

Abstract
Objective
The purposes of this investigation were (1) to describe postpartum drinking patterns among women who were frequent drinkers before pregnancy and (2) to identify factors correlated with postpartum “risky” drinking among women who were frequent drinkers before pregnancy.
Method
Information was gathered through a self-administered questionnaire completed at the postpartum visit and a subsequent face-to-face interview of 381 women, recruited from 35 obstetric/gynecologic clinics throughout Wisconsin, who reported frequent drinking before pregnancy. Multivariate analyses were used to identify correlates of postpartum risky drinking, defined as consuming four or more drinks per occasion (heavy episodic drinking) at least twice in the past 28 days or drinking an average of seven or more drinks per week.
Results
Overall, 37.8% (n = 144) women reported postpartum risky drinking. Eighteen percent reported heavy episodic drinking only, 5% reported frequent drinking only, and 15% reported both behaviors. Postpartum risky drinkers were more likely than other women to have had a partner who engaged in risky drinking (odds ratio [OR] = 2.6, 95% confidence interval [CI]: 1.5–4.5), to have been unemployed (OR = 3.0, 95% CI: 1.2–7.7), to have smoked following pregnancy (OR = 1.9, 95% CI: 1.0–3.5), and to have consumed alcohol after the recognition of pregnancy (OR = 4.8, 95% CI: 2.2–10.6). Women who breast-fed their child were less likely to report risky drinking (OR = 0.3, 95% CI: 0.2–0.5).
Conclusions
In the postpartum period, health care providers may want to focus alcohol screening efforts on former frequent drinkers who are smokers, are unemployed, have a partner who is a risky drinker, or are not breast-feeding.
The consumption of alcohol by mothers during and after pregnancy can have important effects on the developing child. It is estimated that roughly 1 in 100 children has a fetal alcohol spectrum disorder (May and Gossage, 2001). Because of the potential adverse effects of gestational alcohol on the fetus, the U.S. surgeon general has recommended that women who are pregnant or may become pregnant abstain from alcohol (Office of Surgeon General, 2005). Yet, in the United States, more than half of women who might become pregnant report drinking alcohol (Centers for Disease Control and Prevention, 2002). Although women generally reduce their alcohol consumption once pregnancy is recognized, they typically return to their baseline drinking patterns following the birth of a child (Fried et al, 1985).
Maternal drinking can negatively impact families in a variety of ways. Frequent, heavy maternal drinking is associated with poorer family functioning, poorer intellectual stimulation, and increased domestic violence (Jester et al., 2000). Mothers with alcohol dependence are more likely to report punitive behaviors toward their children (Miller et al., 1999). Although not specific to alcohol, a study by Whitaker (2006) documented an increased likelihood of childhood behavior problems among children whose mothers had co-occurring mental-health, substance-use, and domestic-violence conditions. This association persisted even after prenatal exposures and paternal mental health and substance use were controlled for. Furthermore, among women who drink during their pregnancies, the likelihood of having a child with fetal alcohol syndrome increases with subsequent pregnancies (May et al., 2004). Thus, the identification of mothers with risky drinking is a critical step toward the prevention of fetal alcohol spectrum disorders.
Although research on women’s drinking patterns before and during pregnancy exists (Flynn et al., 2003; Floyd et al., 1999; Tough et al., 2006), less is known about women’s drinking habits in the postpartum period. A study by Fried et al. (1985) of nearly 300 Canadian women demonstrated a significant reduction in alcohol intake and heavy episodic drinking during pregnancy. By 12 months postpartum, however, heavy episodic drinking had returned to baseline levels, and most women had returned to their prepregnancy drinking levels. An exception to this pattern occurred among heavy social drinkers who, at the 12-month follow-up, reported drinking less than they did before pregnancy. A similar pattern of reduced drinking during pregnancy, followed by a steady increase after the birth of a child, has been noted among unmarried adolescents (Gilchrest et al., 1996). The steady rise in alcohol use was most notable during the first 6 months postpartum.
