater in trials with more frequent study visits [23]. We realize that it is not possible to test our findings in a randomized clinical trial. Blinding is not possible and it would be unethical since it is now generally accepted that duodenal and stomach ulcers are causally linked to Helicobacter pylori infection [24] and effective therapy is available. Therefore we feel that our approach to this question, although not perfect, is the best available option.
In this systematic review we have shown that there is a relation between frequency of placebo administration and duodenal ulcer healing. We realize that the comparison was based on nonrandomized data. Therefore we speculate that the difference between regimens was induced by the difference in placebo administration. Other factors such as reputation of the doctor, the patient’s attitude towards the expected benefit of the treatment, quality of the physician-patient communication, and perceptual characteristics of the treatment might also influence therapeutic outcomes. Although these factors are widely recognized in medicine, they have generally been regarded as random error in research. It is important to identify these factors in order to optimize clinical practice and improve the methodology of clinical research. We encourage researchers in other fields of medicine to look for comparable examples, either from combining results available in the literature or from new experimental studies.
Acknowledgments
We thank Guus Hart (Amsterdam, the Netherlands) for statistical advice and Gerben ter Riet (Maastricht, the Netherlands) and Gouke Bonsel (Amsterdam, the Netherlands) for helpful comments on the text.
APPENDIX
Trials that employed a four times a day regimen
1 Ahmed WU, Qureshi H, Alam E, Zuberi SJ. A double-blind tudy of misoprostol (SC-29333) in the healing of duodenal ulcer. J Gastroenterol Hepatol 1991; 6: 179–180.
2 Albano O, Barbara L, Miglioli M, et al. Cimetidine in short-term medical treatment of active duodenal ulcer: a multicentre endoscopic double-blind study on 164 patients. Ital J Gastroenterol 1978; 10: 247–248.
3 Barakat M, Badawi A, Menon K. Cimetidine in the treatment of active duodenal ulcer disease. J Kuwait Med Assoc 1979; 13: 21–26.
4 Bardhan KD, Saul DM, Edwards JL, et al. Comparison of two doses of cimetidine and placebo in the treatment of duodenal ulcer: a multicentre trial. Gut 1979; 20: 68–74.
5 Bianchi Porro G, Dal Monte PR, Petrillo M, Giuliani Piccari G, D’Imperio N, Daniotti S. Pirenzepine vs cimetidine in duodenal ulcer. A double-blind, placebo-controlled, short-term clinical trial. Digestion 1982; 23: 110–115.
6 Binder HJ, Cocco A, Crossley RJ, et al. Cimetidine in the treatment of duodenal ulcer. Gastroenterology 1978; 74: 380–388.
7 Brand DL, Roufail WM, Thomson ABR, Tapper EJ. Misoprostol, a synthetic PGE1analogue, in the treatment of duodenal ulcers. A multicentre double-blind study. Dig Dis Sci 1985; 30(Suppl): 147S–58S.
8 Chen PC, Wu CS, Chang-Chien CS, Liaw YF. Double-blind therapeutic trial of active duodenal ulcer disease with cimetidine. Taiwan I Hsueh Hui Tsa Chih 1979; 78: 777–783.
9 Collen MJ, Hanan MR, Maher JA, et al. Cimetidine vs placebo in duodenal ulcer therapy. Six-week controlled duoble-blind investigation without any antacid therapy. Dig Dis Sci 1980; 25: 744–749.
10 Danielsson A, Ek B, Nyhlin H, Steen L. The relationship between active peptic ulcer, endoscopic duodenitis and symptomatic state after treatment with cimetidine. Ann Clin Res 1980; 12: 4–12.
11 Darle N, Almskog B, Falk A, et al. Ranitidine in the treatment of gastric, prepyloric and duodenal ulcer. A controlled prospective double-blind trial. Ann Clin Res 1984; 16: 6–9.
12 Dobrilla G, de Pretis G, Felder M, Chilovi F. Endoscopic double-blind controlled trial of ranitidine vs placebo in the short term treatment of duodenal ulcer. Hepatogastroenterology 1981; 28: 49–52.
