

Abstract
Meniscal injuries place the knee at risk for early osteoarthritis (OA) because they disrupt their load-bearing capabilities. Partial resection is routinely performed to alleviate symptomatic meniscal tears. While the removal of meniscal tissue may not be the only factor associated with partial meniscectomy outcome, the amount removed certainly contributes to functional loss. It is unknown, however, whether there is a critical amount of meniscal tissue that can be removed without diminishing the structure’s chondroprotective role. In order to examine the existence of such a threshold, it is necessary to accurately quantify meniscal volume both before and after partial meniscectomy to determine the amount of meniscal tissue removed. Therefore, our goal was to develop and validate an MR-based method for assessing meniscal volume. The specific aims were: (1) to evaluate the feasibility of the MR-based segmentation method; (2) to determine the method’s reliability for repeated measurements; and (3) to validate its accuracy in situ. MR images were obtained on a 3T magnet, and each scan was segmented using a biplanar approach. The MR-based volumes for each specimen were compared to those measured by water displacement. The results indicate that the biplanar approach of measuring meniscal volumes is accurate and reliable. The calculated volumes of the menisci were within 5% of the true values, the coefficients of variation were 4%, and the intraclass correlation coefficients were greater than 0.96. These data demonstrate that this method could be used to measure the amount of meniscal tissue excised during partial meniscectomy to within 125.7mm3.
Keywords: Knee, Meniscus, Meniscectomy, Biomechanics, MRI
1. Introduction
The menisci of the knee are crescent-shaped fibrocartilagenous washers that protect articular cartilage by maximizing contact area and minimizing contact stress within the tibiofemoral joint. When a meniscus is torn, the contact mechanics of the tibiofemoral joint are altered, which disrupts the homeostasis of articular cartilage metabolism, placing the knee at risk for early osteoarthritis (OA). Biomechanical studies have clearly shown that joint contact mechanics are altered following meniscectomy and meniscal transplantation (Haut Donahue, et al., 2002; Donahue, et al., 2003; Haut Donahue, et al., 2004; Huang, et al., 2002; Huang, et al., 2003; Wilson, et al., 2003; Fairbank, 1948).
Total meniscectomy was once the standard treatment for symptomatic meniscal tears. This procedure decreases tibiofemoral contact area by 50–70%, a change which significantly increases contact stress on the articular cartilage (Ahmed and Burke, 1983) and reduces its shock-absorbing capabilities (Voloshin and Wosk, 1985). The link between meniscectomy and OA has been well-documented (Englund and Lohmander, 2004; McNicholas, et al., 2000; Roos, H., et al., 1998). Thus, partial resection, in which the undamaged portion of the meniscus is preserved, is now routinely performed to eliminate symptoms while attempting to preserve cartilage integrity (Andersson-Molina, et al., 2002; Chatain, et al., 2001; Englund, et al., 2001; Englund, et al., 2003; Englund and Lohmander, 2004). However, partial meniscectomy may not eliminate the risk of early OA (Andersson and Gillquist, 1990; Andersson-Molina, et al., 2002; Chatain, et al., 2001; Chatain, et al., 2003; Cicuttini, et al., 2002; Englund, et al., 2001; Englund, et al., 2003; Higuchi, et al., 2000; Hoser, et al., 2001; Hulet, et al., 2001; Rangger, et al., 1995; Rockborn and Messner, 2000; Roos, H., et al., 1995; Roos, E.M., et al., 2001; Roos, H., et al., 1998).
To date, no clinical studies have objectively measured the amount of meniscus that can be removed following acute meniscal injury without placing the knee at risk of OA. In order to examine whether a critical threshold exists, it is necessary to quantify the amount of meniscal tissue removed during surgery. Quantitative magnetic resonance imaging (MRI) has been used to assess dimensional changes of articular cartilage (Eckstein and Glaser, 2004), and could be used to construct models of the meniscus before and after partial meniscectomy; the difference between the two volumes would indicate the amount of tissue removed.
This study’s objective was to validate an MR-based approach to document meniscal size and assess changes in meniscal volume following surgery. The specific aims were: (1) to evaluate the method’s feasibility (phantom model); (2) to determine the technique’s reliability (cadaver model); and (3) to validate the technique’s accuracy in situ (cadaver model).