Although those studies have documented the trajectory of drinking during and after pregnancy, few studies have explored the differences between women who return to risky drinking in the postpartum period and those who do not. The goals of our study were (1) to describe the postpartum drinking patterns of women who were frequent drinkers before pregnancy and (2) to identify differences between women who report a risky pattern of drinking following the birth of a child and those who either abstain from alcohol or drink at a low-risk level.
Method
Overview
The epidemiologic data used for this report were obtained from the recruitment phase of a randomized clinical trial designed to test the efficacy of a brief alcohol intervention among postpartum women. Subjects were recruited from 35 obstetrical practices located throughout Wisconsin. The practices were selected based on a number of factors, including geographical location, willingness of the physicians to participate in the study, and prior professional relationship with the second author (MF).
The data for this report were obtained from two sources. The first source was the Health Screening Survey-A (HSS-A). The Health Screening Surveys were developed in England in the late 1970s as general health questionnaires to screen primary-care samples for high-risk drinking (Wallace and Haines, 1985). These instruments were further validated by the second author and his research group in the United States in the early 1990s (Fleming and Barry, 1991). The HSS-A has been used by the second author ok to estimate the prevalence of alcohol-use disorders in a general adult sample (Fleming et al., 1998). The HSS-A contains screening questions on exercise, smoking, and alcohol use. Women completed the survey in the clinic waiting room before their postpartum visit. On average (SD), the survey was completed on Postpartum Day 45 (14.1). The response rate varied by clinic and ranged from 85% to 95%.
The second source of data was a face-to-face interview with women who screened positive for risky drinking on the HSS-A. Six field researchers working in the 35 practices conducted the interviews. On average, the interview occurred at 98 days postpartum. The interview consisted of questions related to exercise, smoking, and alcohol use before, during, and after pregnancy. A 28-day Timeline Followback procedure (Sobell and Sobell., 1992). was used to assess current alcohol use during the postpartum period. Reference added to list, please format as needed. Alcohol use before and during pregnancy was assessed using frequency and quantity questions. Additional questions were asked about depression, partner alcohol use, breast-feeding, interpersonal violence, health disparities, employment status, family history, alcohol harm, and health care use.
The sample used for this report consisted of 381 women who reported drinking seven or more drinks per week before pregnancy on the screening survey and completed the subsequent face-to-face interview.
The outcome of interest was postpartum risky drinking, defined as consumption of four or more drinks per occasion (heavy episodic drinking) at least twice in the past 28 days or drinking an average of seven or more drinks per week. These outcomes were assessed using the Timeline Followback procedure during the face-to-face interview.
To identify correlates of postpartum risky drinking, variables related to sociodemographic characteristics, postpartum characteristics, alcohol-related characteristics, and emotional/physical abuse were created and entered into a logistic regression model. Sociodemographic variables included age, which was divided into three categories: 18–25 years, 26–35 years, and 36 years and older. Four race/ethnicity categories were created: white non-Hispanic, black non-Hispanic, multiracial/ethnic (changed in both text and table to better describe the group), and other race. The multiracial/ethnic category included women reporting Hispanic ethnicity as well as women reporting two or more races. The “other race” category included small numbers of women who reported Asian, American Indian, or “other race” on the HSS-A.
Additional variables included being married versus being unmarried; having some college education versus having no college education; and employment status, which was coded into three categories: employed (both part time and full time), unemployed, and not in the labor force (referring to stay-at-home mothers, students, and seasonal workers).
Variables unique to the postpartum period included self-report of any smoking postpartum versus no smoking, any breast-feeding in the past 7 days versus no breast-feeding, having two or more children versus having one or no children, and having postpartum depression versus not having it. Postpartum depression was defined as scoring greater than 12 on the Edinburgh Postnatal Depression Scale (Cox et al., 1987).
Alcohol-related variables included reporting any alcohol use after the recognition of pregnancy versus not reporting any, having a partner engaged in risky drinking versus not having such a partner, having a relative with drug or alcohol problems versus not having such a relative, and reporting the receipt of alcohol counseling by a doctor or nurse within the past 12 months versus not reporting any.
