

Abstract
A 71-year-old man presented with a 2-week history of pain and swelling of his left arm. Subsequent investigations revealed an intramuscular lesion, suggestive of soft tissue sarcoma. Histologic analysis was surprisingly consistent with metastasis from a primary squamous cell lung cancer. Skeletal muscle metastasis as a mode of presentation of primary lung cancer is an unusual phenomenon. A brief literature review accompanies this report.
Case Report
A 71-year-old man presented with a 2-week history of a hard, painful, nonpulsatile mass in his left upper arm. Examination revealed a craggy, mobile mass with irregular borders in the extensor compartment of the left arm measuring 6 × 4 cm. Ultrasonography of the left arm demonstrated the presence of deep ovoid hyperechoic mass located in the long axis of the left triceps muscle, measuring 5 × 3 cm (Figure 1). This led to further radiologic evaluation in the form of MRI of the left arm. MRI showed intermediate signal mass in the triceps musculature on T1-weighted images with fat saturation (Figure 2) This lesion is confined to the extensor compartment of the arm. A presumptive diagnosis of soft tissue sarcoma was made. An incisional biopsy was performed. This was found to be consistent with metastatic squamous cell carcinoma (Figure 3) with a possible lung primary, further supported due to a positive CK7 and negative CK20 stain on immunohistochemistry. CT scan of the chest revealed a lesion measuring 4 × 2 cm in the left upper lobe (Figure 4). Fiber-optic bronchoscopy and biopsy confirmed the diagnosis of stage IV squamous cell carcinoma of the lung. He underwent palliative radiotherapy to the mass in the arm, 20 Gy in 4 fractions. This provided good relief from pain and swelling within 2 weeks of completing treatment. Systemic therapy was not offered on the basis of poor and deteriorating performance status. Unfortunately, the patient died within 10 weeks of presentation.
Figure 1.
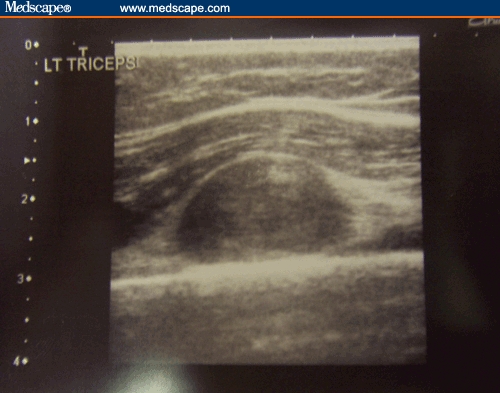
Ultrasonography demonstrating a deep ovoid hypoechoic mass within the axis of left triceps musculature, adjacent to humeral cortex posteriorly.
Figure 2.

T1-weighted MRI with fat saturation, axial images, demonstrating intermediate signal mass within the triceps muscle.
Figure 3.

Biopsy histology demonstrating squamous cell carcinoma histology. H&E stain, 400× magnification.
Figure 4.

Axial images of the thorax showing a 4 × 2 cm lesion in the left upper lobe.
Discussion
Intramuscular metastases in cancer patients are rare.[1] This in itself is quite peculiar because muscular mass accounts for approximately 50% of total body weight. It is thought that muscular contractile actions, local pH environment, and accumulation of lactic acid and other metabolites contribute to the rare occurrence of this phenomenon.[2] The true incidence of muscular metastasis remains unknown, but an autopsy series suggests that its incidence could be as low as 0.8%.[3]
Lung carcinoma seems to be the underlying primary cancer in most of these cases. Many other tumors, such as kidney, stomach, pancreas, thyroid gland, breast, ovary, prostate, and bladder cancers have also been sporadically described in association with intramuscular secondaries.[1,4–7] However, primary presentation of an intramuscular metastasis, such as demonstrated by our patient, remains an exceptionally unusual occurrence.[5]
The most frequent presentation of muscular metastasis is pain with or without swelling.[7,8] Diagnosis of this condition, even with radiologic imaging is often tricky because it can be confused with an abscess or soft tissue tumors, highlighting the value of histologic diagnosis. Treatment in the form of radiotherapy, chemotherapy, or even metastasectomy often provides palliation only. Most patients die in less than a year from diagnosis.[1,8]
This case highlights the importance of histologic diagnosis despite classic clinical and radiologic findings supportive of a particular tumor type. In addition, this case also adds further to the literature pool, suggesting a differential diagnosis of non-small-cell lung cancer in patients presenting with an intramuscular mass.
Footnotes
Readers are encouraged to respond to the author at albiruni_ryan@yahoo.co.uk or to Paul Blumenthal, MD, Deputy Editor of MedGenMed, for the editor's eyes only or for possible publication via email: pblumen@stanford.edu
Contributor Information
Albiruni Ryan Abdul Razak, Northern Centre for Cancer Treatment, Newcastle upon Tyne, United Kingdom Author's email address: albiruni_ryan@yahoo.co.uk.
Rajiv Chhabra, Northern Centre for Cancer Treatment, Newcastle upon Tyne, United Kingdom.
Andrew Hughes, Northern Centre for Cancer Treatment, Newcastle upon Tyne, United Kingdom.
Simon England, Sunderland Royal Hospital, Sunderland, United Kingdom.
Petra Dildey, Northern Centre for Cancer Treatment, Newcastle upon Tyne, United Kingdom.
Rhona McMenemin, Northern Centre for Cancer Treatment, Newcastle upon Tyne, United Kingdom.
References
- 1.McKeown PP, Conant P, Auerbach LE. Squamous cell carcinoma of the lung: An unusual metastasis to the pectoralis muscle. Ann Thorac Surg. 1996;61:1526–1528. doi: 10.1016/0003-4975(95)01177-3. [DOI] [PubMed] [Google Scholar]
- 2.Garcia OA, Fernandez EG, Buelta SL, et al. Metastasis of malignant neoplasms to skeletal muscle. Rev Esp Oncol. 1984;31:57–67. [PubMed] [Google Scholar]
- 3.Sudo A, Ogihara Y, Shiokawa Y, Fujinami S, Sekiguchi S. Intermuscular metastasis of carcinoma. Clin Orthop Relat Res. 1993;296:213–217. [PubMed] [Google Scholar]
- 4.Heyer CM, Rduch GJ, Zgoura P, et al. Metastasis to skeletal muscle from oesophageal adenocarcinoma. Scand J Gastroenterol. 2005;40:1000–1004. doi: 10.1080/00365520510023143. [DOI] [PubMed] [Google Scholar]
- 5.Belhabis D, Maalej S, Fenniche S, et al. Muscle metastasis of primary bronchial carcinoma. Tunis Med. 2001;79:557–560. [PubMed] [Google Scholar]
- 6.Menard O, Seiqneur J, Lamy P. Muscular metastasis of primary bronchial carcinoma. Rev Pneumol Clin. 1990;46:183–186. [PubMed] [Google Scholar]
- 7.Cheong TH, Wang YT, Poh SC, et al. Carcinoma of the lung with metastases to skeletal muscles. Singapore Med J. 1989;30:605–606. [PubMed] [Google Scholar]
- 8.Sridhar KS, Rao RK, Kunhardt B. Skeletal muscle metastases from lung cancer. Cancer. 1987;59:1530–1534. doi: 10.1002/1097-0142(19870415)59:8<1530::aid-cncr2820590824>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]