

Abstract
Background
The occurrence of Loa loa encephalopathy following mass treatment of onchocerciasis with Mectizan® has adversely affected onchocerciasis control efforts in central Africa. Persons with very high densities of L. loa microfilaremia are at increased risk of encephalopathy, but little is known about the geographic distribution of these persons within central Africa. RAPLOA, a new technique that correlates the proportion of community members reporting a history of eyeworm with the prevalence of high-intensity L. loa microfilaremia in that community, may be useful for rapid assessment of areas at potential risk of treatment-related L. loa encephalopathy. Validation of RAPLOA is ongoing. The operational and risk-reduction advantages of RAPLOA over the current technique of village-by-village rapid epidemiologic assessment for onchocerciasis (REA) are unknown.
Methods
We developed a decision model to compare four strategies for minimizing sequelae of L. loa encephalopathy following mass treatment with Mectizan® in areas co-endemic for onchocerciasis and loiasis: REA; RAPLOA with threshold eyeworm prevalences of 40% and 20% (RAPLOA-40 and RAPLOA-20, respectively); and combined REA/RAPLOA-40.
Results
In the model, all four strategies significantly reduced risk of death and neurologic complications from L. loa encephalopathy, but RAPLOA-20 and REA resulted in half as many such cases as did RAPLOA-40 or combined REA/RAPLOA-40.
Conclusion
RAPLOA is likely to be useful programmatically in reducing risk of L. loa encephalopathy following mass treatment with Mectizan®. It also may be cost-saving. Before full-scale implementation, additional data are needed on geographic clustering of high-density L. loa microfilaremia and on RAPLOA's reliability and cost.
Background
For more than a decade, mass distribution of Mectizan® (ivermectin, MSD) has been recommended for prevention of blindness caused by infection with Onchocerca volvulus. The remarkable efficacy of Mectizan® against the microfilariae of O. volvulus, as well as the safety and effectiveness of the drug against a broad range of intestinal helminths and ectoparasites, has resulted in its acceptance at the community level. However, in recent years, serious adverse events (SAEs) associated with mass distribution of Mectizan® in Cameroon have caused widespread concern. Many of these SAEs were characterized by progressive neurologic decline and encephalopathy within a few days of taking Mectizan® [[1,2], Mectizan® Donation Program (MDP), unpublished data]. Affected persons lived in loiasis-endemic areas and, based on their post-treatment L. loa microfilarial loads, are presumed to have had high densities of L. loa microfilaremia prior to treatment with Mectizan® (MDP, unpublished data).
The Mectizan® Expert Committee (MEC) limits mass distribution of Mectizan® to areas considered meso- or hyper-endemic for onchocerciasis, as determined by the technique known as rapid epidemiologic mapping for onchocerciasis (REMO) [3]. REMO is based on rapid epidemiologic assessment (REA) for the presence of onchocercal nodules in samples of 30 adult men in selected indicator villages. Villages with a nodule prevalence of ≥ 40%, 20–39%, or <20% are defined as hyper-, meso-, or hypo-endemic, respectively. These estimates of onchocerciasis endemicity are projected onto larger geographical areas with similar ecologic characteristics [4]. Although residents of areas classified as hypo-endemic do not receive mass treatment with Mectizan®, they are eligible for individual clinic-based treatment if they are diagnosed with onchocerciasis.
REMO projections sometimes result in the inclusion of hypo-endemic villages into areas designated for mass distribution of Mectizan®. Until recently, such misclassifications of hypo-endemic villages had few, if any, known negative consequences. Individuals living in these villages benefited from Mectizan®'s action against intestinal helminths and ectoparasites, even if few of them suffered from onchocercal skin or eye disease. However, when cases of L. loa encephalopathy occurred following mass distribution of Mectizan®, the specificity of REMO (i.e. its ability to exclude hypo-endemic villages from mass drug distribution) was no longer considered adequate.
