

Abstract
BACKGROUND: We evaluated the association between coffee drinking and the prevalence of type 2 diabetes mellitus in elderly people from the Mediterranean islands. METHODS: During 2005-2007, 500 men and 437 women (aged 65 to 100 years) from the islands of Cyprus (n = 300), Mitilini (n = 142), Samothraki (n = 100), Cephalonia (n = 104), Corfu (n = 160) and Crete (n = 131) participated in the survey. Cardiovascular disease (CVD) risk factors (i.e. hypertension, diabetes, hypercholesterolemia and obesity), as well as behavioral, lifestyle and dietary characteristics were assessed using face-to-face interviews and standard procedures. Among various factors, fasting blood glucose was measured and prevalence of type 2 diabetes mellitus was estimated, according to the established American Diabetes Association (ADA) criteria, while all participants were asked about the frequency of any type of coffee consumption over the last year. RESULTS: Coffee drinking was reported by 84% of the participants, the majority of whom drank boiled coffee. The participants reported that they had consumed coffee for at least 30 years of their life. Data analysis adjusted for various potential confounders, revealed that, compared to non-consumption, the multi-adjusted odds ratio for having diabetes was 0.47 (95%, CI 0.32 to 0.69) for 1-2 cups/day, while it was 1.05 (95%, CI 0.70 to 1.55) for >3 cups/day, after adjusting for various potential confounders. The association of coffee drinking with diabetes was significant only among non-tea drinkers. Increased coffee intake was not associated with diabetes prevalence. CONCLUSION: The data presented suggest that moderate coffee drinking is associated with a lower likelihood of having diabetes, after adjusting for various potential confounders.
Keywords: diabetes mellitus, coffee consumption, tea consumption, elderly individuals
Introduction
Coffee is one of the most commonly consumed beverages around the world. The effect of coffee consumption on human health, especially cardiovascular disease, has been evaluated in many studies, with controversial results [1]. Some of these studies reported a positive association between coffee intake and coronary heart disease risk [2, 3], while other studies reported no relationship [4-7].
One of the potential mechanisms through which coffee drinking may affect coronary risk is the increase in blood pressure and lipid levels and the detrimental effect on aortic stiffness and wave reflections [8, 9]. However, certain studies reported that moderate consumption of coffee was associated with lower blood pressure and cholesterol levels, as well as lower risk of hypertension and diabetes [10-17]. All these data are based mainly on middle-aged populations, where the disease burden is low, while among the elderly, where the burden of disease is high, and nutritional status and needs are associated with age-related biological and often socioeconomic changes, information about the effect of coffee consumption on health is sparse. In addition, epidemiological studies that examine the association between coffee consumption in various quantities and the risk of developing diabetes among elderly people are rather limited in the medical literature and are generally included as subgroups of larger studies performed in the general population.
In the context of the Mediterranean islands (MEDIS) study, therefore, which is a health and nutrition survey in elderly people [18], we sought to evaluate whether coffee consumption is independently associated with fasting blood glucose levels and the prevalence of type 2 diabetes mellitus.
Methods
Participants
A random, population-based, multistage sampling method with age groups (3 levels: 65-75, 75-85, 85+) and gender groups (2 levels: male, female) was used to select 500 men (76 ± 7 years) and 437 women (74 ± 7 years) from the Republic of Cyprus and the islands of Mitilini, Samothraki, Cephalonia, Crete and Corfu in Greece. Individuals residing in assisted living centers were not included in this survey, since the aim of the study was to evaluate lifestyle habits and behavioral characteristics in relation to health indices among free-living people. Moreover, people with a history of cardiovascular disease or cancer, revealed when their medical records were reviewed, were also excluded from sampling, since their medical condition may have altered their lifestyle habits and behaviors. The target sample size was 300 people from Cyprus and 150 from each of the other islands. Of the people initially selected (n = 937), 437 men and 500 women (n = 937) agreed to participate (Cyprus; n = 300, Mitilini; n = 142, Samothraki: n = 100, Cephalonia: n = 114, Crete: n = 131 and Corfu: n = 150). A group of scientists (dietitians, nurses and physicians) with previous experience in field investigation (the MEDIS study group) collected all the required information, using a standard questionnaire.