2. Methods
2.1 MR imaging
Specimens were imaged on a 3T scanner (Siemens Trio, Erlangen, Germany) using a surface coil. The T2*-weighted 3D-CISS sequence [constructive interference in the steady state; TR/TE/FA, 14.5/7.3/35°; FOV, 160mm; matrix, 512x512, slice length/gap, 1mm/0; avg, 1] was utilized. Preliminary testing determined that this sequence provided high contrast between meniscal tissue and adjacent structures.
2.2 Segmentation technique
The phantom model and cadaver menisci were manually segmented from both sagittal and coronal plane image reconstructions using commercial software (Mimics 9.11; Materialise, Ann Arbor, MI). Three-dimensional voxel models were generated from the biplanar segmentations and wrapped with a triangular mesh to create a solid model of each structure. The solid models captured both meniscal volume and morphology (Figure 1). Each model’s volume was calculated by surface integration.
Figure 1.
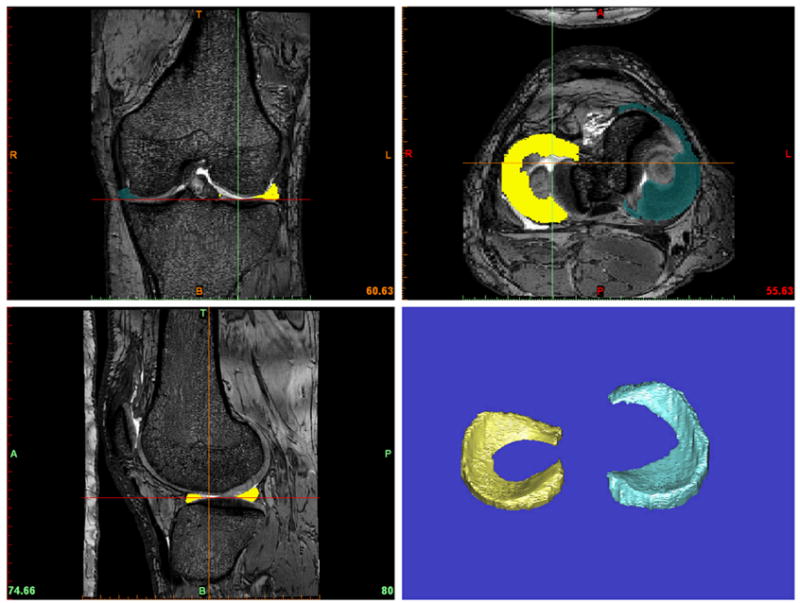
The user interface of the commercial segmentation software (Mimics 9.11; Materialise, Ann Arbor, MI) used for this study. The top panes show coronal (left) and axial (right) views; the bottom panes show the sagittal view (left) and 3-D meniscal reconstructions (right).
2.3 Water volume technique
The volume of each MR-based model was compared to its water displacement volume (Stone, et al., 1994). After imaging, the menisci were carefully dissected from the joint. Each meniscus was placed in a 25cc graduated cylinder containing 25cc of isotonic saline. The displaced saline was removed from the cylinder, using a micropipette, until the fluid level was restored to 25cc. Each water volume measurement was repeated three times, and the values averaged. Previous testing determined that the coefficient of variation for repeated water displacement measurements was 1.5%.
2.4 Feasibility study (Aim 1)
The feasibility of the segmentation method was evaluated using a plastic phantom model. A single intact fresh human cadaver knee with no evidence of knee pathology was imaged as described above. The menisci were segmented using MR-based biplanar segmentation, and 3-D models of the menisci were generated. Using rapid prototyping technology, plastic prototypes of these menisci were created. The volumes of the model menisci (medial = 4352.67mm3; lateral = 3741.38mm3) were confirmed by water displacement. The plastic models were then embedded within 1.7% agarose gel. The gel was created within a plastic cylinder (diameter 11cm, height 10cm) similar in size to a human knee cross-section. The phantom was imaged as described, and the plastic produced a contrast similar to that seen between menisci and surrounding tissues. The plastic menisci were segmented, and the MR-based volumes were compared with the known model volumes to establish a percent error in volume.