Partner risky drinking was defined as a subject’s report of a partner consuming (1) an average of seven or more drinks per week or (2) five or more drinks on one occasion at least twice in the past 30 days. Family history of alcohol or drug problems was assessed using the question “Has anyone in your family ever had an alcohol or other drug problem?” Alcohol-related counseling by a doctor or nurse was defined as advice offered by a clinician regarding the patient’s alcohol consumption. A clinician’s merely inquiring as to how much alcohol was consumed did not fulfill this criterion.
Physical and emotional abuse was assessed with the following questions, respectively: “Within the last 12 months, have you been emotionally abused? (some examples of emotional abuse include patterns of repeated criticism or ridicule, threatening behavior, destroying belongings, unreasonable jealousy, and overly domineering behavior),” and “Within the last 12 months, have you been hit, slapped, kicked, or otherwise physically hurt by an adult?” (McFarlane et al., 1992).
The study was approved by 12 human subjects committees, all of which have their own federal wide assurance certificates. The primary institutional review board was the University of Wisconsin Health Sciences Human Subjects Committee. All members of the research team completed National Institutes of Health–required courses on human subjects’ protection. All participants provided written, informed consent.
Statistical analysis
Analysis of the data was performed using SPSS for Windows Version 15 statistical package (SPSS Inc., Chicago, IL). Descriptive analyses were performed on the sample. Multivariate logistic regression was used to determine the characteristics associated with risky drinking in the postpartum period. All variables in the model were generated before estimation. The variables were chosen based on existing literature. The results are presented as adjusted odds ratios (ORs).
Results
Table 1 describes the women in our sample. Approximately 87% of women identified themselves as white, 3.7% as black, 5.5% as multiracial/ethnic, and 3.9% as other (changed the order to match the order in table 1). The sample was equally split between married and unmarried women. More than 65% of the sample had attended at least some college, and more than half reported breast-feeding in the past 7 days. Thirty-five percent of the women were smokers at the time of the postpartum visit.
Table 1.
Characteristics of the sample, characterized by alcohol consumption patterns
| Total (N = 381) | Low risk (n = 237) | At risk (n = 144) | ||||
|---|---|---|---|---|---|---|
| Variable | n | % | n | % | n | % |
| Sample characteristics | ||||||
| Age, in years | (N = 381) | (n = 235) | (n = 143) | |||
| 18–25 | 161 | 42.3 | 97 | 41.3 | 64 | 44.8 |
| 26–35 | 170 | 44.6 | 110 | 46.8 | 60 | 42.0 |
| ≥36 | 47 | 12.3 | 28 | 11.9 | 19 | 13.3 |
| Missing | 3 | 0.8 | ||||
| Race/ethnicity | (N = 381) | (n = 237) | (n = 144) | |||
| White, non-Hispanic | 331 | 86.9 | 210 | 88.6 | 121 | 84.0 |
| Black, non-Hispanic | 14 | 3.7 | 7 | 3.0 | 7 | 4.9 |
| Multiracial/ethnic | 21 | 5.5 | 14 | 5.9 | 7 | 4.9 |
| Other race | 15 | 3.9 | 6 | 2.5 | 9 | 6.3 |
| Education | (N = 381) | (n = 234) | (n = 143) | |||
| No college | 124 | 32.5 | 73 | 31.2 | 51 | 35.7 |
| Some college | 253 | 66.4 | 161 | 68.8 | 92 | 64.3 |
