

Abstract
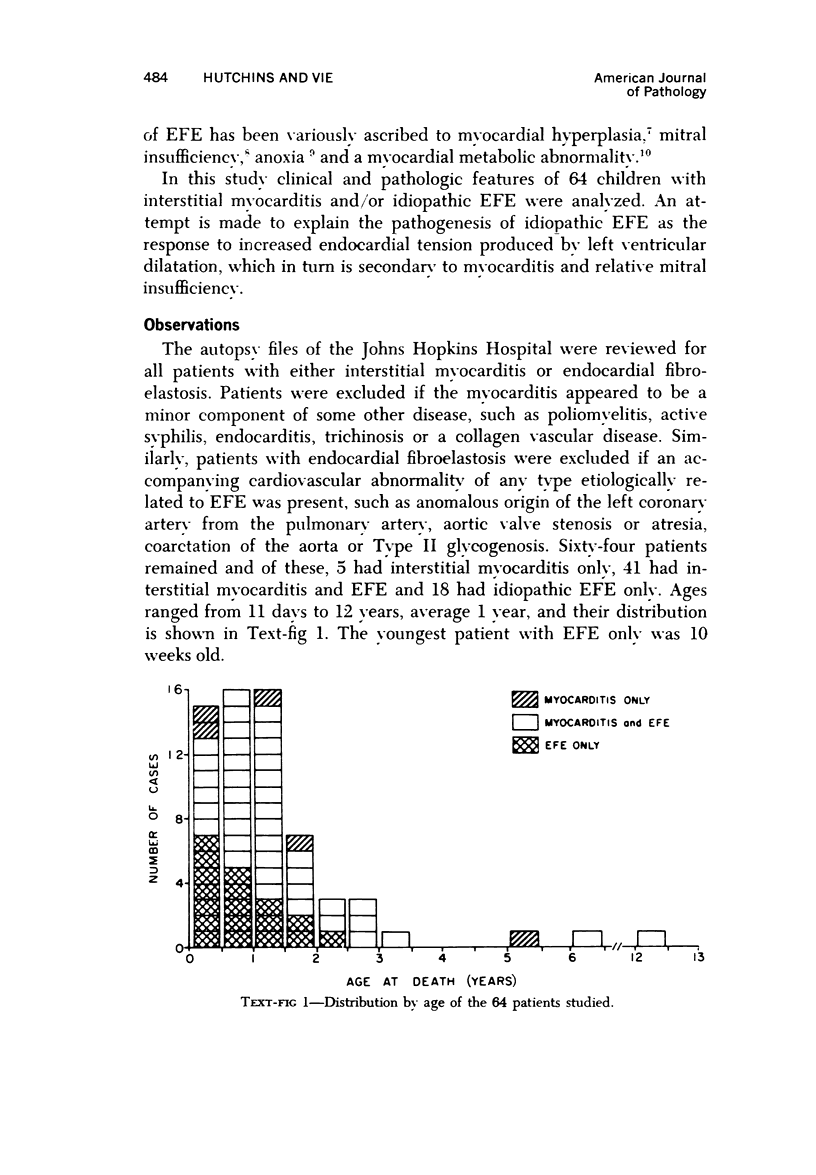
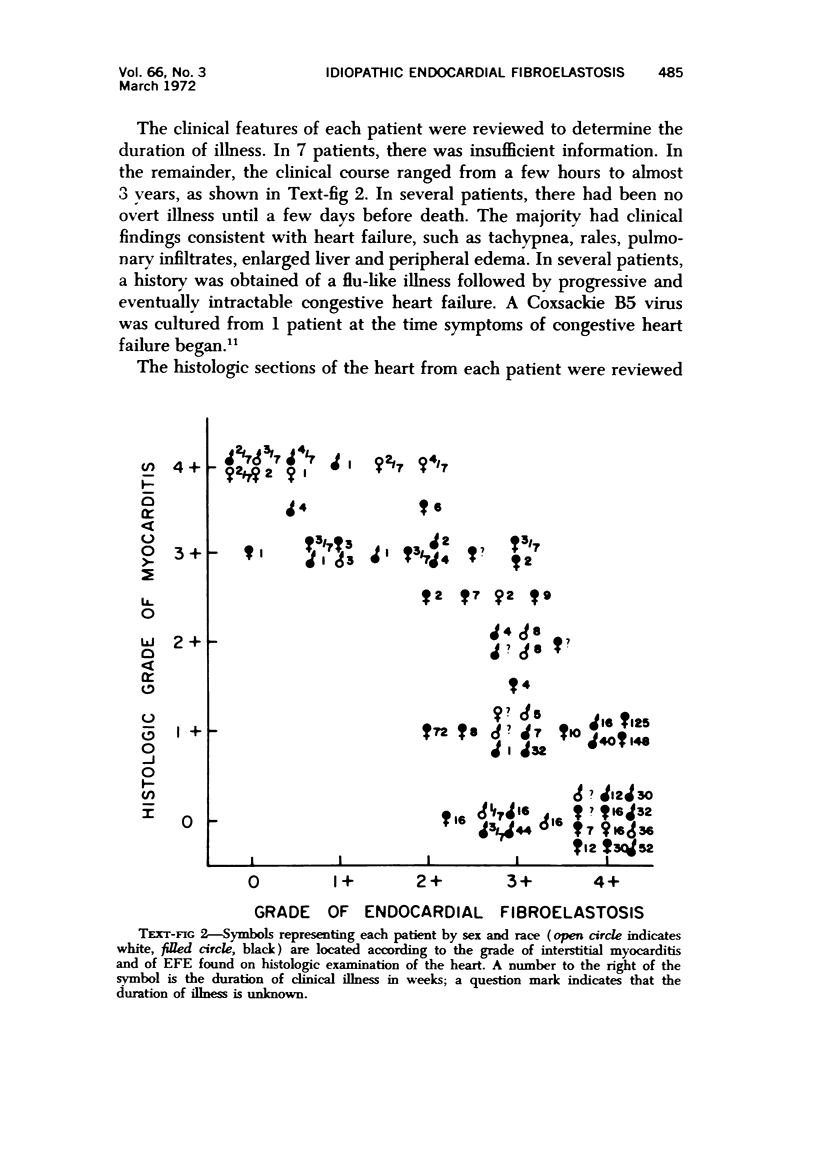
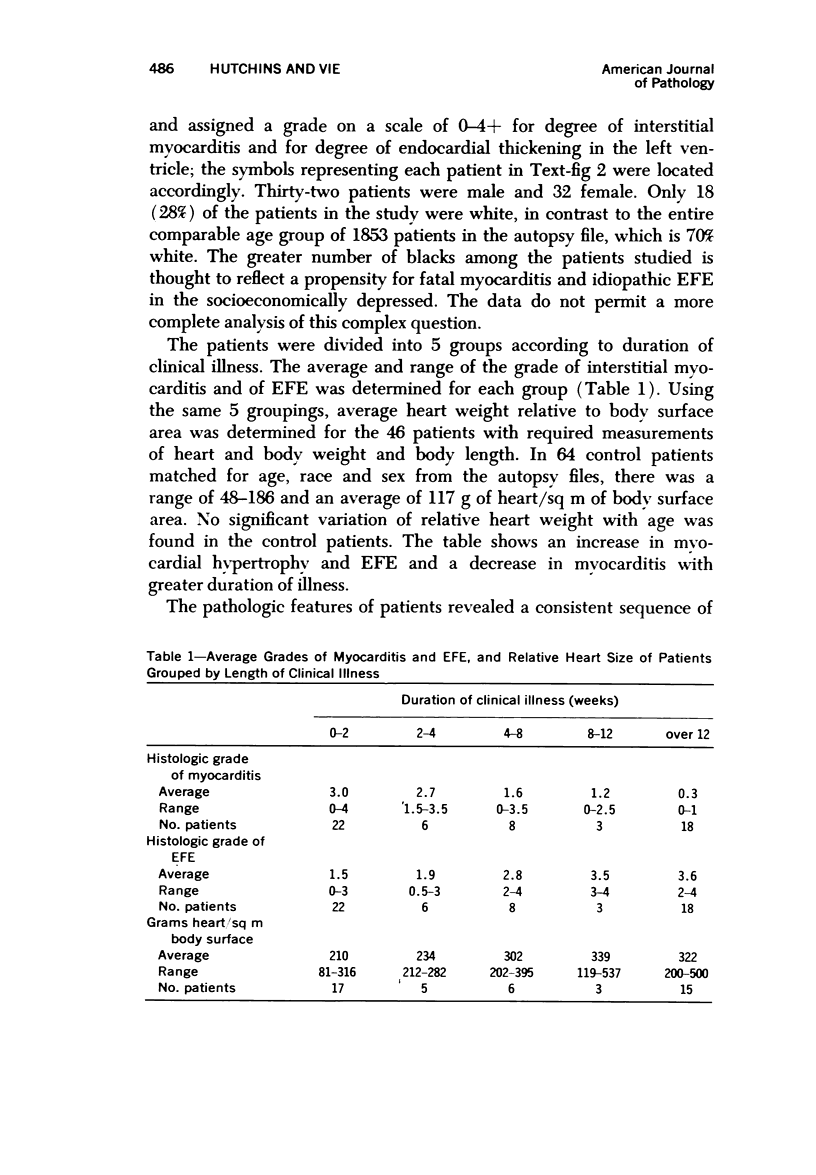
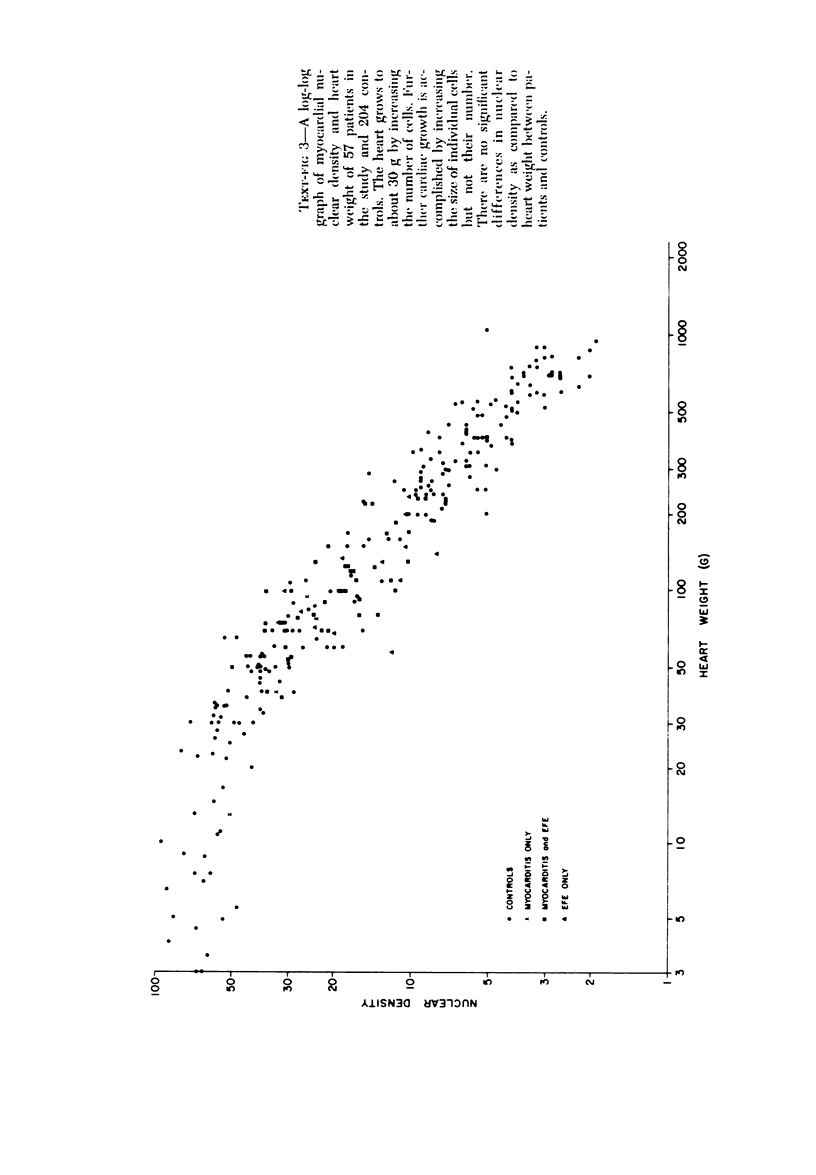
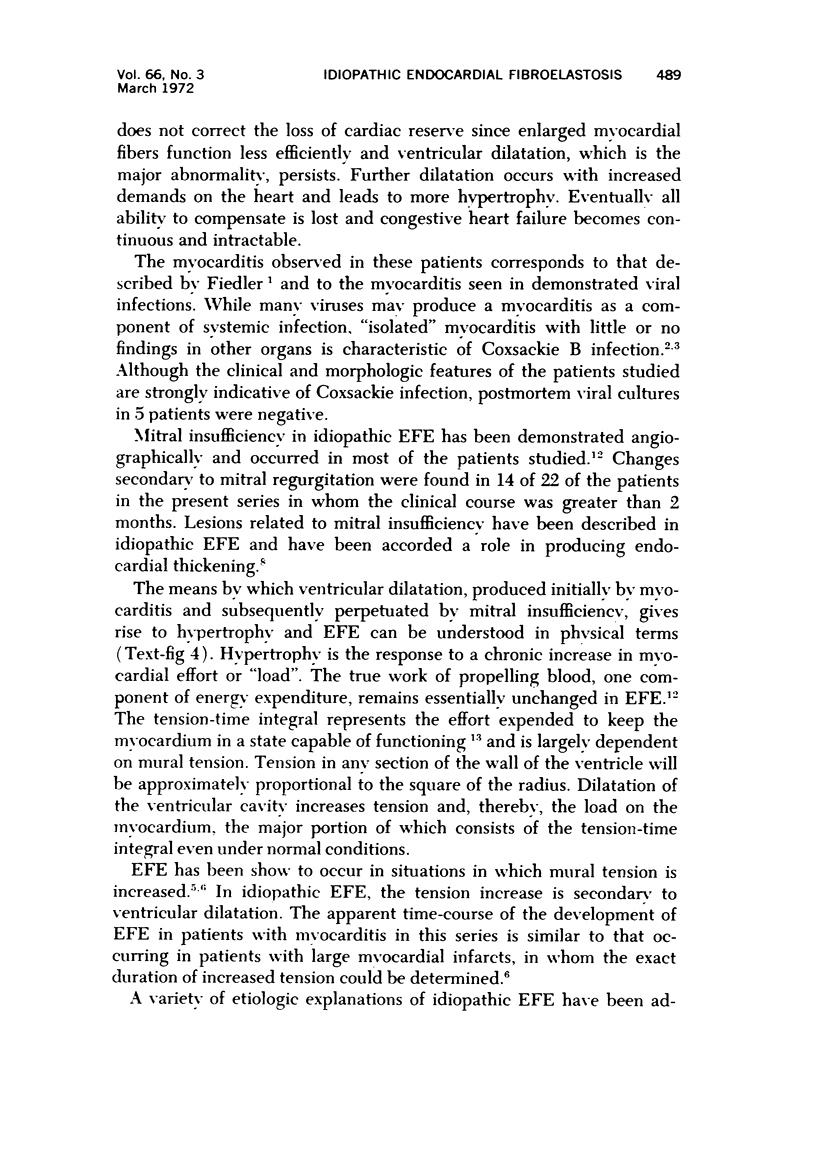
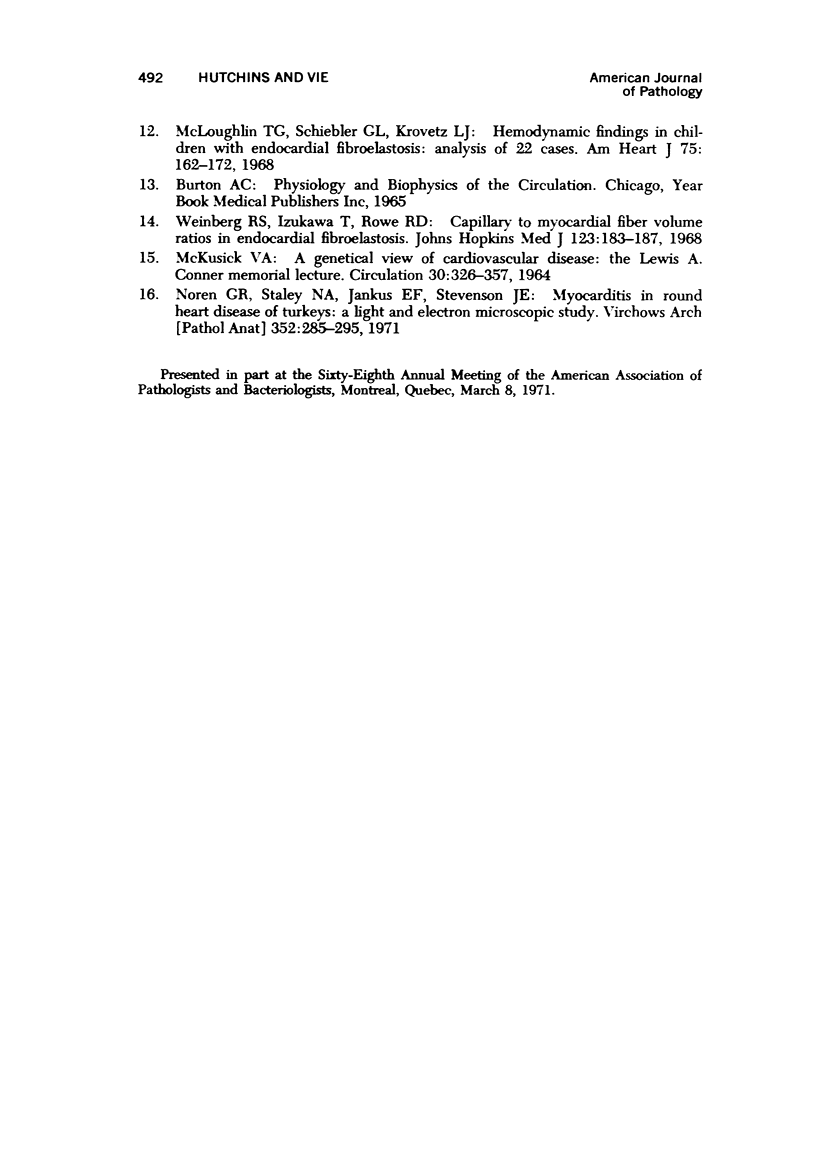
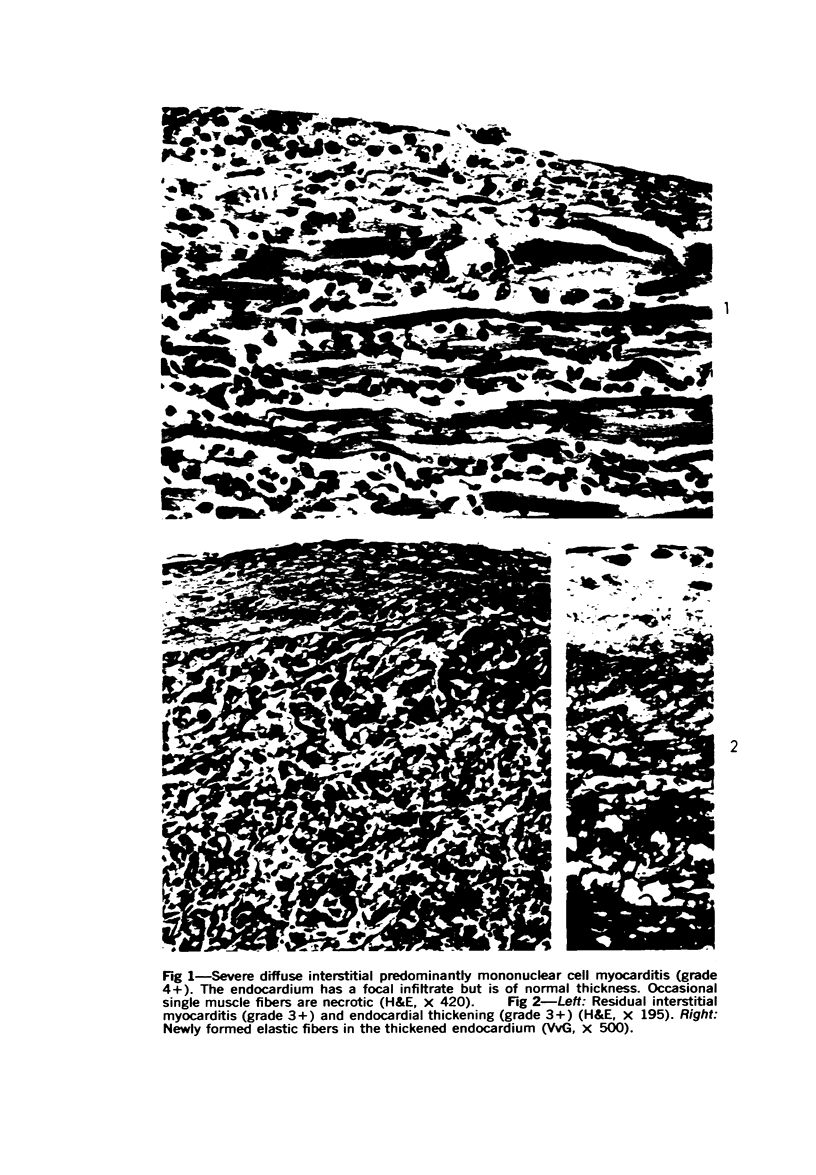
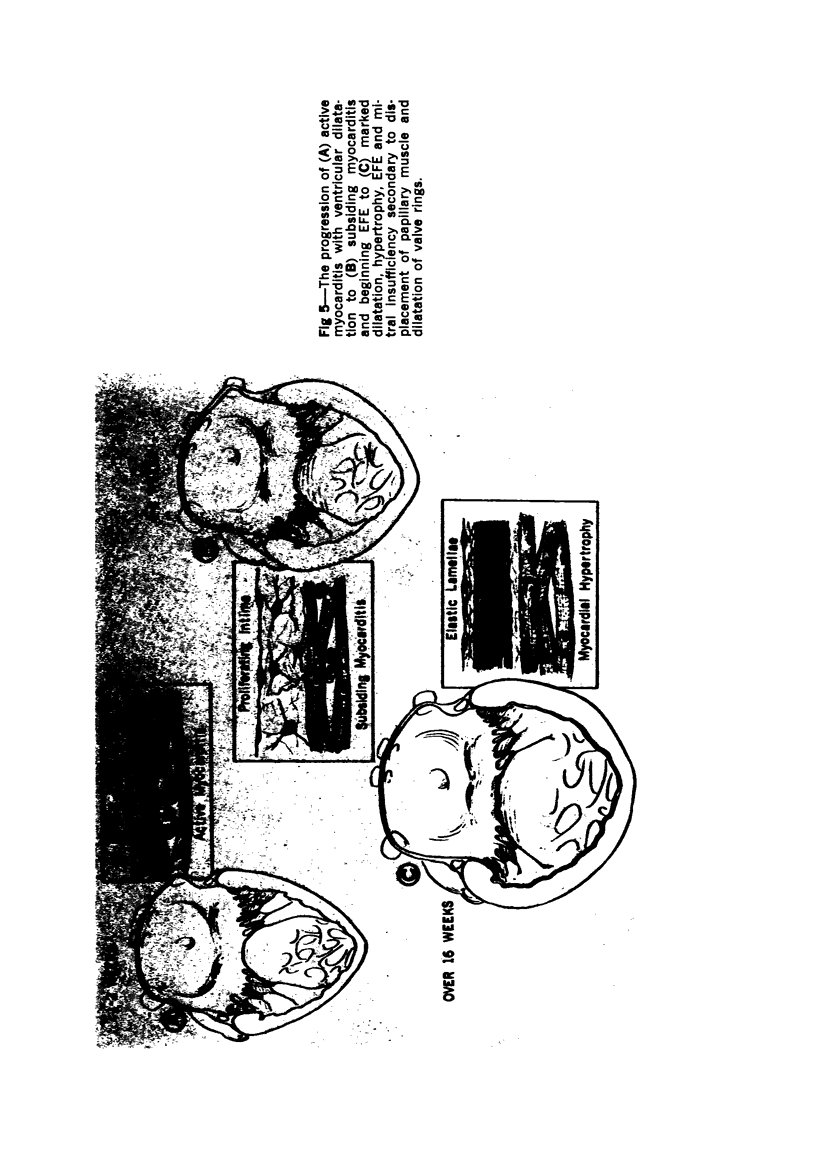
Diffuse interstitial mononuclear cell myocarditis of unidentified but probable viral etiology in patients with endocardial fibroelastosis (EFE) suggested a possible pathogenetic relationship. Clinical and autopsy findings were reviewed in 64 children with one or both conditions. Five had myocarditis only and 18 had idiopathic EFE only, but in 41, both lesions