During the mid-1990s, reviews of the clinical features of Mectizan®-associated L. loa encephalopathy revealed that basic supportive care (i.e., hydration, feeding, and nursing care) was critical for patient recovery; indeed, prompt and sustained supportive care is the most important therapeutic measure [5]. Thus, mass distribution of Mectizan® in L. loa-endemic areas should be preceded by community education to increase awareness of possible SAEs following treatment. During and after mass drug distribution, intensified surveillance for SAEs is required, as is a referral system to appropriate health facilities for any SAEs that may occur [5]. In affected areas, these requirements have led to a temporary shift away from the strategy of community-directed treatment with ivermectin (CDTI) currently favored by the African Programme for Onchocerciasis Control (APOC). CDTI emphasizes community decision-making on the timing and manner of drug distribution by community volunteers (rather than by nurses or other medical personnel) [6,7].
In 2000, the MEC and the Technical Consultative Committee (TCC) of APOC recommended a new approach to mass treatment for onchocerciasis in areas co-endemic for loiasis. This approach begins with an environmental risk model based on remote sensing data for Central and West Africa. The model, developed by Madeleine Thomson and colleagues at the Liverpool School of Tropical Medicine, predicts the prevalence of L. loa infection based on vegetation and other land characteristics associated with a suitable environment for the presence of Chrysops spp., the vector of L. loa [8]. The model generates a map that, although still in the process of being validated, serves as an important operational starting point when considering whether a given area is likely to be endemic for loiasis [9]. For high-risk areas on the map, the MEC/TCC recommendations for areas co-endemic for onchocerciasis and loiasis currently require village-by-village REA before initiating mass treatment with Mectizan® [3,9]. Mass distribution of Mectizan® is recommended for all villages that remain classified as meso- or hyper-endemic for onchocerciasis by REA – but only after enhanced health education and training of community members, and only if SAE surveillance by community distributors and medical preparedness for SAE management can be ensured. In villages confirmed as hypo-endemic on the basis of REA, mass treatment is not recommended, although Mectizan® is made available to treat individuals with clinical onchocerciasis after health workers assess the individual's burden of L. loa microfilariae and related risk of L. loa encephalopathy.
This policy has financial and logistical implications. Increased costs result from village-by-village REA before treatment, as well as from safeguards required to reduce risk of death and disability from L. loa encephalopathy in hyper- and meso-endemic areas. Further, communities classified as hypo-endemic may be surrounded by meso- and hyper-endemic communities, and this can complicate the public health messages and interventions in both areas.
The current MEC/TCC approach assumes maximum risk of L. loa encephalopathy in all areas predicted as high risk on the environmental risk model map, and it uses village-by-village REA to increase programmatic certainty that "enough" onchocerciasis exists to warrant mass treatment with Mectizan®. This strategy focuses the mass treatment decision on the health benefits of preventing blindness rather than on the risk of L. loa encephalopathy following treatment. It was adopted because the only way to reliably predict risk of encephalopathy was to microscopically examine blood samples from all residents of a treatment area for L. loa microfilaremia before mass treatment. Operationally, this was thought to be difficult in remote parts of rural Africa.
A new technique, known as RAPLOA, has been developed that does not require collection of blood to detect areas with high-density L. loa microfilaremia [10]. A recent multi-center study showed that 1) the prevalence of L. loa infection is associated with microfilarial density; and 2) the prevalence of individuals with high-level microfilaremia in a community is associated with the percentage of community members who respond positively to questions about previous experience with a migrating eyeworm [11]. This study found that the most sensitive and specific rapid assessment tool was based on a "restricted" definition of eyeworm passage, in which the subject must recognize a photograph of eyeworm as the same condition that he or she had experienced, and the eyeworm episode must have lasted no more than 7 days. In three different ecologic settings in Nigeria and Cameroon, investigators found that the prevalence of persons with high microfilarial densities (≥30,000 microfilariae per milliliter [mf/ml] of blood) remained low when the prevalence of a history of eyeworm was less than 40%, but that it increased rapidly above this level (Figure 1, excerpted from the multi-country report on RAPLOA [10]).
Figure 1.