The retrieved data were confidential and the survey was conducted according to the declaration of the World Medical Association on bio-ethics (52nd WMA General Assembly, Edinburgh, Scotland, October 2000). Before the interview, participants were informed about the aims and procedures of the study and signed a declaration of informed consent.
Measurements
Regarding dietary habits, consumption of 15 food groups and beverages (i.e. meat and meat products, fish and fish products, poultry, milk and other dairy products, fruits, vegetables, greens, legumes, refined and non-refined cereals, coffee, tea and soft-drinks) was measured through a semi-quantitative food-frequency questionnaire, in terms of weekly consumption. All participants were asked about their usual frequency of coffee consumption (i.e. never, < 1 cup per week, 1-2 cups/day, 3-5 cups/day and >5 cups/day) over the previous year. Because the number of participants in the last 2 categories was small, we decided to combine them in all analyses. For the analysis, all types of coffee reported (instant, boiled coffee, "cappuccino" or filtered) were adjusted for one cup of 150 ml coffee and a concentration of 28 mg caffeine per 100 ml. Thus, according to Bunker and McWilliams [19], a measurement of one cup of coffee was equivalent to 450 ml of brewed coffee or 300 ml of instant coffee. We also recorded, and included in the analysis, as dummy variables, consumption of tea and caffeine-containing drinks (such as cola). Moreover, it should be noted that, according to the participants' reports, none of them were taking caffeine as a medication. Consumption of decaffeinated coffee was not analyzed because this product was not frequently consumed in the investigated islands. Consumption of various alcoholic beverages (wine, beer, etc.) was measured in terms of wine glasses adjusted for ethanol intake (e.g. one 100 ml glass of wine was considered to be 12% ethanol). Furthermore, overall assessment of dietary habits was evaluated through a special diet score (MedDietScore, range 0-55), which assesses adherence to the Mediterranean dietary pattern [20, 21]. Higher values on the score indicate greater adherence to this pattern and, consequently, healthier dietary habits.
Physical activity was evaluated using the shortened version of the self-reported International Physical Activity Questionnaire (IPAQ) for the elderly [22]. Frequency (times per week), duration (minutes per time) and intensity of physical activity during sports, occupation and/or free-time activities were assessed. Participants who did not report any physical activity were defined as sedentary. In accordance with the standard IPAQ scoring procedures, physically active participants were classified into one of the following groups: upper tertile: "vigorous" physical activity (< 2500 MET/min/week), middle tertile: "moderate" physical activity (500-2500 MET/min/week) or lower tertile: "low" physical activity (< 500 MET/min/week). Current smokers were defined as those who smoked at least one cigarette per day or had stopped cigarette smoking during the past 12 months. Former smokers were defined as those who previously smoked but had not done so in a year or more. The remaining participants were defined as rare smokers or non-smokers.
The survey also included basic demographic items, such as age, gender, financial status (average annual income during the past three years), educational level (years of school) and various clinical characteristics. Diabetes mellitus type 2 was determined by fasting plasma glucose tests and was analyzed in accordance with the American Diabetes Association diagnostic criteria (fasting blood glucose levels greater than 125 mg/dl (7 mmol/l) or use of special medication, indicated the presence of diabetes) [23]. Weight and height were measured to give body mass index (BMI) scores (kg/m2). Obesity was defined as a BMI < 29.9 kg/m2. Moreover, participants' arterial blood pressure levels were measured when participants were calm and had been in a sitting position for at least 30 minutes. If this procedure was not possible, blood pressure measurements were retrieved from participants' medical records (in 15% of cases). People, who had blood pressure levels ≥ 140/90 mmHg or used antihypertensive medications, were classified as hypertensive. Fasting blood lipids, including triglyceride concentrations, were measured in the majority of the participants using a colorimetric enzymatic method, while in some cases (17% total serum cholesterol levels during the past year) results were retrieved from participant's medical records. Hypercholesterolemia was defined as total serum cholesterol levels >200 mg/dl or the use of lipid-lowering agents. If measurements could not be made, participants' medical records were also consulted to determine high and low density lipoprotein (HDL, LDL) cholesterol and triglyceride levels.