2.5 Reliability study (Aim 2)
The reliability of the MR-based segmentation method for multiple scans was evaluated using a fresh human cadaver knee. The knee was scanned 7 times; the specimen was removed and repositioned within the coil between scans. After imaging, the cadaver menisci were carefully excised, and their water displacement volumes were measured. After the menisci were segmented and reconstructed, the MR-based volumes were compared to the water displacement volumes. The coefficients of variation for both the medial and lateral menisci were calculated.
2.6 In situ validation (Aim 3)
The MR-based segmentation method was then validated in situ. 10 fresh-frozen human cadaver knees (5 pairs; mean age=56; range=52–60) with no gross evidence of knee pathology were imaged, after which one knee from each pair underwent a partial medial meniscectomy. Partial meniscectomies were performed within the inner rim of the medial meniscus. Resection size was not standardized between specimens. All knees were then rescanned. The “pre-operative” and “post-operative” MR images of each knee were segmented, and the volumes of the medial and lateral menisci were calculated. The MR-based volume of meniscal tissue removed during each resection was determined by subtracting the post-operative volume from the pre-operative volume. This value was compared to the water displacement volume of the portion of meniscus removed. The post-operative scans of the medial meniscus of the contralateral knee and the lateral menisci from both knees served as “repeated standards” to assess reliability. Because these menisci did not undergo meniscectomy, no volume changes were expected between scans. Both menisci were then removed from all 10 knees, and their water displacement volumes were determined. Reliability was quantified by calculating intraclass correlation coefficients (ICCs) for the repeated standards. Accuracy was assessed by calculating the absolute error between the MR-based volume and water displacement volume for each meniscus. Variation between right and left medial and lateral meniscal volumes was examined for these five pairs of cadaver specimens (Figure 2).
Figure 2.

Mean (+1 standard deviation) MR-based and water displacement volumes for right and left medial and lateral menisci of specimens used in Aim 3. Water volumes of medial and lateral menisci for each pair of knees showed mean coefficients of variation (CV) of 5.78% and 4.95%, respectively. MR-based volumes of medial and lateral menisci for each pair showed mean CVs of 6.45% and 4.32%, respectively. Mean MR-based volumes of the medial menisci of the right and left knees were 3102mm3 and 2969mm3, respectively. Mean MR-based volumes of the lateral menisci of the right and left knees were 2913mm3 and 2859mm3, respectively.
3. Results
3.1 Feasibility study (Aim 1)
When compared to the known volumes, the errors for the plastic medial and lateral menisci were 0.3% and 3.3%, respectively. The phantom MR-based volumes overestimated the intact model volumes for the medial and lateral menisci at 4363.8mm3 (versus 4352. 7mm3) and 3863.1mm3 (versus 3741.4mm3), respectively.
3.2 Reliability study (Aim 2)
The mean absolute errors between MR-based and water displacement volumes of the medial and lateral menisci were 4.6% and 7.9%, respectively (Table 1). The coefficients of variation were 4% for both compartments.
Table 1.
The mean absolute errors between MR-based and water displacement volumes of the medial and lateral menisci
Mean (± 1 standard deviation) MR-based and water displacement volumes of one cadaver knee scanned 7 times (Aim 2). Water volume measurements were repeated 3 times.
| Meniscus | Water Vol. Mean (mm3; n=3) | MR-Based Mean (mm3; n=7) | %Error |
|---|---|---|---|
| Medial | 3041 (±43) | 2927 (±118) | 4.6 |
| Lateral | 3067 (±71) | 2801 (±112) | 7.9 |
3.3 In situ Validation (Aim 3)
The ICCs for repeated standards were greater than 0.96, indicating that the technique was reliable. The mean absolute errors between MR-based and water displacement volumes across all specimens were less than 5.3% (Figure 3). The average volumes of the resected pieces were 522 (range 330–880) mm3 and 565 (range 325–1000) mm3 for the MR-based segmentation and water displacement methods, respectively (Figure 3). Excluding the volumes of the resected pieces, the mean absolute errors between MR-based volumes and water displacement volumes were 4.8% and 3.0% for the medial and lateral menisci, respectively (Figure 2). The 95% confidence interval of the difference between the calculated (MR) and actual (water displacement) volumes of the removed fragments was 125.7mm3.