coexisted and demonstrated the progression of myocarditis into idiopathic EFE. Patients with myocarditis but without EFE all died within 2 weeks of the onset of symptoms. With longer survival, myocarditis subsided but EFE and myocardial hypertrophy increased progressively. Marked EFE and hypertrophy, with trivial or no residual myocarditis, occurred with survival times over 4 months. Mitral insufficiency due to ventricular dilatation and a papillary muscle displacement commonly developed with prolonged survival. The results of the study are consistent with the hypothesis that in some patients interstitial myocarditis may produce left ventricular dilatation of a duration sufficient for the development of myocardial hypertrophy and EFE. These nonspecific responses to increased expenditure of myocardial energy and increased mural tension produce ventricular compensation, but result in a marked loss of cardiac reserve. Relative mitral insufficiency perpetuates the cycle of congestive failure and diminishing cardiac reserve by causing further ventricular dilatation with consequent myocardial hypertrophy.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ANDERSEN D. H., KELLY J. Congenital endocardial fibro-elastosis. II. A clinical and pathologic investigation of those cases without associated cardiac malformations including report of two familial instances. Pediatrics. 1956 Oct;18(4):539–555. [PubMed] [Google Scholar]
- BLACK-SCHAFFER B. Infantile endocardial fibroelastosis; a suggested etiology. AMA Arch Pathol. 1957 Mar;63(3):281–306. [PubMed] [Google Scholar]
- BLACK-SCHAFFER B., TURNER M. E. Hyperplastic infantile cardiomegaly; a form of idiopathic hypertrophy with or without endocardial fibroelastosis; and a comment on cardiac atrophy. Am J Pathol. 1958 Jul-Aug;34(4):745–765. [PMC free article] [PubMed] [Google Scholar]
- DE JAGER H., VAN CREVELD S. Myocarditis in newborns, caused by coxsackie virus; clinical and pathological data. Ann Paediatr. 1956 Jul-Aug;187(1-2):100–118. [PubMed] [Google Scholar]