| Missing | 4 | 1.0 | ||||
| Marital status | (N = 381) | (n = 235) | (n = 143) | |||
| Married | 190 | 49.9 | 126 | 53.6 | 64 | 44.8 |
| Not married | 188 | 49.3 | 109 | 46.4 | 79 | 55.2 |
| Missing | 3 | 0.8 | ||||
| Employment status | (N = 381) | (n = 231) | (n = 138) | |||
| Employed | 279 | 73.2 | 185 | 80.1 | 94 | 68.1 |
| Not in labor forcea | 50 | 13.1 | 28 | 12.1 | 22 | 15.9 |
| Unemployed | 40 | 10.5 | 18 | 7.8 | 22 | 15.9 |
| Missing | 12 | 3.2 | ||||
| Postpartum variables | ||||||
| No. of children | (N = 381) | (n = 233) | (n = 144) | |||
| 0–1 | 241 | 63.3 | 162 | 68.6 | 79 | 54.9 |
| ≥2 | 139 | 36.5 | 74 | 31.4 | 65 | 45.1 |
| Missing | 1 | 0.3 | ||||
| Breast-feeding in past 7 days | (N = 381) | (n = 237) | (n = 144) | |||
| No | 171 | 44.9 | 79 | 33.3 | 92 | 63.9 |
| Yes | 210 | 55.1 | 158 | 66.7 | 52 | 36.1 |
| Postpartum smoking | (N = 381) | (n = 237) | (n = 143) | |||
| No | 246 | 64.6 | 174 | 73.4 | 72 | 50.4 |
| Yes | 134 | 35.2 | 63 | 26.6 | 71 | 49.7 |
| Missing | 1 | 0.3 | ||||
| Postpartum depression | (N = 381) | (n = 320) | (n = 61) | |||
| No | 320 | 84.0 | 205 | 64.1 | 32 | 52.5 |
| Yes | 61 | 16.0 | 115 | 35.9 | 29 | 47.5 |
| Alcohol-related variables | ||||||
| Partner with risky drinking | (N = 381) | (n = 226) | (n = 140) | |||
| No | 148 | 39.8 | 109 | 49.2 | 39 | 24.9 |
| Yes | 218 | 54.2 | 117 | 51.8 | 101 | 72.1 |
| Missing | 15 | 3.9 | ||||
| Relative with history of substance problem | (N = 381) | (n = 237) | (n = 144) | |||
| No | 124 | 32.5 | 76 | 32.1 | 48 | 33.3 |
| Yes | 257 | 67.5 | 161 | 64.9 | 96 | 65.7 |
| Alcohol use during pregnancy | (N = 381) | (n = 237) | (n = 143) | |||
| No | 334 | 87.7 | 223 | 94.1 | 111 | 77.6 |
| Yes | 46 | 12.1 | 14 | 5.9 | 32 | 22.4 |
| Missing | 1 | 0.3 | ||||
| Alcohol counseling from MD/RN in past year | (N = 381) | (n = 237) | (n = 144) | |||
| No | 258 | 67.7 | 154 | 65.0 | 104 | 72.2 |
| Yes | 123 | 32.3 | 83 | 35.0 | 40 | 27.8 |
| Emotional or physical violence | (N = 381) | (n = 237) | (n = 144) | |||
| No | 278 | 73.0 | 178 | 75.1 | 100 | 69.4 |
| Yes | 103 | 27.0 | 59 | 24.9 | 44 | 30.6 |
Notes: Low risk refers to consuming fewer than seven drinks per week and not consuming four or more drinks on two or more occasions in the past 30 days. At risk refers to consuming seven or more drinks per week or consuming four or more drinks on two or more occasions in the past 30 days. MD/RN = medical doctor/registered nurse.
Such as stay at home parents, seasonal workers, or students.
Alcohol characteristics
Twelve percent of the women answered “yes” to “Did you drink any alcohol once you found out you were pregnant?” as asked on the screening survey. This percentage is in sharp contrast to the 87% (n = 333) of women who responded “yes” to “Did you drink any alcohol during the first 3 months of your most recent pregnancy? (Please include drinks you consumed before you knew you were pregnant.)” as asked in the context of the face-to-face interview. This difference indicates that most women stopped drinking once they realized that they were pregnant. Figure 1 presents the change in weekly alcohol consumption across time, with Time 1 corresponding to 6 months before pregnancy, Time 2 corresponding to the time during pregnancy and following the recognition of pregnancy, and Time 3 corresponding to the time of the postpartum interview.
Figure 1.