13 Dobrilla G, Felder M, Valentini M, Bonoldi MC. Pirenzepine and cimetidine in the short term treatment of duodenal ulcer: a vs placebo endoscopic controlled trial. Curr Ther Res1980; 28: 371–376.
14 Dobrilla G, Valentini M, Filippini M, Felder M, Bonoldi MC, Moroder E. Therapie mit Cimetidin beim Ulcus duodeni. Klinisch-endoskopische Studie an 76 Patienten. Munchener Med Wochenschrift 1978; 120: 839–842.
15 Dolle W, Malchow H, Sewing KF, Albinus M, Schomerus H. The effect of cimetidine on inpatients with duodenal ulcer. A double blind trial. Acta Gastroenterol Belg 1978; 41: 424–426.
16 Elsborg L, Boysen K, Bruusgaard A, Reinicke V. Sucralfate vs placebo treatment in duodenal and prepyloric ulcer: a clinical endoscopic, double-blind controlled investigation. Hepatogastroenterology 1984; 31: 269–271.
17 Euler AR, Krawiec J, Odes H, et al. An evaluation of arbaprostil at multiple doses for the treatment of acute duodenal ulcer: a randomized double-blind placebo controlled international trial. Am J Gastroenterol 1990; 85: 145–149.
18 Euler AR, Tytgat G, Berenguer J, et al. Failure of a cytoprotective dose of arbaprostil to heal acute duodenal ulcers. Results of a multiclinic trial. Gastroenterology 1987; 92: 604–607.
19 Falaiye JM, Popoola AO. A double-blind comparative study of cimetidine and placebo in adult Nigerian duodenal ulcer patients with special reference to gastroduodenal mucosal morphology and intestinal bacterial activity. Afr J Med Med Sci 1979; 8: 61–70.
20 Festen HPM, Lamers CBH, van Tongeren JHM. De onderdrukking van de maagzuurproduktie door middel van cimetidine; resultaten van een dubbelblind onderzoek naar de betekenis van cimetidine voor de behandeling van peptische ulcera. Ned Tijdschr Geneeskd 1978; 122: 862–865.
21 Figueroa RB, Espejo HR. Cimetidine in active duodenal ulcer. Curr Ther Res 1979; 25: 16–24.
22 Fixa B, Komarova O. Aluminium sucrose sulphate (sucralfate) in the treatment of peptic ulcer (double-blind study). In Duodenal ulcer, gastric ulcer: Sucralfate, a new therapeutic agented Caspary WF.Munich:Urban and Schwarzenberg, 1981: 80–84.
23 Giger M, Gonvers JJ, Weber KB, et al. Therapie des Ulcus duodeni mit Cimetidin, Pirenzepin und Placebo. Schweiz Med Wochenschr 1979; 109: 617–618.
24 Gray GR, Smith IS, McKenzie I, Crean GP, Gillespie G. Oral cimetidine in severe duodenal ulceration. A double-blind controlled trial. Lancet 1977; i: 4–7.
25 Grewal GS, Broor SL, Mehta SK, Chuttani PN. Cimetidine in the treatment of duodenal ulcer: results of a short-term double blind study. J Assoc Physicians India 1979; 27: 785–789.
26 Guelrud M, Beker S, Machado LP, Borjas JAO. Effectos de los bloqueadores H2 (Cimetidina) en el tratamiento de la ulcera duodenal. Estudio doble ciego multicentrico. G E N 1978; 32: 451–459.
27 Hentschel E, Schutze K, Havelee L. Die Behandlung des Ulcus duodeni und des prapylorischen Ulcus ventriculi mit Cimetidin. Wien Klin Wochenschr 1979; 91: 53–57.
28 Hollander D. Efficacy of sucralfate for duodenal ulcers: a multicentre, double-blind trial. J Clin Gastroenterol 1981; 3(Suppl 2): 153–157.
29 Khanna SS, Pipalia DH, Nadkarni PM, Naik SR. Sucralfate in the short term treatment of duodenal ulcer. A double-blind comparison with cimetidine and placebo. J Assoc Physicians India 1989; 37: 503–505.
30 Kollberg B, Slezak P. The effect of prostaglandin E2 on duodenal ulcer healing. Prostaglandins 1982; 24: 527–536.
31 Lam SK, Koo J. Accurate prediction of duodenal-ulcer healing rate by discriminant analysis. Gastroenterology 1983; 85: 403–412.