- FRUHLING L., KORN R., LAVILLAUREIX J., SURJUS A., FOUSSEREAU S. [Chronic fibroelastic myoendocarditis of the newborn and the infant (fibroelastosis). New morphological, etiological and pathogenic data. Relation to certain cardiac abnormalities]. Ann Anat Pathol (Paris) 1962 Apr-Jun;7:227–303. [PubMed] [Google Scholar]
- Hutchins G. M., Bannayan G. A. Development of endocardial fibroelastosis following myocardial infarction. Arch Pathol. 1971 Feb;91(2):113–118. [PubMed] [Google Scholar]
- JAVETT S. N., HEYMANN S., MUNDEL B., PEPLER W. J., LURIE H. I., GEAR J., MEASROCH V., KIRSCH Z. Myocarditis in the new newborn infant; a study of an outbreak associated with Coxsackie group B virus infection in a maternity home in Johannesburg. J Pediatr. 1956 Jan;48(1):1–22. doi: 10.1016/s0022-3476(56)80111-x. [DOI] [PubMed] [Google Scholar]
- JOHNSON F. R. Anoxia as a cause of endocardial fibroelastosis in infancy. AMA Arch Pathol. 1952 Sep;54(3):237–247. [PubMed] [Google Scholar]
- MCKUSICK V. A. A GENETICAL VIEW OF CARDIOVASCULAR DISEASE. THE LEWIS A. CONNER MEMORIAL LECTURE. Circulation. 1964 Sep;30:326–357. doi: 10.1161/01.cir.30.3.326. [DOI] [PubMed] [Google Scholar]
- MOLLER J. H., LUCAS R. V., Jr, ADAMS P., Jr, ANDERSON R. C., JORGENS J., EDWARDS J. E. ENDOCARDIAL FIBROELASTOSIS. A CLINICAL AND ANATOMIC STUDY OF 47 PATIENTS WITH EMPHASIS ON ITS RELATIONSHIP TO MITRAL INSUFFICIENCY. Circulation. 1964 Nov;30:759–782. doi: 10.1161/01.cir.30.5.759. [DOI] [PubMed] [Google Scholar]
- McLoughlin T. G., Schiebler G. L., Krovetz L. J. Hemodynamic findings in children with endocardial fibroelastosis. Analysis of 22 cases. Am Heart J. 1968 Feb;75(2):162–172. doi: 10.1016/s0002-8703(68)90060-4. [DOI] [PubMed] [Google Scholar]
- Noren G. R., Staley N. A., Jankus E. F., Stevenson J. E. Myocarditis in round heart disease of turkeys. A light and electron microscopic study. Virchows Arch A Pathol Pathol Anat. 1971;352(4):285–295. doi: 10.1007/BF00542713. [DOI] [PubMed] [Google Scholar]
- Weinberg R. S., Izukawa T., Rowe R. D. Capillary to myocardial fiber volume ratios in endocardial fibroelastosis. Johns Hopkins Med J. 1968 Oct;123(4):183–187. [PubMed] [Google Scholar]