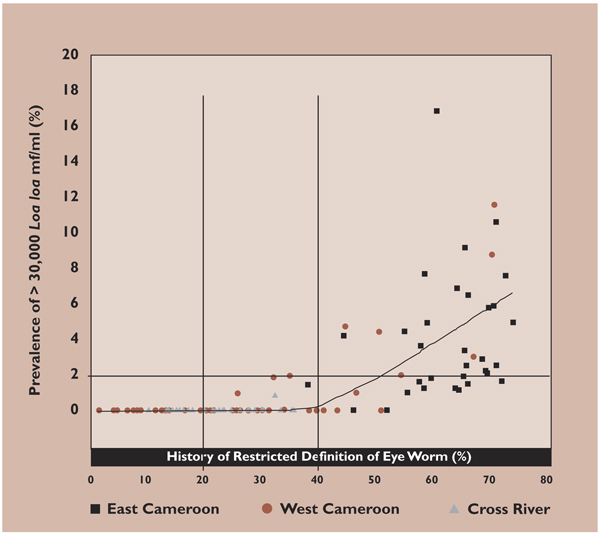
Prevalence of persons with L. loa microfilaremia ≥ 30,000 per ml as a function of the prevalence of a restricted definition of eyeworm, from Figure 10 of the multi-center report on RAPLOA [10]. See RAPLOA in the List of Abbreviations for details on the restricted definition of eyeworm.
RAPLOA is now being suggested as an alternate approach to REA in areas that are predicted by the environmental risk model map to be co-endemic for L. loa. Conceptually, such an approach, which bases the mass treatment decision on a defined risk of L. loa encephalopathy following Mectizan® treatment, seems more appealing than one based solely on an assessment of how much onchocerciasis is "enough" at the village level to justify an unknown risk of treatment-related L. loa encephalopathy. A threshold of 40% of persons with a history of eyeworm has been suggested for distinguishing between high-risk areas for L. loa encephalopathy (which would require enhanced community education, SAE surveillance, and supportive medical care) from those at low risk [10,11]. Presumably, the traditional CDTI approach to mass drug distribution could be used in areas categorized as low risk. We refer to RAPLOA based on a 40% threshold of eyeworm prevalence as RAPLOA-40.
Data on the sensitivity and specificity of RAPLOA are currently limited. A close examination of Figure 1 reveals that in some villages where <40% of persons have a history of eyeworm, as many as 2% of persons also have L. loa microfilarial densities of ≥30,000 per ml. These persons would be at risk of L. loa encephalopathy if mass distribution of Mectizan® were implemented. Use of 20% prevalence of a history of eyeworm as the threshold (RAPLOA-20) would substantially reduce (to near zero, based on Figure 1) the prevalence of persons with microfilarial densities of ≥30,000 per ml in areas classified as low risk. Another alternative, suggested by some, would be to apply both REA and RAPLOA-40 simultaneously in a given area to gather the maximum available information about both onchocerciasis and loiasis. With this strategy, once communities are confirmed by REA as hyper- or meso-endemic for onchocerciasis, RAPLOA-40 would be used to determine whether they are at high risk for L. loa encephalopathy following treatment with Mectizan®.
Rationale for a decision analysis model
Decision models can be useful to guide programmatic decisions, identify new research needs, identify critical decision points, and determine factors that most strongly influence both cost and safety. The primary purpose of the current model is to provide a structured framework to understand and estimate the potential health risks and benefits of alternative approaches to mass treatment strategies in areas that are co-endemic for onchocerciasis and loiasis. The broad conceptual framework underlying the model, described above, is shown graphically in Figure 2. The underlying assumptions of the model are based on the scientific literature and, when scientific data are lacking, on expert opinion and information available to the MDP (See additional file 1: Assumptions used in the decision model).
Figure 2.