32 Lam SK, Lau WY, Choi TK, et al. Prostaglandine E1 (misoprostol) overcomes the adverse effect of chronic cigarette smoking on duodenal ulcer healing. Dig Dis Sci 1986; 31(Suppl): 68S–74S.
33 Lambert R, Bader JP, Bernier JJ, et al. Traitement de l’ulcere gastrique et duodenal par la cimetidine. Etude multicentrique. Gastroenterol Clin Biol 1977; 1: 855–860.
34 Manousos ON, Zografos A, Nicolaou A, Scandalis N, Kalogerakou-Ioannidi E. A double-blind study of cimetidine in patients with duodenal or gastric ulcer in Greece. J Int Med Res 1978; 6: 381–383.
35 Marini G, Guidoni G, Schiaroli G, Camarri E, Magni E, Fornara CF. Endoscopic evaluation of sulglycotide on healing duodenal ulcer. Clin Trials J1981; 18: 105–113.
36 Mazure PA, Cosen JN, Ciccia JE, et al. Estudio doble ciego con misoprostol en el tratamiento de la ulcera duodenal activa. Acta Gastroenterol Latinoam 1985; 15: 13–24.
37 McHardy GG. A multicentre, double-blind trial of sucralfate and placebo in duodenal ulcer. J Clin Gastroenterol 1981; 3(Suppl 2): 147–152.
38 Misra RC, Gupta BB, Agarwal SK, Gupta PS. Cimetidine in the treatment of duodenal ulcer. J Assoc Physicians India 1981; 29: 705–709.
39 Mukhtar ED, El Masri SH, El Agib AA. Double-blind comparative study of cimetidine 1 gm daily and placebo in the treatment of patients with severe duodenal ulceration in the Sudan. East Afr Med J 1982; 59: 413–415.
40 Nanivadekar SA, Govindani NF, Tandon NH, Dixit SD, Thomas G. Short-term therapy with cimetidine of endoscopically proved chronic duodenal ulcer. J Postgrad Med 1982; 28: 73–77.
41 Orchard R, Elliot C. A double-blind placebo-controlled study of sucralfate in the treatment of gastric and duodenal ulcer. In Duodenal ulcer, gastric ulcer: Sucralfate, a new therapeutic concept,ed Caspary WF. Munich: Urban and Schwarzenberg, 1981: 85–88.
42 Salgado JA, de Oliveira CA, Lima Junior GF, Paula Castro L. Endoscopic findings after antacid, cimetidine and placebo for peptic ulcer. Importance of staging the lesions. Arq Gastroenterol 1981; 18: 51–53.
43 Semb LS, Berstad A, Myren J, Foss JC, Carlsen E, Kruse-Jensen A. A double-blind multicentre comparative study of cimetidine and placebo in short-term treatment of active duodenal ulceration. In Cimetidine. Proceedings of the 2nd International Symposium on histamine H2-receptor antagonists, edsBurland WL, Simkins MA. Amsterdam: Exerpta Medica, 1977: 248–253.
44 Sonnenberg A, Muller-Lissner SA, Vogel E, et al. Predictors of duodenal ulcer healing and relapse. Gastroenterology 1981; 81: 1061–1067.
45 Sontag SJ, Mazure PA, Pontes JF, Beker SG, Dajani EZ. Misoprostol in the treatment of duodenal ulcer. A multicentre double-blind placebo-controlled study. Dig Dis Sci 1985; 30(Suppl): 159S–63S.
46 Sung JL, Yu JY, Wang TH, Wang CY, Chen DS. A placebo controlled, double blind study of sucralfate in the short term treatment of duodenal ulcer. Scand J Gastroenterol 1983; 18(Suppl 83): 21–24.
47 Ubilluz R. Cimetidine in the treatment of active duodenal ulcer: a double-blind study. Curr Ther Res 1979; 25: 243–250.
48 Vantini I, Ederle A, Bovo P, et al. Serum fasting gastrin levels after short-term treatment with cimetidine in patients with duodenal ulcer. Acta Hepatogastroenterol 1978; 25: 376–379.