Figure 3.

Mean (+1 standard deviation) meniscal volumes for surgical and contralateral control knees using MR-based segmentation and water displacement. 565mm3 (range 325–1000mm3; water displacement-based) were removed from the medial meniscus of the surgical* knee. The mean surgical* pre-op water volume was 3020 ± 987mm3 (the sum of the post-op water volume and the volume of meniscus removed during meniscectomy). Pre-op water displacement volume equaled post-op water volume for medial control and all lateral menisci.
4. Discussion
The amount of meniscus that can be removed following an acute meniscal injury without placing the knee at risk of OA is unknown. In order to examine whether there is a critical threshold, it is necessary to quantify the amount of meniscal tissue removed during surgery. Such a method could be used to design a clinical study of partial meniscectomy for simple acute tears, in which each patient’s partial meniscectomy and residual meniscal tissue could be quantified. Each patient could then be tracked, and the mechanisms of OA development following partial meniscectomy could be better understood. We have shown that this MR-based approach is accurate and reliable for tracking changes in meniscal volume. This method may also be useful for sizing meniscal allografts, because the MR-based segmentation technique results in a 3-D model in which both meniscal morphology and volume can be examined.
In developing a technique to size meniscal allografts, Stone et al utilized a similar imaging approach (Stone, et al., 1994). They used a 3-D MR sequence on a 1.5T magnet. Images were segmented in the sagittal plane, and MR measurements were performed 6 times per cadaver specimen before the menisci were excised. The volumes of the menisci were then measured by water displacement. Stone reported that the MR technique was precise but consistently underestimated true meniscal volume by 20% and 44% for medial and lateral menisci, respectively.
Our MR-based segmentation approach has several improvements. Images were obtained on a 3T magnet using the T2*-weighted, 3D-CISS sequence. The protocol provided high-resolution images and high contrast between meniscal tissue and adjacent structures. Because meniscal contours are best seen in orthogonal images, segmentations were performed using both sagittal and coronal views of the same volume to optimize the central and anterior/posterior boundaries of the menisci, respectively. The reliability study (Aim 2), in which coefficients of variation were less than 4% for both menisci, indicated that results were reproducible. The calculated volumes of the menisci for the in situ validation study were within 5% of their water displacement volumes, and the ICCs between methods were greater than 0.96. The method was accurate for detecting meniscal morphometry before and after partial meniscectomy to within 125.7mm3.
Some limitations should be noted. The evaluations were performed using phantom (Aim 1) and cadaver specimens (Aims 2 and 3). Motion and blood flow artifacts were not present; thus, a clinical evaluation of reliability is needed. The segmentations were performed manually. To minimize variation, the images were segmented by a trained examiner under a musculoskeletal radiologist’s direction. Since meniscal segmentations were performed independently, the results of the repeatability (Aim 2) and accuracy (Aim 3) studies minimize this concern. Although MRI is a reasonable means of detecting displaced meniscal fragments (Wright, et al., 1995), the accuracy of this approach for more complicated tears (i.e. bucket handle tears) remains unknown. However, based on our results (Figure 2), it would be possible to use the respective meniscus of the uninjured contralateral knee as a baseline, or check, for complex tears. Despite these limitations, the MR-based biplanar segmentation method provides an accurate and reliable way to document meniscal volumes from 3-D segmented models.
Acknowledgments
This work was funded by the National Institutes of Health (AR049199; AR047910; and AR047910S1). The authors gratefully acknowledge the technical support of Lynn Fanella and Theodore Trafton, and the statistical advice of Gary Badger (University of Vermont).