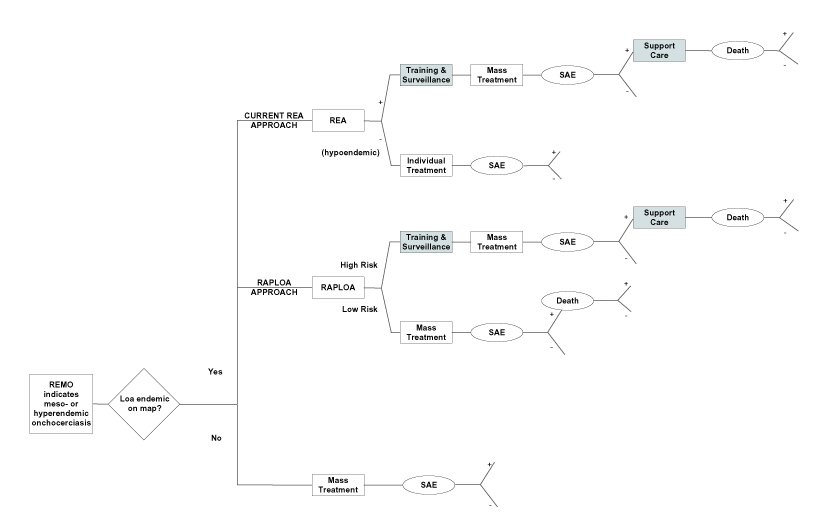
Conceptual framework for current and alternative approaches to minimizing risks and maximizing benefits of mass treatment with Mectizan® in areas suspected of being co-endemic for onchocerciasis and loiasis. Implementation of training, surveillance, and supportive care, indicated in shaded boxes, are assumed to reduce the risk of death associated with SAEs. + indicates the condition indicated -indicates the absence of the condition.
Methods
The model was constructed in the standard fashion using TreeAge software (Williamstown, MA). Four strategies (REA, RAPLOA-40, RAPLOA-20, and combined REA/RAPLOA-40) were examined (Figure 3) under four different ecologic conditions with varying intensities of O. volvulus and L. loa transmission (Appendix - see additional file 1). We examined three principal outcomes: 1) onchocercal blindness; 2) chronic neurologic complications or death associated with L. loa encephalopathy following Mectizan® treatment; and 3) disability-adjusted life years (DALYs), which were influenced by onchocercal blindness and skin disease as well as by treatment-related L. loa encephalopathy, death, and chronic neurologic sequelae (Appendix - see additional file 1) [12]. DALY losses for onchocercal blindness and skin disease were extrapolated from the Global Burden of Disease estimates (Appendix - see additional file 1) [12]. No similar estimates are available for Loa loa-related events. As a result, authors' estimates were used to reflect a short-term serious event (L. loa encephalopathy), a chronic severe event (permanent neurologic sequelae), and death at unknown age. Economic outcomes, particularly the costs associated with the various approaches, were not included because data were not available.
Figure 3.
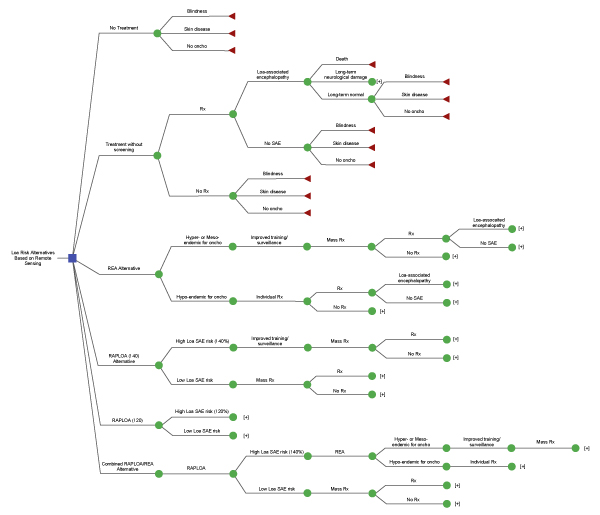
Decision model of four strategies to reduce risk of L. loa encephalopathy following treatment with Mectizan® in areas that are 1) thought to be endemic for loiasis on the basis of remote sensing (the environmental risk model map); and 2) determined to be hyper- or meso-endemic for onchocerciasis by REMO. Abbreviations: oncho = onchocerciasis; Rx = treatment. Additional details on the model are available from the authors upon request. [+] indicates truncation of a branch to simplify the figure. For the remainder of this branch, see the structure of similarly labelled branches elsewhere in the figure.
Risk of L. loa encephalopathy following Mectizan® treatment
The risk of L. loa encephalopathy temporally related to Mectizan® treatment was assumed to be a function of a threshold prevalence of high intensity microfilaremia, defined as 30,000 mf/ml of blood. This threshold was suggested previously by Ducorps and colleagues [1] and Boussinesq and co-workers [13]. Other investigators have suggested thresholds as high as 50,000 mf/ml [2] and as low as 10,000 mf/ml [5]. We assumed that the risk of L. loa encephalopathy following Mectizan® treatment was reduced by 50% in the second year of treatment.