49 Vantrappen G, Janssens J, Popiela T, et al. Effect of 15 (R) -15-Methyl Prostaglandin E2 (arbaprostil) on the healing of duodenal ulcer. Gastroenterology 1982; 83: 357–363.
50 Villalobos JJ, Elizondo J, Guevara L, Centeno F. Cimetidine in the treatment of duodenal ulcer: double-blind study. J Int Med Res 1978; 6: 351–354.
51 Wengrower D, Fich A, Goldin E, Eliakim R, Ligumsky M, Rachmilewitz D. Cytoprotective doses of arbacet with minimal antisecretory properties are not effective in duodenal ulcer healing. Dig Dis Sci 1987; 32: 857–860.
Trials that employed a twice a day regimen
1 Berstad A, Kett K, Aadland E, et al. Treatment of duodenal ulcer with ranitidine, a new histamine H2-receptor antagonist. Scand J Gastroenterol 1980; 15: 637–639.
2 Bianchi Porro G, Petrillo M, Lazzaroni M. Ranitidine in the short term treatment of duodenal ulcer: a multicentre endoscopic double-blind trial. In The Clinical Use of Ranitidine. Second International Symposium on Ranitidine, eds Misiewicz JJ, Wormsley KG. Oxford: Medicine Publishing Foundation, 1982: 136– 142.
3 Boucekkine T, Meknini B, Bitoun A, et al. Treatment of duodenal ulcer with rioprostil: a randomized multicentre double-blind study. Scand J Gastroenterol 1989; 24(Suppl 164): 191–193.
4 Bright-Asare P, Krejs GJ, Santangelo WC, et al. Treatment of duodenal ulcer with enprostil, a prostaglandin E2 analogue. Am J Med 1986; 81(Suppl 2A): 64–68.
5 Bright-Asare P, Sontag SJ, Gould RJ, Brand DL, Roufail WM. Efficacy of misoprostol (twice daily dosage) in acute healing of duodenal ulcer. A multicentre double-blind controlled trial. Dig Dis Sci 1986; 31(Suppl): 63S–7S.
6 Cloud ML, Offen WW, Matsumoto C, Chernish SM. Healing and recurrence of active duodenal ulcer with nizatidine. Clin Pharmacol Ther 1989; 46: 310–316.
7 Dobrilla G, Barbara L, Bianchi-Porro G, et al. Placebo-controlled studies with ranitidine in duodenal ulcer. Scand J Gastroenterol 1981; 16(Suppl 69): 101–107.
8 Dyck WP, Cloud ML, Offen WW, Matsumoto C, Chernish SM. Treatment of duodenal ulceration in the United States. Scand J Gastroenterol 1987; 22(Suppl 136): 47–55.
9 Forssell H, Koch G. Effect of H2-receptor blockade by ranitidine on ulcer healing and gastric acid secretion in patients with gastric and duodenal ulcers. Eur J Clin Pharmacol 1983; 25: 195–198.
10 Gitlin N, McCullough AJ, Smith JL, Mantell G, Berman R. A multicentre, double-blind, randomized, placebo-controlled comparison of nocturnal and twice-a-day famotidine in the treatment of active duodenal ulcer disease. Gastroenterology 1987; 92: 48–53.
11 Hirschowitz BI, Berenson MM, Berkowitz JM, et al. A multicentre study of ranitidine treatment of duodenal ulcers in the United States. J Clin Gastroenterol 1986; 8: 359–366.
12 Jones DB, Rose JDR, Smith PM, Calcraft BJ. Treatment of peptic ulcer with ranitidine. A clinical trial. In The Clinical Use of Ranitidine Second International Symposium on Ranitidine,eds Misiewicz JJ, Wormsley KG. Oxford: Medicine Publishing Foundation, 1982: 185–188.
13 Klinger J, Maggiolo P, Goic A. Ranitidina, cimetidina y placebo en el tratamiento a corto y mediano plazo de la ulcera duodenal. Rev Med Chil 1984; 112: 337–341.
14 Korman MG, Hansky J, Merrett A, Schmidt GT. Ranitidine in duodenal ulcer. Incidence of healing and effect of smoking. Dig Dis Sci 1982; 27: 712–715.