Statistical analysis
The final number of enrolled participants was adequate to evaluate two-tailed standardized differences of greater than 10% on the odds ratio of having diabetes between coffee consumption categories, with statistical power >0.80 and a type I error level (i.e., p-value) of <0.05.
Continuous variables were summarized as mean values ± standard deviation and categorical variables as relative (%) frequencies. After controlling for equality of variances, associations between continuous variables and the coffee-drinking group of participants were evaluated using analysis of variance (ANOVA), while associations between categorical variables and coffee-drinking groups were evaluated using the chi-square test. Relationships between continuous variables were tested with Pearson's correlation coefficient. Multiple linear regression was applied to evaluate the differences between blood glucose levels and coffee consumption categories (using 3 dummy variables: 1 cup/week, 1-2 cups/day, 3+ cups/day), after adjusting for various potential confounders. The interaction of coffee intake with potential confounding factors was also assessed. The assumptions of linearity for the continuous independent variables and constant variance of the standardized residuals were assessed by plotting the residuals against the fitted values. Moreover, multiple logistic regression analysis by the calculation of odds ratio and the corresponding 95% confidence intervals, was used to evaluate the association between coffee intake and the presence of diabetes. Statistical significances < 0.05 from two-sided hypotheses were considered to be statistically significant. All statistical calculations were performed on the SPSS version 14.0 software (SPSS Inc, Chicago, IL, U.S.A.).
Results
The prevalence of type 2 diabetes mellitus in this sample was 19.9% in men and 20.1% in women (p = 0.82). As we can see in Table 1, coffee drinking was reported by 85% of men and 82% of women participants (p = 0.24), while the majority of them (90%) drank boiled coffee (i.e. "Greek type"), 7% consumed unfiltered coffee and 3% consumed filtered coffee. The participants reported that they had consumed coffee for at least 30 years of their life. Men were more heavy coffee consumers compared to women (p < 0.05). Moreover, with the exception of smoking habits, where heavy coffee drinkers were more likely to be smokers compared to non-coffee drinkers, no other differences were found between the coffee consumption groups and various socio-demographic and lifestyle characteristics of the participants (Table 1).
Table 1. Participants' demographic and lifestyle characteristics by coffee consumption group.

Data are mean ± SD and percentages. p from one-way ANOVA (for age, years of school and MedDietScore) and chi-square test (for gender, smoking habits, physical activity status and tea drinking). * p < 0.01 for comparisons between coffee consumption groups vs. non-consumption (Bonferroni corrected).
Table 2 illustrates various clinical and biological characteristics of the participants by coffee consumption category. It can be seen that blood glucose levels were much lower in moderate coffee consumption categories compared to non-consumption or heavier consumption (p = 0.04). Similarly, the prevalence of diabetes was lower in the moderate consumption group compared to no intake or rare intake (p = 0.05), while no differences in the prevalence of diabetes were observed between heavier consumption and non-consumption sub-groups (p = 0.67, Figure 1). Moreover, coffee drinking was positively associated with BMI and obesity, while a parabolic association was observed as regards systolic blood pressure levels (Table 2).
Table 2. Participants' biological and clinical characteristics by coffee consumption group.

Data are mean ± SD and percentages. p from one-way ANOVA (for glucose, blood pressures, cholesterols, triglycerides, body mass index) and chi-square test (for hypertension, diabetes, obesity, hypercholesterolemia, CVD risk factors). No gender differences were observed. † Factors included in this variable were hypertension, diabetes, hypercholesterolemia and obesity. * p < 0.05 and ** p < 0.01 for comparisons between coffee consumption groups vs. non-consumption (Bonferroni corrected).
Figure 1.