The estimated risk of L. loa encephalopathy following Mectizan® treatment is based on two factors: 1) the percentage of communities with different portions of their population having microfilarial loads of ≥30,000 mf/ml (which we categorized as 0%, 0.1–0.9%, 1.0–1.9%, 2.0–3.9%, 4.0–7.9%, and ≥ 8%); and 2) risk of L. loa encephalopathy following Mectizan® treatment in individuals with microfilarial loads above the 30,000 mf/ml threshold, which we assumed to be 1% (Appendix - see additional file 1). The model estimates the prevalence of individuals with microfilarial loads of ≥30,000 mf/ml within communities that receive 1) mass treatment without additional education or enhanced SAE surveillance; 2) mass treatment with additional education and enhanced surveillance; or 3) clinic-based treatment for individuals diagnosed with onchocerciasis. These estimates are based on the estimated sensitivity and specificity of RAPLOA (Figure 1), the performance of REA, and the underlying distribution of high-intensity L. loa microfilaremia within communities (Appendix - see additional file 1). Four scenarios of varying L. loa prevalence were examined, two in which 60% of communities had ≥ 1 resident with high-density L. loa microfilaremia and two in which this figure was 10% (Appendix - see additional file 1).
Based on the estimated prevalence of individuals with high intensity infection, the community risk of L. loa encephalopathy following Mectizan® treatment was estimated. Three ultimate outcomes were considered: death, chronic or permanent neurological damage, and no adverse outcome. We assumed that the outcome of L. loa encephalopathy following Mectizan® treatment was influenced by the presence or absence of adequate supportive care for these patients (Appendix - see additional file 1).
Risk of Onchocerciasis
The model assumes that the lifetime risk of onchocercal blindness and skin disease is determined by the estimated community prevalence of onchocerciasis as determined by REA. In areas where the sowda form of onchocerciasis predominates, this assumption would underestimate risk of skin disease. In the high-prevalence scenarios for O. volvulus, the percentage of communities that were classified as hyper-, meso- and hypo-endemic for onchocerciasis was 60%, 30%, and 10%, respectively. For low-prevalence areas, these figures were 30%, 30% and 40%, respectively (Appendix - see additional file 1).
Since treatment halts progression of disease in those who already have clinical manifestations and prevents disease manifestations in those already infected or those not yet infected, we assumed that treatment is completely effective in eliminating the risk of morbidity due to onchocerciasis among treated individuals. We assumed that there was no impact of mass distribution on transmission or on risk of blindness or skin disease among persons who did not take Mectizan®. Thus, non-treated individuals were assumed to receive no benefit from mass treatment in their village. Drug coverage was considered to be systematic and to remain constant at 65%.
Results
Health benefits of Mectizan® treatment (DALYs and reduction in blindness)
In our model, onchocerciasis reduced average disability adjusted life years (DALYs) by 1.52 and 0.88 years per person in the high- and low-prevalence areas, respectively (Table 1). Although our model was conservative in assuming systematic annual drug coverage of only 65%, mass treatment with Mectizan® resulted in a net gain of 0.5 to 1.0 DALYs per person (reducing lost DALYs from 1.52 to 0.53 and from 0.88 to 0.31 in high - and low - prevalence areas, respectively), even in the absence of measures to reduce the risk of L. loa-associated death and permanent disability (Table 1).
Table 1.
Estimated mean disability-adjusted life years (DALYs) lost on a per-capita basis as a result of onchocercal blindness, skin disease, and L. loa encephalopathy, under conditions of: 1) no mass treatment with Mectizan®; 2) mass treatment with no risk reduction strategy; and 3) mass treatment using REA, RAPLOA-40, RAPLOA-20, or combined REA/RAPLOA-40 to reduce risk of L. loa encephalopathy. DALYs are expressed as mean years lost per person for the entire population. Four scenarios are considered based on high and low prevalence of loiasis and onchocerciasis, respectively (as defined in the Appendix - see additional file 1).