15 Lee FI, Fielding JD, Mackay C, et al. Comparison of twice daily ranitidine and placebo in the treatment of duodenal ulcer—a multicentre study in the United Kingdom. Hepatogastroenterology 1982; 29: 127–129.
16 Leroux P, Farley A, Archambault A, et al. Effect of ranitidine on healing of peptic ulcer: a 2-month study. Am J Gastroenterol 1983; 78: 227–230.
17 Levendoglu H, Mehta B, Wait C, Reddy G, Hatcher C. Nizatidine. A new histamine receptor blocker in the treatment of active duodenal ulcers. Am J Gastroenterol 1986; 81: 1167–1170.
18 Makalinao AU, Zano FM. Ranitidine in the treatment of peptic ulcer. Clin Ther 1984; 6: 185–192.
19 Mangiameli A, Monaco S, Catalano F, Blasi A. Ranitidine in short-term treatment of duodenal ulcer. Ital J Gastroenterol 1982; 14: 5–6.
20 Marks IN, Wright JP, Denyer M, Hatfield A, Girdwood AH, Lucke W. Ranitidine heals duodenal ulcers. S Afr Med J 1982; 61: 152–154.
21 Moshal MG, Spitaels JM, Khan F. A double-blind endoscopically controlled trial of ranitidine in a high incidence area. Scand J Gastroenterol 1981; 16(Suppl 69): 129–131.
22 Saunders JHB, Oliver RJ, Higson DL. Dyspepsia: incidence of nonulcer disease in a controlled trial of ranitidine in general practice. Br Med J 1986; 292: 665–668.
23 Schubert T. Twice-daily sucralfate dosing to heal acute duodenal ulcer. Am J Med 1989; 86(Suppl 6A): 108–112.
24 Schubert TT, Frizzell JA, Meier PB, Cano RI, Schwartz KE. A US multicentre study of enprostil 35 μg twice daily for treatment of prepyloric, pyloric channel and duodenal bulb ulcers. Dig Dis Sci 1989; 34: 1355–1360.
25 Theodoropoulos G, Tzivras M, Archimandritis A, Dimitriou P, Damoulakis G. Short-term ranitidine treatment of gastric and duodenal ulcer in a Greek population. Ital J Gastroenterol 1984; 16: 255.
26 Thomson ABR, Navert H, Halvorsen L, et al. Treatment of duodenal ulcer with enprostil, a synthetic prostaglandin E2 analogue. Am J Med 1986; 81(Suppl 2A): 59–63.
27 Yap I, LaBrooy SJ, Tay HH, Guan R, Kang JY. Ranitidine in the acute treatment of duodenal ulcer. A double-blind placebo-controlled trial. Singapore Med J 1985; 26: 539–542.
References
- 1.Shapiro AK. Factors contributing to the placebo effect. Their implications for psychotherapy. Am J Psychother. 1964;18:73–88. doi: 10.1176/appi.psychotherapy.1964.18.s1.73. [DOI] [PubMed] [Google Scholar]
- 2.Ernst E, Resch KL. Concept of true and perceived placebo effects. Br Med J. 1995;311:551–553. doi: 10.1136/bmj.311.7004.551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hrobjartsson A. The uncontrollable placebo effect. Eur J Clin Pharmacol. 1996;50:345–348. doi: 10.1007/s002280050120. [DOI] [PubMed] [Google Scholar]
- 4.Bodemar G, Walan A. Cimetidine in the treatment of active duodenal and prepyloric ulcers. Lancet. 1976;ii:161–164. doi: 10.1016/s0140-6736(76)92342-4. [DOI] [PubMed] [Google Scholar]
- 5.Blackwood WS, Pickard RG, Maudgal DP, Lawrence D, Northfield TC. Cimetidine in duodenal ulcer. Lancet. 1976;ii:174–176. doi: 10.1016/s0140-6736(76)92347-3. [DOI] [PubMed] [Google Scholar]
- 6.Poynard T, Pignon JP. Acute Treatment of Duodenal Ulcer Analyses of 293 Randomized Clinical Trials. Paris: John Libbey Eurotext; 1989. [Google Scholar]
- 7.Gudjonsson B, Spiro HM. Response to placebos in ulcer disease. Am J Med. 1978;65:399–402. doi: 10.1016/0002-9343(78)90761-1. [DOI] [PubMed] [Google Scholar]