References
- Ahmed AM, Burke DL. In-vitro measurement of static pressure distribution in synovial joints - Part I: Tibial surface of the knee. Journal of Biomechanical Engineering. 1983;105:216–225. doi: 10.1115/1.3138409. [DOI] [PubMed] [Google Scholar]
- Andersson-Molina H, Karlsson H, Rockborn P. Arthroscopic partial and total meniscectomy: A long-term follow-up study with matched controls. Arthroscopy. 2002;18:183–189. doi: 10.1053/jars.2002.30435. [DOI] [PubMed] [Google Scholar]
- Andersson C, Gillquist J. Instrumented testing for evaluation of sagittal plane laxity. Clinical Orthopaedics and Related Research. 1990;256:178–184. [PubMed] [Google Scholar]
- Chatain F, Adeleine P, Chambat P, Neyret P. A comparative study of medial versus lateral arthroscopic meniscectomy on stable knees. 10-year minimum follow-up study. Arthroscopy. 2003;19:842–849. doi: 10.1016/s0749-8063(03)00735-7. [DOI] [PubMed] [Google Scholar]
- Chatain F, Robinson AHN, Adeleine P, Chambat P, Neyret P. The natural history of the knee following arthroscopic medial meniscectomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2001;9:15–18. doi: 10.1007/s001670000146. [DOI] [PubMed] [Google Scholar]
- Cicuttini FM, Forbes A, Yuanyuan W, Rush G, Stuckey SL. Rate of knee cartilage loss after partial meniscectomy. Journal of Rheumatology. 2002;29:195–1956. [PubMed] [Google Scholar]
- Donahue TLH, Hull ML, Rashid MM, Jacobs CR. How the stiffness of meniscal attachments and meniscal material properties affect tibiofemoral contact pressure computed using a validated finite element model of the human knee joint. Journal of Biomechanics. 2003;36:19–34. doi: 10.1016/s0021-9290(02)00305-6. [DOI] [PubMed] [Google Scholar]
- Eckstein F, Glaser C. Measuring cartilage morphology with quantitative magnetic resonance imaging. Seminars in Musculoskeletal Radiology. 2004;8:329–353. doi: 10.1055/s-2004-861579. [DOI] [PubMed] [Google Scholar]
- Englund M, Lohmander LS. Risk factors for symptomatic knee osteoarthritis fifteen to twenty-two years after meniscectomy. Arthritis & Rheumatism. 2004;50:2811–2819. doi: 10.1002/art.20489. [DOI] [PubMed] [Google Scholar]
- Englund M, Roos EM, Lohmander LS. Impact of type of meniscal tear on radiographic and symptomatic knee osteoarthritis: A sixteen-year followup of meniscectomy with matched controls. Arthritis & Rheumatism. 2003;48:2178–2187. doi: 10.1002/art.11088. [DOI] [PubMed] [Google Scholar]
- Englund M, Roos EM, Roos HP, Lohmander LS. Patient relevant outcomes fourteen years after meniscectomy: Influence of type of meniscal tear and size of resection. Rheumatology. 2001;40:631–639. doi: 10.1093/rheumatology/40.6.631. [DOI] [PubMed] [Google Scholar]
- Fairbank TJ. Knee joint changes after meniscectomy. Journal of Bone and Joint Surgery. British Volume. 1948;30:664–670. [PubMed] [Google Scholar]
- Haut Donahue TL, Hull ML, Rashid MM, Jacobs CR. A finite element model of the human knee joint for the study of tibio-femoral contact. Journal of Biomechanical Engineering. 2002;124:273–280. doi: 10.1115/1.1470171. [DOI] [PubMed] [Google Scholar]
- Haut Donahue TL, Hull ML, Rashid MM, Jacobs CR. The sensitivity of tibiofemoral contact pressure to the size and shape of the lateral and medial menisci. Journal of Orthopaedic Research. 2004;22:807–814. doi: 10.1016/j.orthres.2003.12.010. [DOI] [PubMed] [Google Scholar]
- Higuchi H, Kimura M, Shirakura K, Terauchi M, Takagishi K. Factors affecting long-term results after arthroscopic partial meniscectomy. Clinical Orthopaedics and Related Research. 2000;377:161–168. doi: 10.1097/00003086-200008000-00022. [DOI] [PubMed] [Google Scholar]