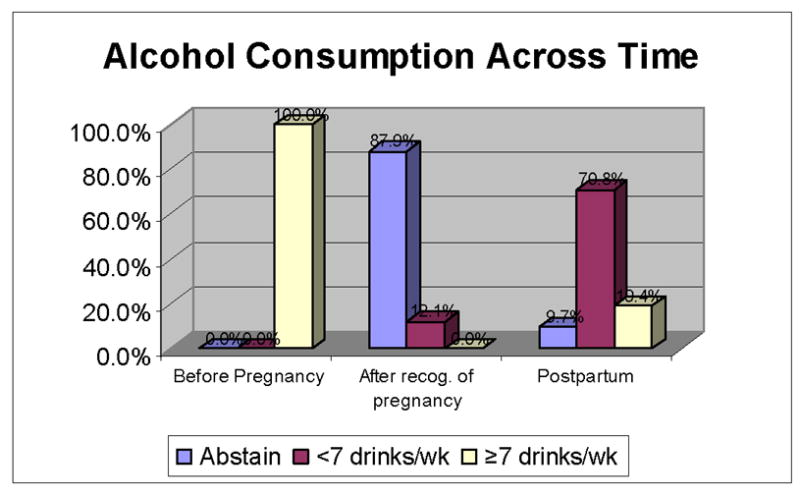
Alcohol consumption across time. Recog. = recognition; wk = week.
Based on the face-to-face interview, 52% of the sample reported at least one episode of heavy episodic drinking (four or more drinks per day) during their pregnancy. Overall, 22% of the sample reported a single incident of heavy episodic drinking, and 17% reported five or more such incidents.
Based on data from the Timeline Followback procedure, 37.8% (n = 144) of the subjects met criteria for postpartum risky drinking. Eighteen percent reported heavy episodic drinking only (consumption of four or more drinks per day at least twice in the past 28 days); 5% reported frequent drinking only (consumption of seven or more drinks per week on average); and 15% met criteria for both heavy episodic drinking and frequent drinking. Thirty-two percent of the sample reported that their physician or nurse had discussed alcohol use with them in the past 12 months.
Correlates of postpartum risky drinking
Multivariate logistic regression was used to identify characteristics correlated with risky drinking in the postpartum period. Forty women were excluded because of incomplete data, leaving 341 subjects in the final regression analysis. The model included 14 variables, which are described in the Method section. Results, in the form of adjusted ORs, are shown in Table 2. Postpartum risky drinkers were more likely than other women to have had a partner engaged in risky drinking in the past month (OR = 2.6, 95% confidence interval [CI]: 1.5–4.5); been unemployed (OR = 3.0, 95% CI: 1.2–7.7); smoked following pregnancy (OR = 1.9, 95% CI: 1.0–3.5); and consumed alcohol after the recognition of pregnancy (OR = 4.8, 95% CI: 2.2–10.6). Women who breastfed were less likely to report risky drinking (OR = 0.3, 95% CI: 0.2–0.5). The adjusted OR for receipt of counseling by a doctor or nurse was 0.6 (95% CI: 0.3–1.1, p = .07).
Table 2.
Correlates of at-risk drinking presented as adjusted odds ratios (ORs) using logistic regression
| Variable | Adjusted OR (95% CI) | p |
|---|---|---|
| Sample characteristics | ||
| Age, in years | ||
| 26–35 | Referent | |
| 18–25 | 0.9 (0.4–1.7) | NS |
| ≥36 | 1.0 (0.4–2.3) | NS |
| Race/ethnicity | ||
| White, non-Hispanic | Referent | |
| Black, non-Hispanic | 1.3 (0.3–6.0) | NS |
| Other race | 2.3 (0.7–7.7) | NS |
| Multiracial/multiethnic | 0.9 (0.3–3.0) | NS |
| Education | ||
| No college | Referent | |
| Some college | 1.6 (0.8–3.0) | NS |
| Marital status | ||
| Married | Referent | |
| Not married | 1.4 (0.7–2.8) | NS |
| Employment status | ||
| Employed | Referent | |
| Not in labor force | 1.2 (0.6–2.6) | NS |
| Unemployed | 3.0 (1.2–7.7) | <.05 |
| Postpartum variables | ||
| No. of children | ||
| 0–1 | Referent | |
| ≥2 | 1.4 (0.8–2.5) | NS |
| Breast-feeding in past 7 days | ||
| No | Referent | |
| Yes | 0.3 (0.2–0.5) | <.01 |
| Postpartum smoking | ||
| No smoking | Referent | |
| Smoking | 1.9 (1.0–3.5) | <.05 |
| Postpartum depression | ||
| EPDS ≤ 12 | Referent | |
| EPDS > 12 | 1.1 (0.5–2.5) | NS |
| Alcohol-related variables | ||
| Partner with risky drinking | ||
| No | Referent | |
| Yes | 2.6 (1.5–4.5) | <.01 |
| Relative with history of substance problems | ||
| No | Referent | |
| Yes | 0.9 (0.5–1.5) | NS |
| Alcohol use during pregnancy | ||
| No | Referent | |
| Yes | 4.8 (2.2–10.6) | <.01 |
| Alcohol counseling from MD/RN past year | ||
| No counseling | Referent | |
| Counseling | 0.6 (0.3–1.1) | NS |
| Emotional or physical violence | ||
| No | Referent | |
| Yes | 1.0 (0.5–1.9) | NS |
Notes: EPDS = Edinburgh Postnatal Depression Scale; MD/RN = medical doctor/registered nurse.
