

Abstract
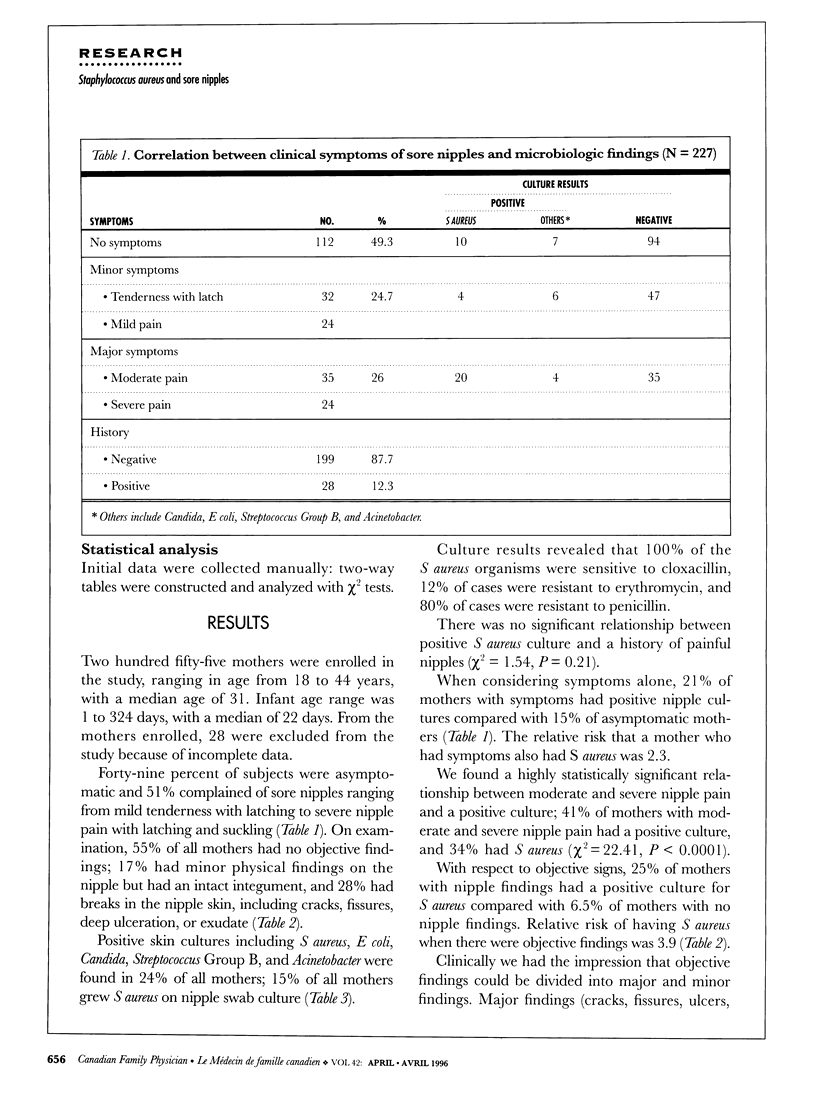
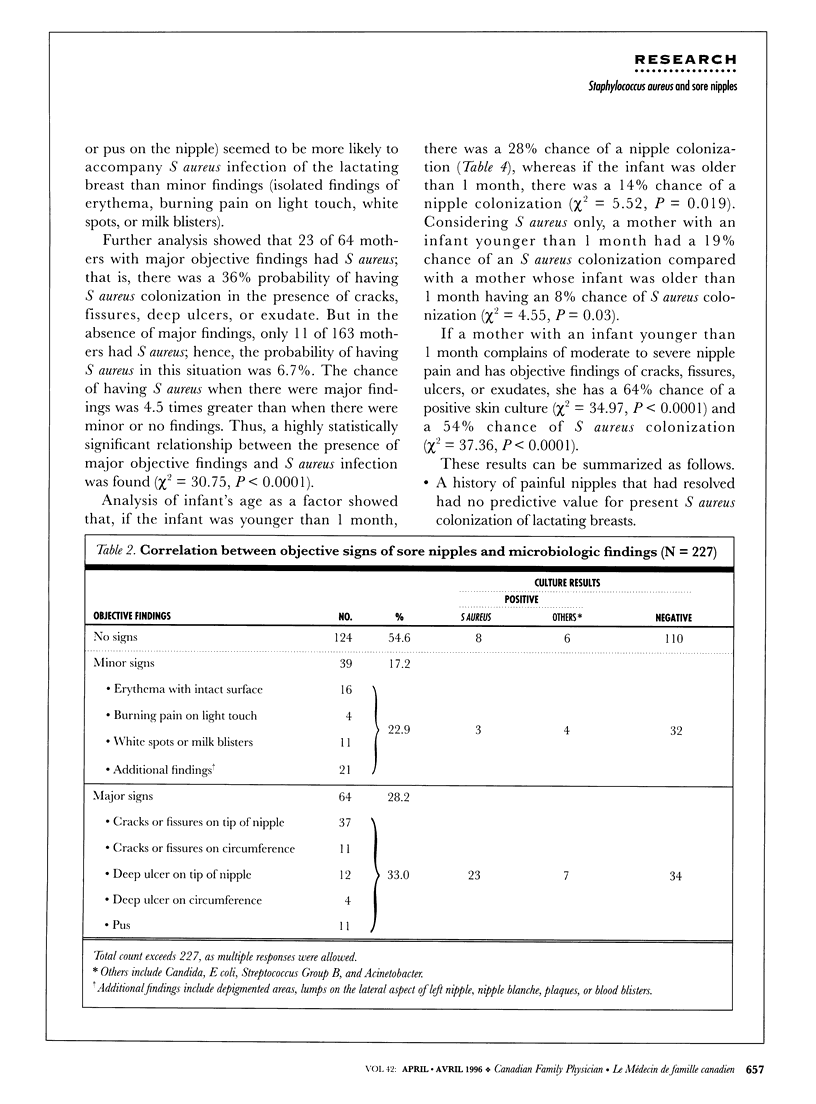
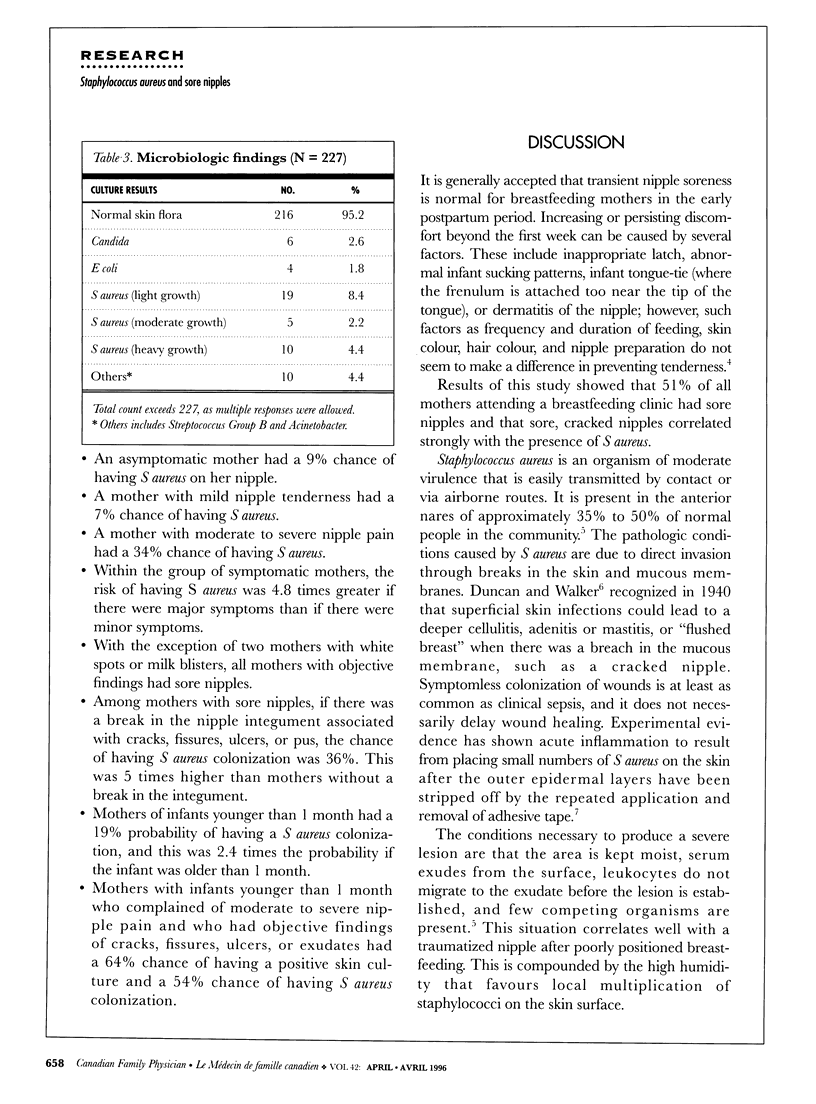
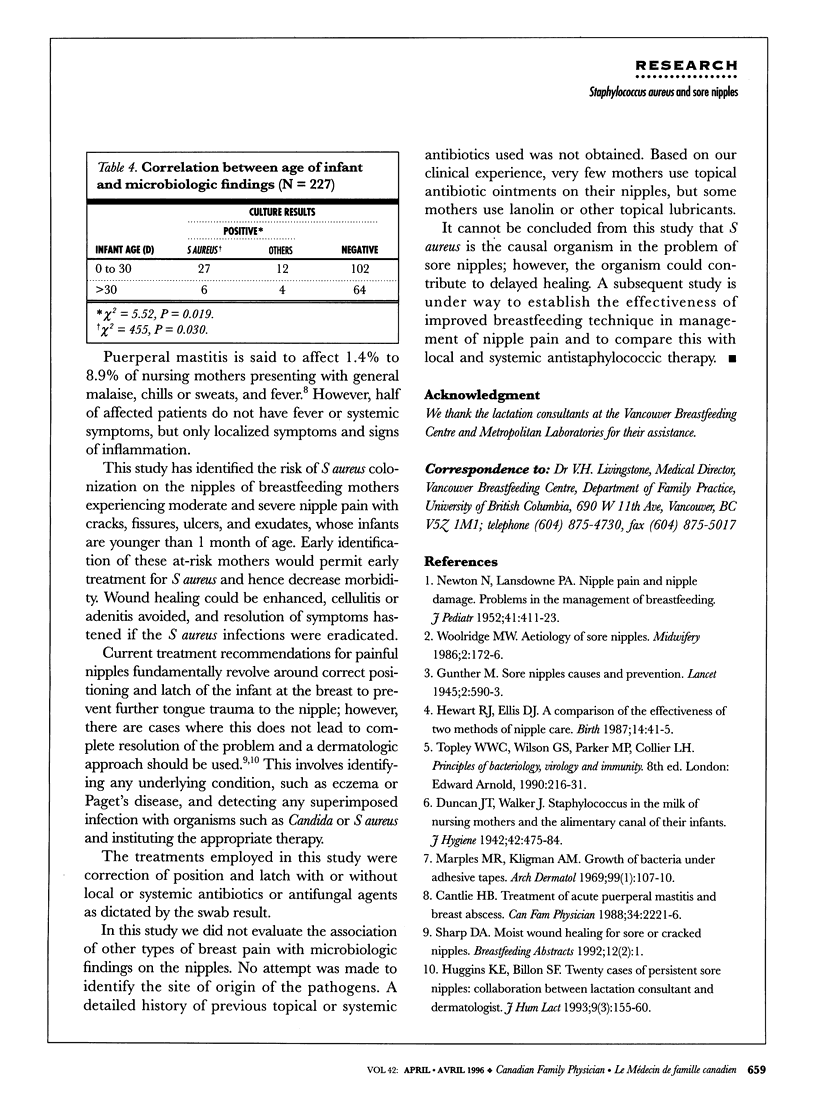
OBJECTIVE: To correlate clinical symptoms and signs of sore nipples with the presence of Staphylococcus aureus and to determine the probability of mothers having S aureus-infected nipples when these local symptoms and signs are found. DESIGN: Two cohorts of consecutive patients were enrolled regardless of presenting complaint. A questionnaire was administered to determine the presence and severity of sore nipples. Objective findings on breast examination were documented. A nipple swab was taken for culture and sensitivity. SETTING: Breastfeeding clinic serving patients referred by family physicians, pediatricians, and community health nurses. PATIENTS: A sample of 227 