

A primiparous mother had an antenatal ultrasound at 21 weeks' gestation, which showed a mass in the left side of the brain arising from the intraventricular region and several cardiac tumours, most likely to be rhabdomyomas. An MRI scan at 24 weeks' gestation showed an intraventricular mass in the fronto‐parietal part of the left cerebral hemisphere of the fetus (fig 1). The lesion was of high signal on T1 weighted sequence and low on T2. The boy was born at 36 weeks' gestation. Physical and neurological examination was normal. Postnatal cranial ultrasound and MRI confirmed a large mass lesion involving the left lateral ventricle; within the body of the right ventricle was a solitary subependymal nodule (fig 2). Based on the radiological abnormalities of the brain and heart, tuberous sclerosis (TS) was strongly suspected. The tumour in the left hemisphere fulfilled the neuroradiological diagnostic criteria for a subependymal giant cell astrocytoma (SEGA).1 There was no history or evidence of TS on clinical examination of family members. Genetic testing of the neonate showed the mutation for TS.
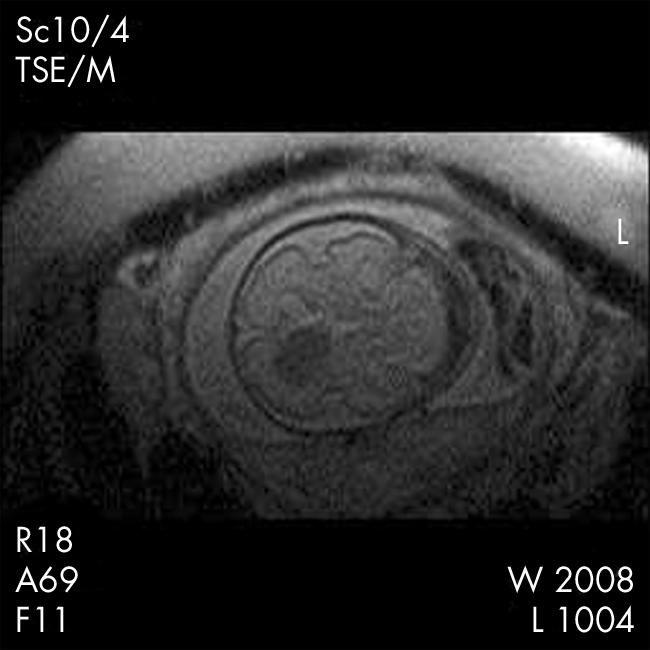
Figure 1 Fetal MRI scan. Axial T2 weighted image at 24 weeks, showing a low signal mass in the body of the left lateral ventricle.
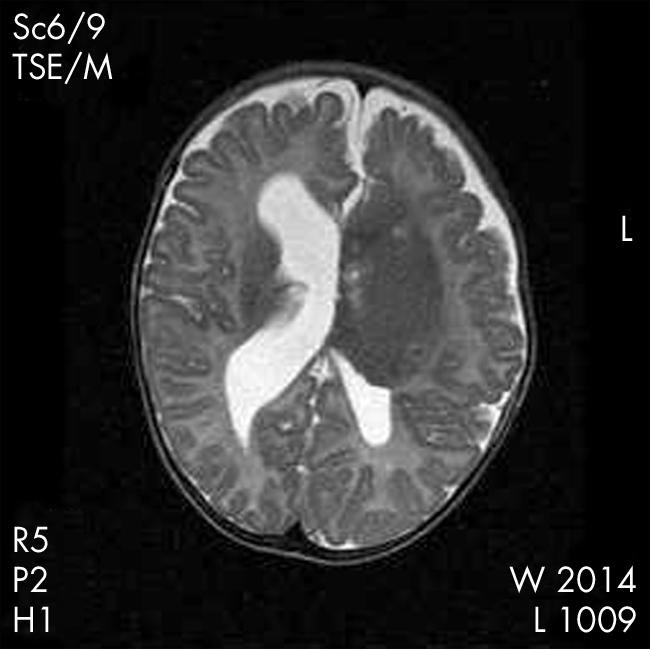
Figure 2 Postnatal MRI scan. Axial T2 weighted sequence, showing large mass lesion involving the body and frontal horn of the left lateral ventricle. Within the body of the right ventricle was a solitary subependymal nodule.
At 2 months he developed right focal seizures and anticonvulsant therapy was commenced. EEG showed hypsarrhythmia. At 10 months of age he underwent surgical excision of the brain tumour, confirmed histologically as a SEGA. Now aged 1 year, his development is within normal limits and his seizures are controlled.
SEGAs are rare brain tumours that occur typically in the walls of the lateral ventricles and are generally located near the foramen of Monro. They are nearly always associated with TS.2,3 They are usually discovered in the second decade of life and only rarely occur in infancy.4 To our knowledge this the first report of a SEGA diagnosed on fetal MRI. Although they are benign in nature and grow slowly, they represent a major cause of death due to raised intracranial pressure or haemorrhage in patients with TS.5
Footnotes
Competing interests: none
References
- 1.Griffiths P D, Martland T R. Tuberous sclerosis complex: the role of neuroradiology. Neuropediatrics 199728244–252. [DOI] [PubMed] [Google Scholar]
- 2.Haslam R H A. Tuberous sclerosis. In: Buyse ML, ed. Birth defects encyclopedia. Cambridge, MA: Blackwell, 19901712–1714.
- 3.Reznik M, Pierard G E. Neurophakomatoses and allied disorders. In: Duckett S, ed. Pediatric neuropathology. Malvern, PA: Williams & Wilkins, 1995740–743.
- 4.Shepherd C W, Scheithauer B, Gomez M R. Brain tumors in tuberous sclerosis: a clinicopathologic study of the mayo clinic experience. Mayo Clin Proc 199166378–379. [DOI] [PubMed] [Google Scholar]
- 5.Gomez M R. The phakomatoses. In: Gomez MR, ed. Tuberous sclerosis. New York: Raven Press, 199816–20.