Discussion
It is concerning that 40% of women who were frequent drinkers before pregnancy were engaged in risky drinking at 3 months postpartum.. The positive association between postpartum smoking and risky drinking is not surprising, given the known association between these two behaviors during pregnancy (Flynn et al., 2003.) Although partner drinking has been identified as a risk factor for maternal drinking during pregnancy (Wiemann and Berenson, 1998), a recent study of pregnant women who screened positive on the T-ACE (Sokol et al., 1989) did not find an association between maternal prenatal alcohol consumption and a partner’s alcohol use (Chang et al., 2006). Further research is needed to clarify the role that partner drinking plays in women’s drinking patterns before, during, and after pregnancy.
Women who breast-fed their infant were less likely to be engaged in risky drinking. This finding is consistent with a previous study that found that women who breast-fed were less likely to report heavy episodic drinking (Little et al., 1990). Possible explanations for this finding are that women who engage in risky drinking may choose not to breast-feed to avoid the potential transmission of alcohol to their child, or women drinkers may be less likely to breast-feed their child because of a potential effect of alcohol on lactation. Additionally, other variables, such as those related to social support or health literacy, may affect infant-feeding practices among women drinkers.
We saw a trend for women who had received alcohol counseling by a doctor or nurse to be less likely to report postpartum risky drinking. After adjusting for other factors, however, this trend failed to reach statistical significance. We are concerned that, among this group of previously frequent drinkers, 68% did not recall having a discussion about alcohol use with a physician or nurse.
This study has several strengths. The sample was obtained from women presenting for a postpartum visit. Thus the results are applicable to obstetrical practices with patients similar to those in our study. The data on postpartum alcohol use were collected using the Timeline Followback technique, which has been validated for use across several populations (Sobell et al., 1988). Finally, we were able to control for a number of sociodemographic and behavioral variables in the analysis.
The study also has limitations. Data regarding drinking before and during pregnancy were collected during the postpartum period, leaving this information prone to recall bias. Also, partner drinking was indirectly assessed by asking the subject rather than her partner. We acknowledge the difficulty of obtaining truthful responses to questions about personal abuse. We used a number of methods to minimize underreporting, including conducting the interview in a confidential manner and instructing the research staff to reassure subjects that the information collected was solely for research purposes. A federal certificate of confidentiality also was obtained to minimize the discoverability of the information.
Although many risky drinkers reduced their alcohol consumption during pregnancy, nearly 40% of the subjects in our study reported risky patterns of drinking at 3 months postpartum. As a result, if medical providers limit their discussion of alcohol use to the first prenatal visit, opportunities for screening and intervention at other visits may be missed. Medical professionals should be aware that, although many frequent drinkers decrease their alcohol consumption during pregnancy, nearly 4 of 10 such women will once again report risky drinking in the postpartum period. Although our study focused on women with a history of frequent drinking, health care providers will not have access to this prenatal alcohol information unless alcohol screening is conducted in their offices. Validated, brief instruments such as the TWEAK (Chan et al., 1993) and the T-ACE (Sokol et al., 1989) exist to assist busy providers with the important task of screening women for problem drinking.
The evidence supporting brief intervention as an effective method for changing women’s drinking patterns continues to grow. A recent study of brief motivational intervention among women at risk for alcohol-exposed pregnancy demonstrated a twofold reduction in the risk of alcohol-exposed pregnancy among the intervention group (Floyd et al., 2007). Although this study used trained counselors in diverse settings, the delivery of brief intervention is feasible and cost-effective when done in the offices of primary care physicians (Fleming et al., 2000).