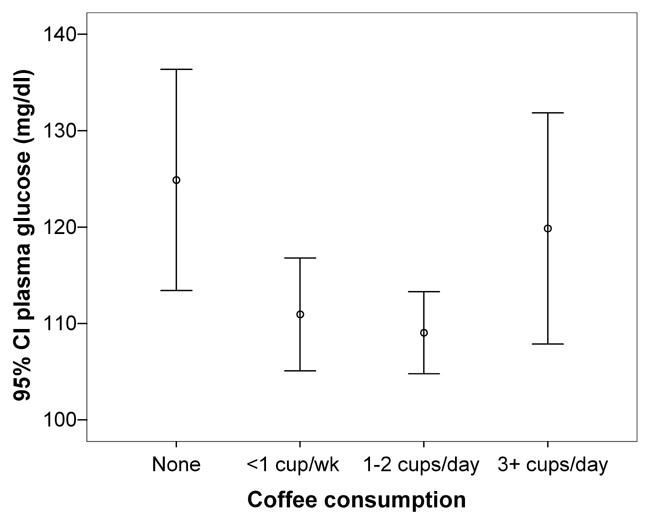
Adjusted mean values for fasting plasma glucose levels by coffee intake category (adjustments were made for age, sex, physical activity status, smoking habits, BMI, presence of hypertension, hypercholesterolemia, family history of diabetes or premature CHD, dietary habits (through the MedDietScore) and tea drinking.
Age- and sex-adjusted logistic regression analysis revealed that coffee drinking of 1-2 cups/day is associated with 0.55 times lower odds of having diabetes (95%, CI 0.30-0.99), while no significant associations were observed between the other coffee intake categories and the prevalence of diabetes. The analysis was later adjusted for various other potential confounders, such as age, sex, physical activity status, smoking habits, BMI, presence of hypertension, hypercholesterolemia, family history of diabetes or premature CHD, dietary habits (through the MedDietScore) and tea drinking. Compared to non-consumption, the multi-adjusted odds ratio of having diabetes was 0.47 (95%, CI 0.32-0.69) for 1-2 cups/day, while it was 1.05 (95%, CI 0.70-1.55) for 3 or more cups/day, indicating that only moderate coffee drinking was associated with a lower likelihood of having diabetes, after adjusting for various potential confounders. Moreover, linear regression analysis revealed that coffee consumption of 1-2 cups/day was associated with about 17 mg/dl reduction in fasting blood glucose levels (p < 0.01), while rare coffee intake showed no significant results, after various adjustments had been made (Table 3).
Table 3. Results from multiple linear regression analysis that evaluated the association between coffee consumption (in cups/day) and levels of fasting blood glucose (dependent outcome).
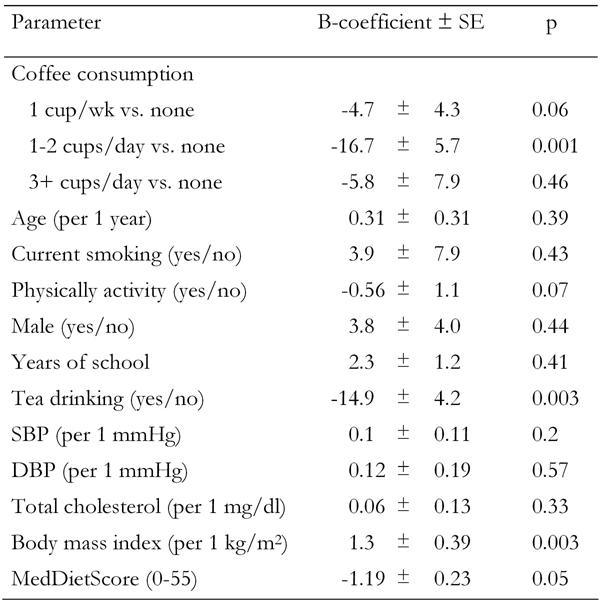
Data are mean ± SD. p from one-way ANOVA. Adjusted R2 with/without coffee intake variable in the mode: 4.1%/2.9%. SE: standard error. SBP: systolic blood pressure. DBP: diastolic blood pressure.