- 8.Moerman DE. General medical effectiveness and human biology: placebo effects in the treatment of ulcer disease. Med Anthropol Q. 1983;14:13–16. [Google Scholar]
- 9.Dobrilla G, Scarpignato C. Placebo and placebo effects: their impact on the evaluation of drug response in patients. Dig Dis. 1994;12:368–377. doi: 10.1159/000171471. [DOI] [PubMed] [Google Scholar]
- 10.Laird NM, Mosteller F. Some statistical methods for combining experimental results. Int J Technol Assess Health Care. 1990;6:5–30. doi: 10.1017/s0266462300008916. [DOI] [PubMed] [Google Scholar]
- 11.Hedges LV. Fixed effects models. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 285–299. [Google Scholar]
- 12.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 13.Newman RD, Gitlin N, Lacayo EJ, et al. Misoprostol in the treatment of duodenal ulcer refractory to H2-blocker therapy. Am J Med. 1987;83(Suppl 1A):27–31. doi: 10.1016/0002-9343(87)90575-4. [DOI] [PubMed] [Google Scholar]
- 14.Coronary Drug Project Research Group. Influence of adherence to treatment and response of cholesterol on mortality in the coronary drug project. N Engl J Med. 1980;303:1038–1041. doi: 10.1056/NEJM198010303031804. [DOI] [PubMed] [Google Scholar]
- 15.Braverman AJ. Dose validation and study design criteria in current cimetidine studies. Clin Ther. 1986;8(Suppl A):49–56. [PubMed] [Google Scholar]
- 16.Cloud ML, Offen W, Matsumoto C. Healing and subsequent recurrence of duodenal ulcer in a clinical trial comparing nizatidine 300 mg and 100 mg evening doses and placebo in the treatment of active duodenal ulcer. Curr Ther Res. 1989;45:359–367. [Google Scholar]
- 17.Eliakim R, Stalnikowicz R, Ackerman Z, Karmeli F, Rachmilewitz D. The effect of nizatidine on duodenal ulcer healing and on mucosal inflammation mediators. Isr J Med Sci. 1994;30:751–756. [PubMed] [Google Scholar]
- 18.Euler AR, Baily RJ, Zinny MA, et al. Arbaprostil (15 (R) -15-Methyl Prostaglandin E2) in a single nighttime dose of either 50 or 100 μg in acute duodenal ulcer. Gastroenterology. 1989;97:98–103. doi: 10.1016/0016-5085(89)91421-2. [DOI] [PubMed] [Google Scholar]
- 19.Gilinsky NH, Bright-Asare P, Cobert BL, et al. A multicenter, double-blind, randomized, placebo controlled comparison of nocturnal roxatidine in the treatment of active duodenal ulcer disease. Am J Gastroenterol. 1992;87:847–853. [PubMed] [Google Scholar]
- 20.Gruber CM. Interpreting medical data. Arch Intern Med. 1956;98:767–773. doi: 10.1001/archinte.1956.00250300085010. [DOI] [PubMed] [Google Scholar]
- 21.Rickels K, Hesbacher PT, Weise CC, Gray B, Feldman HS. Pills and improvement: a study of placebo reponse in psychoneurotic outpatients. Psychopharmacologia. 1970;16:318–328. doi: 10.1007/BF00404738. [DOI] [PubMed] [Google Scholar]
- 22.Samuels AS, Edison CB. A study of the psychiatric effects of placebo. J Louisiana State Med Society. 1961;113:114–117. [PubMed] [Google Scholar]
- 23.Ilnyckyj A, Shanahan F, Anton PA, Cheang M, Bernstein CN. Quantification of the placebo response in ulcerative colitis. Gastroenterology. 1997;112:1854–1858. doi: 10.1053/gast.1997.v112.pm9178676. [DOI] [PubMed] [Google Scholar]
- 24.Marshall B. Helicobacter pylori. Am J Gastroenterol. 1994;89:S116–S128. [PubMed] [Google Scholar]