Finding the time and resources to implement alcohol screening for all women of reproductive age in health care settings is an important health care challenge. It is one of a limited number of public health interventions that can reduce the frequency of fetal alcohol exposure. Fetal alcohol spectrum disorder remains one of the most common neurologic disorders affecting children throughout the world.
This article suggests that among former frequent drinkers, some women are at higher risk for postpartum drinking than others. In the presence of limited resources and multiple competing prevention topics (e.g., tobacco use, postpartum depression, postpartum interpersonal violence, parenting issues, child-care issues, childhood-injury prevention) obstetricians and nurses who care for postpartum women may want to focus alcohol screening efforts on high-risk women. The factors noted in this report provide a profile of the women at greatest risk.
Footnotes
This research was supported by National Institute on Alcohol Abuse and Alcoholism grants R01 AA12522 and T32 AA014845.
References
- Centers for Disease Control and Prevention. Alcohol consumption among women who are pregnant or who might become pregnant—United States, 2002. MMWR. 2004;53(50):1178–1181. [PubMed] [Google Scholar]
- Chan AW, Pristach EA, Welte JW, Russell M. Use of the TWEAK test in screening for alcoholism/heavy drinking in three populations. Alcsm Clin Exp Res. 1993;17:1188–1192. doi: 10.1111/j.1530-0277.1993.tb05226.x. [DOI] [PubMed] [Google Scholar]
- Chang G, McNamara TK, Orav EJ, Wilkins-Haug L. Alcohol use by pregnant women: Partners, knowledge, and other predictors. J Stud Alcohol. 2006;67:245–251. doi: 10.15288/jsa.2006.67.245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Brit J Psychiat. 1987;150:782–786. doi: 10.1192/bjp.150.6.782. [DOI] [PubMed] [Google Scholar]
- Fleming MF, Barry KL. A three-sample test of a masked alcohol screening questionnaire. Alcohol Alcsm. 1991;26:81–91. [PubMed] [Google Scholar]
- Fleming MF, Manwell LB, Barry KL, Johnson K. At-risk drinking in an HMO primary care sample: Prevalence and health policy implications. Amer J Publ Hlth. 1998;88:90–93. doi: 10.2105/ajph.88.1.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleming MF, Mundt MP, French MT, Manwell LB, Stauffacher EA, Barry KL. Benefit-cost analysis of brief physician advice with problem drinkers in primary care settings. Med Care. 2000;38:7–18. doi: 10.1097/00005650-200001000-00003. [DOI] [PubMed] [Google Scholar]
- Floyd RL, Decoufle P, Hungerford DW. Alcohol use prior to pregnancy recognition. Amer J Prev Med. 1999;17:101–107. doi: 10.1016/s0749-3797(99)00059-8. [DOI] [PubMed] [Google Scholar]
- Floyd RL, Sobell M, Velasquez MM, Ingersoll K, Nettleman M, Sobell L, Mullen PD, Ceperich S, von Sternberg K, Bolton B, Skarpness B, Nagaraja J the Project CHOICES Efficacy Study Group. Preventing alcohol-exposed pregnancies: A randomized controlled trial. Amer J Prev Med. 2007;32:1–10. doi: 10.1016/j.amepre.2006.08.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn HA, Marcus SM, Barry KL, Blow FC. Rates and correlates of alcohol use among pregnant women in obstetrics clinics. Alcsm Clin Exp Res. 2003;27:81–87. doi: 10.1097/01.ALC.0000046595.47491.37. [DOI] [PubMed] [Google Scholar]
- Fried PA, Barnes MV, Drake ER. Soft drug use after pregnancy compared to use before and during pregnancy. Amer J Obstet Gynecol. 1985;151:787–792. doi: 10.1016/0002-9378(85)90520-4. [DOI] [PubMed] [Google Scholar]