However, a significant interaction was observed between tea and coffee consumption (p < 0.0001). When the analysis was stratified by tea intake category (i.e. tea drinkers and non-drinkers), it showed that compared to drinking no coffee, drinking 1-2 cups of coffee daily was associated with -18.2 ± 4.0 mg/dl decrease in fasting blood glucose levels among non-consumers of tea (p = 0.001). A non-significant association was observed between any category of coffee intake and blood glucose levels in people who reported that they also consumed tea after various adjustments were made (<1 cup/week vs. none: -9.2 ± 4.3 mg/dl, p = 0.17, 1-2 cups/week vs. none: -12.2 ± 3.7 mg/dl, p = 0.07, 3+ cups/week vs. none: -3.2 ± 7.2 mg/dl, p = 0.89).
Discussion
The major finding of this study was that moderate coffee drinking (1-2 cups/day) was found to be associated with a lower likelihood of having diabetes, while no significant relationship was observed when increased consumption was taken into account. Moreover, the effect of coffee intake on fasting blood glucose levels was significant only among participants who did not consume tea. Tea consumption seemed to mask the influence of coffee drinking on blood glucose levels. This is one of the first studies in the literature to show a relationship between coffee drinking and diabetes among the elderly, where the disease burden is high and nutritional status is often associated with age-related biological and other socioeconomic conditions.
Evidence from previous epidemiologic studies suggests that moderate coffee drinking (up to 3-4 cups per day) may confer a protective effect on cardiovascular disease risk, possibly because coffee contains polyphenols (chlorogenic and caffeic acids), which may have antioxidant properties [5, 10, 24]. In a recent study among elderly people, the authors concluded that moderate coffee drinking (<3 cups per day) did not increase the risk of myocardial infarction [25]. However, regarding coffee drinking and diabetes, the available information in the literature is very sparse. In an 11-year follow-up study of about 28000 post-menopausal women, the investigators reported that coffee drinking, especially decaffeinated coffee, was inversely associated with the risk of diabetes [26]. Similar results were reported by the Nurses' Health Study and the Health Professionals' Follow-up Study [27], where the investigators suggested an inverse relationship, independent of known confounders, between the risk of diabetes and coffee drinking.
In our work, moderate coffee drinking was associated with a reduced likelihood of having type 2 diabetes and lower levels of blood glucose. However, the latter association was significant only among people who did not consume tea. The polyphenols contained in tea appeared to mask the association between coffee and glucose levels. The novelty of our findings is that they were obtained from an elderly population, living in the Mediterranean islands, where the consumption of polyphenols and other anti-oxidants is very high, and there is evidence of the antioxidative effect of herbs that are consumed as a hot tea on the island of Crete [28]. Thus, the intake of these protective nutrients from other food sources did not alter the relationship between long-term coffee drinking and diabetes. Based on the previously mentioned findings, it could be suggested that consumption of coffee is associated with a lower risk of type 2 diabetes, which suggests that coffee constituents other than caffeine may play a protective role. It has been suggested that caffeine increases basal energy expenditure and that this thermogenic effect has a dose-response relationship with the amount of coffee consumed [29]. Moreover, chlorogenic and caffeic acids may be a key point in this relationship. However, further research on phytochemicals in coffee may lead to the identification of novel mechanisms clarifying the effects of diet on the development of diabetes, as van Dam suggested [30].
There are others who suggest that increased incidence of coronary heart disease is associated with increasing coffee consumption. In particular, in a prospective study from Finland, Happonen et al. [13] found that heavy coffee consumption (>814 ml/day) increased the rates of acute myocardial infarction or coronary death, after a 14-year mean follow-up, independent of the brewing method or currently recognized cardiovascular risk factors. Also, in a mean follow-up of 6.4 years, Tverdal et al. [31] found that consuming nine or more cups of coffee per day increased the risk of coronary heart disease mortality by 2.2 times in men and 5.1 times in women, over and above its effect in raising cholesterol concentrations. Some investigators also attributed the development of arrhythmias to the harmful effect of coffee [16]. However, there is not enough evidence in humans that caffeine, at the doses typically consumed, can provoke any spontaneous arrhythmia [32]. Furthermore, coffee drinking may also, through caffeine, raise blood pressure levels in patients who are infrequently exposed [33], but acute caffeine intake has little or no effect in habitual coffee drinkers [8].