breastfeeding mothers was collected in two cohorts. MAIN OUTCOME MEASURES: Answers to questions about sore nipples, objective findings from physical examination, and results from nipple swabs. RESULTS: Most subjects (51%) had sore nipples, and 45% of subjects had objective findings on examination; 23% of subjects had a positive nipple swab culture; 15% grew S aureus on culture. The risk of having S aureus colonization was 4.8 times greater if nipple pain was moderate or severe rather than mild. A break in nipple integument associated with cracks, fissures, ulcers, or pus gave a 35% chance of having S aureus colonization, five times greater than when the integument was intact. CONCLUSIONS: The study showed that mothers with infants younger than 1 month who complained of moderate to severe nipple pain and who had cracks, fissures, ulcers, or exudates had a 64% chance of having positive skin cultures and a 54% chance of having S aureus colonization.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hewat R. J., Ellis D. J. A comparison of the effectiveness of two methods of nipple care. Birth. 1987 Mar;14(1):41–45. doi: 10.1111/j.1523-536x.1987.tb01447.x. [DOI] [PubMed] [Google Scholar]
- Huggins K. E., Billon S. F. Twenty cases of persistent sore nipples: collaboration between lactation consultant and dermatologist. J Hum Lact. 1993 Sep;9(3):155–160. doi: 10.1177/089033449300900313. [DOI] [PubMed] [Google Scholar]
- Marples R. R., Kligman A. M. Growth of bacteria under adhesive tapes. Arch Dermatol. 1969 Jan;99(1):107–110. [PubMed] [Google Scholar]
- Woolridge M. W. Aetiology of sore nipples. Midwifery. 1986 Dec;2(4):172–176. doi: 10.1016/s0266-6138(86)80042-0. [DOI] [PubMed] [Google Scholar]