- Gilchrist LD, Hussey JM, Gillmore MR, Lohr MJ, Morrison DM. Drug use among adolescent mothers: Prepregnancy to 18 months postpartum. J Adolesc Hlth. 1996;19:337–344. doi: 10.1016/S1054-139X(96)00052-3. [DOI] [PubMed] [Google Scholar]
- Jester JM, Jacobson SW, Sokol RJ, Tuttle BS, Jacobson JL. The influence of maternal drinking and drug use on the quality of the home environment of school-aged children. Alcsm Clin Exp Res. 2000;24:1187–1197. [PubMed] [Google Scholar]
- Little RE, Lambert MD, Worthington-Roberts B. Drinking and smoking at 3 months postpartum by lactation history. Paediat Perinat Epidemiol. 1990;4:290–302. doi: 10.1111/j.1365-3016.1990.tb00653.x. [DOI] [PubMed] [Google Scholar]
- McFarlane J, Parker B, Soeken K, Bullock L. Assessing for abuse during pregnancy: Severity and frequency of injuries and associated entry into prenatal care. JAMA. 1992;267:3176–3178. doi: 10.1001/jama.267.23.3176. [DOI] [PubMed] [Google Scholar]
- May PA, Gossage JP. Estimating the prevalence of fetal alcohol syndrome: A summary. Alcohol Res Hlth. 2001;25:159–167. [PMC free article] [PubMed] [Google Scholar]
- May PA, Gossage JP, White-Country M, Goodhart K, Decoteau S, Trujillo PM, Kalberg WO, Viljoen DL, Hoyme HE. Alcohol consumption and other maternal risk factors for fetal alcohol syndrome among three distinct samples of women before, during, and after pregnancy: The risk is relative. Amer J Med Genet Part C Seminars Med Genet. 2004;127:10–20. doi: 10.1002/ajmg.c.30011. [DOI] [PubMed] [Google Scholar]
- Miller BA, Smyth NJ, Mudar PJ. Mothers’ alcohol and other drug problems and their punitiveness toward their children. J Stud Alcohol. 1999;60:632–642. doi: 10.15288/jsa.1999.60.632. [DOI] [PubMed] [Google Scholar]
- Office of Surgeon General. Surgeon General Releases Advisory on Alcohol Use in Pregnancy (Press Release) Bethesda, MD: Department of Health and Human Services; February 21, 2005. [Google Scholar]
- Sobell LC, Sobell MB, Leo GI, Cancilla A. Reliability of a timeline method: Assessing normal drinkers’ reports of recent drinking and a comparative evaluation across several populations. Brit J Addict. 1988;83:393–402. doi: 10.1111/j.1360-0443.1988.tb00485.x. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB. Timeline follow-back: a technique for assessing self-reported alcohol consumption. In: Litten R, Allen J, editors. Measuring Alcohol Consumption. Totowa, NJ: Human Press; 1992. pp. 41–72. [Google Scholar]
- Sokol RJ, Martier SS, Ager JW. The T-ACE questions: Practical prenatal detection of risk-drinking. Amer J Obstet Gynecol. 1989;160:863–868. doi: 10.1016/0002-9378(89)90302-5. discussion 868–870. [DOI] [PubMed] [Google Scholar]
- Tough S, Tofflemire K, Clarke M, Newburn-Cook C. Do women change their drinking behaviors while trying to conceive? An opportunity for preconception counseling. Clin Med Res. 2006;4:97–105. doi: 10.3121/cmr.4.2.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace P, Haines A. Use of a questionnaire in general practice to increase the recognition of patients with excessive alcohol consumption. Brit Med J Clin Res Ed. 1985;290:1949–1953. doi: 10.1136/bmj.290.6486.1949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitaker RC, Orzol SM, Kahn RS. Maternal mental health, substance use, and domestic violence in the year after delivery and subsequent behavior problems in children at age 3 years. Arch Gen Psychiat. 2006;63:551–560. doi: 10.1001/archpsyc.63.5.551. [DOI] [PubMed] [Google Scholar]
- Wiemann CM, Berenson AB. Factors associated with recent and discontinued alcohol use by pregnant adolescents. J Adolesc Hlth. 1998;22:417–423. doi: 10.1016/s1054-139x(97)00215-2. [DOI] [PubMed] [Google Scholar]