Limitations
This study is cross-sectional and, consequently, has potential for recall biases, particularly in the assessment of dietary habits. Thus, although important associations were assessed, the design of this study prohibits causal interpretations. Moreover, people living in the Mediterranean islands are not a representative sample of the total population. They could be considered a population that has been a "closed" population for a long time and, therefore, unaffected by the influence of westernized habits. Also, it could be suggested that increased consumption of coffee is associated with unhealthy behaviors, such as physical inactivity, unhealthier dietary habits, and smoking. In the present work, these potential confounders were statistically controlled but, as always, residual confounding cannot be explained. The majority of the participants consumed unfiltered, boiled coffee, which meant that the actual association of filtered coffee with the presence of diabetes could not be evaluated in our study. Furthermore, because coffee consumption and physician-diagnosed diabetes were self-reported, some misclassification of exposure and outcome was to be expected. In cross-sectional studies, however, this kind of misclassification would have biased the results toward the null hypothesis. Finally, in some cases, information about participants' clinical characteristics was not measured but retrieved from individuals' medical records. We believe, however, that this did not alter the significance of our findings, since we made an effort to collect accurate information regarding participants' medical history.
Conclusions
Coffee is a widespread beverage in our sample, as it is in most of the world. The results presented, suggest that moderate, long-term coffee drinking seems to be associated with lower prevalence of type 2 diabetes among elderly men and women living in the Mediterranean islands. The latter association is independent of smoking, physical activity status, body mass, and various dietary habits. Tea consumers, however, showed less striking results. Our findings suggest an important relationship between the dietary habits and health status of elderly people, who have an increased disease burden and whose dietary habits are often associated with age-related biological and socioeconomic conditions [34]. The study clearly shows that, in coffee studies, it is important to regard tea consumption as an important aspect in the prevention of diabetes and cardiovascular disease. However, further metabolic studies are needed in order to investigate the long-term effects of coffee and tea intake on glucose homeostasis and insulin resistance.
Acknowledgments
We are particularly grateful to the men and women from the islands of Cyprus, Mitilini, Samothraki, Crete, Corfu and Cephalonia, who participated in and collaborated on this survey. We also wish to express our gratitude to the following: M. Tornaritis, A. Polystipioti, N. Papairakleous and S. Papoutsou (field investigators from Cyprus), K. Gelastopoulou (field investigator from Mitilini), F. Anastasiou, E. Ladoudaki and M. Antonopoulou (field investigators from Crete), E. Niforatou, V. Alpentzou, M. Voutsadaki and M. Galiatsatos (field investigators from Cephalonia) and E. Lioliou and K. Voutsa (field investigators from Corfu) for their substantial assistance in the enrolment of the participants. Moreover, the study was funded by research grants from the Hellenic Heart Foundation and, therefore, we should also like to thank Prof. Pavlos Toutouzas, Director of the Foundation.
References