- Hoser C, Fink C, Brown C, Reichkendler M, Hackl W, Bartlett J. Long-term results of arthroscopic partial lateral meniscectomy in knees without associated damage. Journal of Bone and Joint Surgery British. 2001;83:513–516. doi: 10.1302/0301-620x.83b4.11364. [DOI] [PubMed] [Google Scholar]
- Huang A, Hull ML, Howell SM. The level of compressive load affects conclusions from statistical analyses to determine whether a lateral meniscal autograft restores tibial contact pressure to normal: a study in human cadaveric knees. Journal of Orthopaedic Research. 2003;21:459–464. doi: 10.1016/S0736-0266(02)00201-2. [DOI] [PubMed] [Google Scholar]
- Huang A, Hull ML, Howell SM, Donahue TH. Identification of cross-sectional parameters of lateral meniscal allografts that predict tibial contact pressure in human cadaveric knees. Journal of Biomechanical Engineering. 2002;124:481–489. doi: 10.1115/1.1503061. [DOI] [PubMed] [Google Scholar]
- Hulet CH, Locker G, Schiltz D, Texier A, Tallier E, Vielpeau CH. Arthroscopic medial meniscectomy on stale knees - A 12-year follow-up. Journal of Bone and Joint Surgery. British Volume. 2001;83:29–32. doi: 10.1302/0301-620x.83b1.11115. [DOI] [PubMed] [Google Scholar]
- McNicholas MJ, Rowley DI, McGurty D, Adalberth T, Abdon P, Lindstrand A, Lohmander LS. Total meniscectomy in adolescence: a thirty year follow-up. Journal of Bone and Joint Surgery - British Volume. 2000;82:217–221. [PubMed] [Google Scholar]
- Rangger C, Klestil T, Gloetzer W, Kemmler G, Benedetto KP. Osteoarthritis after arthroscopic partial meniscectomy. American Journal of Sports Medicine. 1995;23:240–244. doi: 10.1177/036354659502300219. [DOI] [PubMed] [Google Scholar]
- Rockborn P, Messner K. Long term results of meniscus repair and meniscectomy: a 13-year functional and radiographic follow-up study. Knee Surgery, Sports Traumatology, Arthroscopy. 2000;8:2–9. doi: 10.1007/s001670050002. [DOI] [PubMed] [Google Scholar]
- Roos EM, Ostenberg A, Roos H, Ekdahl C, Lohmander LS. Long-term outcome of meniscectomy: symptoms, function, and performance tests in patients with or without radiographic osteoarthritis compared to matched controls. Osteoarthritis and Cartilage. 2001;9:316–324. doi: 10.1053/joca.2000.0391. [DOI] [PubMed] [Google Scholar]
- Roos H, Adalberth T, Dahlberg L, Lohmander LS. Osteoarthritis of the knee after injury to the anterior cruciate ligament or meniscus: The influence of time and age. Osteoarthritis and Cartilage. 1995;3:261–267. doi: 10.1016/s1063-4584(05)80017-2. [DOI] [PubMed] [Google Scholar]
- Roos H, Lauren M, Adalberth T, Roos EM, Jonsson K, Lohmander LS. Knee osteoarthritis after meniscectomy: prevalence of radiographic changes after twenty-one years, compared with matched controls. Arthritis and Rheumatism. 1998;41:687–693. doi: 10.1002/1529-0131(199804)41:4<687::AID-ART16>3.0.CO;2-2. [DOI] [PubMed] [Google Scholar]
- Stone KR, Stoller DW, Irving SG, Elmquist C, Gildengorin G. 3D MRI volume sizing of knee meniscus cartilage. Arthroscopy. 1994;10:641–644. doi: 10.1016/s0749-8063(05)80062-3. [DOI] [PubMed] [Google Scholar]
- Voloshin AS, Wosk J. Shock absorbtion of meniscectomized and painful knees. Journal of Biomedical Engineering. 1985;5:157–161. doi: 10.1016/0141-5425(83)90036-5. [DOI] [PubMed] [Google Scholar]
- Wilson W, van Rietbergen B, van Donkelaar CC, Huiskes R. Pathways of load-induced cartilage damage causing cartilage degeneration in the knee after meniscectomy. Journal of Biomechanics. 2003;36:845–851. doi: 10.1016/s0021-9290(03)00004-6. [DOI] [PubMed] [Google Scholar]
- Wright DH, De Smet AA, Norris M. Bucket-Handle Tears of the Medial and Lateral Menisci of the Knee: Value of MR Imaging in Detecting Displaced Fragments. AJR. American Journal of Roentgenology. 1995;165:621–625. doi: 10.2214/ajr.165.3.7645481. [DOI] [PubMed] [Google Scholar]