- 1.Sofi F, Conti AA, Gori AM, Eliana Luisi ML, Casini A, Abbate R, Gensini GF. Coffee consumption and risk of coronary heart disease: A meta-analysis. Nutr Metab Cardiovasc Dis. 2007;17(3):209–223. doi: 10.1016/j.numecd.2006.07.013. [DOI] [PubMed] [Google Scholar]
- 2.Grobbee DE, Rimm EB, Giovannucci E, Colditz G, Stampfer M, Willett W. Coffee, caffeine, and cardiovascular disease in men. New Eng J Med. 1990;323:1026–1032. doi: 10.1056/NEJM199010113231504. [DOI] [PubMed] [Google Scholar]
- 3.Klag MJ, Mead LA, La Croix AZ, Wang NY, Coresh J, Liang KY, Pearson TA, Levine DM. Coffee intake and coronary heart disease. Ann Epidemiol. 1994;4:425–433. doi: 10.1016/1047-2797(94)90001-9. [DOI] [PubMed] [Google Scholar]
- 4.Palmer JR, Rosenberg L, Rao RS, Shapiro S. Coffee consumption and myocardial infarction in women. Am J Epidemiol. 1995;141:724–731. doi: 10.1093/oxfordjournals.aje.a117494. [DOI] [PubMed] [Google Scholar]
- 5.Kleemola P, Jousilahti P, Pietinen P, Vartiainen E, Tuomilehto J. Coffee consumption and the risk of coronary heart disease and death. Arch Intern Med. 2000;160(22):3393–3400. doi: 10.1001/archinte.160.22.3393. [DOI] [PubMed] [Google Scholar]
- 6.Cannon ME, Cooke CT, McCarthy JS. Caffeine-induced cardiac arrhythmia: an unrecognized danger of healthfood products. Med J Aust. 2001;174:520–521. doi: 10.5694/j.1326-5377.2001.tb143404.x. [DOI] [PubMed] [Google Scholar]
- 7.Gyntelberg F, Hein HO, Suadicani P, Sorensen H. Coffee consumption and risk of ischemic heart disease - a settled issue? J Intern Med. 1995;237:55–61. doi: 10.1111/j.1365-2796.1995.tb01140.x. [DOI] [PubMed] [Google Scholar]
- 8.Corti R, Binggeli C, Sudano I, Spieker L, Hanseler E, Ruschitzka F, Chaplin WF, Luscher TF, Noll G. Coffee acutely increases sympathetic nerve activity and blood pressure independently of caffeine content: role of habitual versus non habitual drinking. Circulation. 2002;106:2935–2940. doi: 10.1161/01.cir.0000046228.97025.3a. [DOI] [PubMed] [Google Scholar]
- 9.Vlachopoulos C, Panagiotakos D, Ioakeimidis N, Dima I, Stefanadis C. Chronic coffee consumption has a detrimental effect on aortic stiffness and wave reflections. Am J Clin Nutr. 2005;81:1307–1312. doi: 10.1093/ajcn/81.6.1307. [DOI] [PubMed] [Google Scholar]
- 10.Panagiotakos DB, Pitsavos C, Chrysohoou C, Kokkinos P, Toutouzas P, Stefanadis C. The J-shaped effect of coffee consumption on the risk of developing acute coronary syndromes: The CARDIO2000 case-control study. J Nutr. 2003;133:3228–3232. doi: 10.1093/jn/133.10.3228. [DOI] [PubMed] [Google Scholar]
- 11.Myers MG, Basinski A. Coffee and coronary heart disease. Arch Intern Med. 1992;152:1767–1772. [PubMed] [Google Scholar]
- 12.Heyden S, Tyroler HA, Heiss G, Hames CG, Bartel A. Coffee consumption and mortality: total mortality, stroke mortality and coronary heart disease mortality. Arch Intern Med. 1978;138:1472–1475. [PubMed] [Google Scholar]
- 13.Happonen P, Voutilainen S, Salonen JT. Coffee drinking is dose-dependently related to the risk of acute coronary events in middle-aged men. J Nutr. 2004;134:2381–2386. doi: 10.1093/jn/134.9.2381. [DOI] [PubMed] [Google Scholar]
- 14.Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam. 2003;20:1–30. doi: 10.1080/0265203021000007840. [DOI] [PubMed] [Google Scholar]
- 15.de Roos B, Katan MB. Possible mechanisms underlying the cholesterol-raising effect of the coffee diterpene cafestol. Curr Opin Lipidol. 1999;10:41–45. doi: 10.1097/00041433-199902000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Mehta A, Jain AC, Mehta MC, Billie M. Caffeine and cardiac arrhythmias. An experimental study in dogs with review of literature. Acta Cardiol. 1997;52:273–283. [PubMed] [Google Scholar]
- 17.van Dam RM, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Dietary patterns and risk for type 2 diabetes mellitus in US men. Ann Intern Med. 2002;136:201–209. doi: 10.7326/0003-4819-136-3-200202050-00008. [DOI] [PubMed] [Google Scholar]
- 18.Polychronopoulos E, Panagiotakos D, Polystipioti A. Diet, lifestyle factors and hypercholesterolemia in elderly men and women from Cyprus. Lipids Health Dis. 2005;4:17. doi: 10.1186/1476-511X-4-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bunker ML, McWilliams M. Caffeine content of common beverages. J Am Diet Assoc. 1979;74:28–32. [PubMed] [Google Scholar]
- 20.Panagiotakos DB, Pitsavos C, Stefanadis C. Dietary Patterns: a Mediterranean diet score and its relation to CVD risk and markers. Nutr Metab Cardiovasc Dis. 2006;16:559–568. doi: 10.1016/j.numecd.2005.08.006. [DOI] [PubMed] [Google Scholar]
- 21.Panagiotakos DB, Pitsavos C, Arvaniti C, Stefanadis C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev Med. 2007;44(4):335–340. doi: 10.1016/j.ypmed.2006.12.009. [DOI] [PubMed] [Google Scholar]
- 22.Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- 23.Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 1997;20:1183–1197. doi: 10.2337/diacare.20.7.1183. [DOI] [PubMed] [Google Scholar]
- 24.Laranjinha JA, Almeida LM, Madeira VM. Reactivity of dietary phenolic acids with peroxyl radicals: antioxidant activity upon low density lipoprotein cholesterol peroxidation. Biochem Pharmac. 1994;48:487–494. doi: 10.1016/0006-2952(94)90278-x. [DOI] [PubMed] [Google Scholar]
- 25.Rosner SA, Akesson A, Stampfer MJ, Wolk A. Coffee consumption and risk of myocardial infarction among older Swedish women. Am J Epidemiol. 2007;165:288–293. doi: 10.1093/aje/kwk013. [DOI] [PubMed] [Google Scholar]
- 26.Pereira MA, Parker ED, Folsom AR. Coffee consumption and risk of type 2 diabetes mellitus: an 11-year prospective study of 28812 postmenopausal women. Arch Intern Med. 2006;166:1311–1316. doi: 10.1001/archinte.166.12.1311. [DOI] [PubMed] [Google Scholar]
- 27.Salazar-Martinez E, Willett WC, Ascherio A, Manson JE, Leitzmann MF, Stampfer MJ, Hu FB. Coffee consumption and risk for type 2 diabetes mellitus. Ann Intern Med. 2004;140:1–8. doi: 10.7326/0003-4819-140-1-200401060-00005. [DOI] [PubMed] [Google Scholar]
- 28.Lionis C, Faresjo A, Faresjo T, Skoula M, Kapsokefalou M. Antioxiadant effects of various herbs common in rural Crete. Lancet. 1998;352:1987–1988. doi: 10.1016/S0140-6736(05)61333-5. [DOI] [PubMed] [Google Scholar]
- 29.Astrup A, Toubro S, Cannon S, Hein P, Breum L, Madsen J. Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers. Am J Clin Nutr. 1990;51:759–767. doi: 10.1093/ajcn/51.5.759. [DOI] [PubMed] [Google Scholar]
- 30.van Dam RM. Coffee and type 2 diabetes: from beans to beta-cells. Nutr Metab Cardiovasc Dis. 2006;16:69–77. doi: 10.1016/j.numecd.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 31.Tverdal A, Stensvold I, Solvoll K, Foss OP, Lund-Larsen P, Bjartveit K. Coffee consumption and death from coronary heart disease in middle aged Norwegian men and women. BMJ. 1990;300:566–569. doi: 10.1136/bmj.300.6724.566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Frost L, Vestergaard P. Caffeine and risk of atrial fibrillation or flutter: the Danish diet, cancer and health study. Am J Clin Nutr. 2005;81:578–582. doi: 10.1093/ajcn/81.3.578. [DOI] [PubMed] [Google Scholar]
- 33.Green PJ, Kirby R, Suls J. The effects of caffeine on blood pressure and heart rate: a review. Ann Behav Med. 1996;18:201–216. doi: 10.1007/BF02883398. [DOI] [PubMed] [Google Scholar]
- 34.Lionis C, Bathianaki M, Antonakis N, Papavasiliou S, Philalithis A. A high prevalence of diabetes mellitus in a Municipality of rural Crete, Greece. Some results from a primary care study. Diab Med. 2001;18:1–2. doi: 10.1046/j.1464-5491.2001.00526.x. [DOI] [PubMed] [Google Scholar]