| Loiasis Prevalence | High | High | Low | Low |
| Onchocerciasis Prevalence | High | Low | High | Low |
| No Mectizan® treatment | 1.5155 | 0.8822 | 1.5155 | 0.8822 |
| Mectizan® treatment | ||||
| No risk reduction strategy | 0.5319 | 0.3102 | 0.5309 | 0.3092 |
| REA | 0.5393 | 0.3436 | 0.5391 | 0.3436 |
| RAPLOA-40 | 0.5307 | 0.3090 | 0.5305 | 0.3088 |
| RAPLOA-20 | 0.5305 | 0.3088 | 0.5305 | 0.3088 |
| REA/RAPLOA-40 | 0.5341 | 0.3228 | 0.5313 | 0.3124 |
Similarly, in our model, mass treatment with Mectizan® reduced the lifetime risk of blindness from 166 to 58 cases per 1000 population in areas with a high prevalence of onchocerciasis and from 94 to 33 cases per 1000 population in low prevalence areas. Because REA-based strategies to reduce Mectizan®-related L. loa encephalopathy result in fewer people receiving Mectizan®, these reductions in blindness were somewhat diminished in the presence of such strategies (Table 2).
Table 2.
Estimated risk of blindness per 1000 population in four scenarios based on high and low prevalence of loiasis and onchocerciasis, under conditions of: 1) no mass treatment with Mectizan®; 2) mass treatment with no risk reduction strategy; and 3) mass treatment using REA, RAPLOA-40, RAPLOA-20, or combined REA/RAPLOA-40 to reduce risk of L. loa encephalopathy.
| Loiasis Prevalence | High | High | Low | Low |
| Onchocerciasis Prevalence | High | Low | High | Low |
| No Mectizan® treatment | 166.0 | 94.0 | 166.0 | 94.0 |
| Mectizan® treatment | ||||
| No risk reduction strategy | 58.1 | 32.9 | 58.1 | 32.9 |
| REA | 58.7 | 35.5 | 58.7 | 35.5 |
| RAPLOA-40 | 58.1 | 32.9 | 58.1 | 32.9 |
| RAPLOA-20 | 58.1 | 32.9 | 58.1 | 32.9 |
| REA/RAPLOA-40 | 58.4 | 33.9 | 58.2 | 33.3 |
Reduction in L. loa associated SAEs
In the absence of any approach to reduce complications of L. loa encephalopathy following mass treatment with Mectizan®, the estimated risk of L. loa associated death or permanent neurologic sequelae was 85.1 and 26.0 cases per 1 million population in high- and low-prevalence areas for loiasis, respectively. All four risk-reduction strategies dramatically reduced the risk of these complications (Table 3). Regardless of the prevalence of onchocerciasis or loiasis, the current risk reduction strategy, REA, led to the greatest reductions (94% – 99%) in death and permanent disability associated with L. loa encephalopathy. Similar reductions (93–98%) were observed for RAPLOA-20. RAPLOA-40 and the combined REA/RAPLOA-40 approach were less effective in reducing risk (Table 3, Figure 4). Risk of L. loa associated death and disability was 2.0 to 6.7 times greater with RAPLOA-40 or REA/RAPLOA-40 than with REA or RAPLOA-20 (Table 3). Figure 4 illustrates the relationship between the estimated number of cases of blindness and the number of deaths and chronic disabilities resulting from L. loa encephalopathy in the context of 1) no mass treatment; 2) mass treatment with no risk reduction strategies; and 3) mass treatment with each of the four risk reduction strategies in the model.
Table 3.
Estimated risk of death or chronic disability per 1 million population resulting from L. loa encephalopathy following mass treatment with Mectizan®, under conditions of: 1) no mass treatment; 2) mass treatment with no risk reduction strategy; and 3) mass treatment using REA, RAPLOA-40, RAPLOA-20, or combined REA/RAPLOA-40 to reduce risk of L. loa encephalopathy. Four scenarios are considered based on high and low prevalence of loiasis and onchocerciasis, respectively (defined in the Appendix - see additional file 1).
| Loiasis Prevalence | High | High | Low | Low |
| Onchocerciasis Prevalence | High | Low | High | Low |
| No Mectizan® treatment | 0 | 0 | 0 | 0 |
| Mectizan® treatment | ||||
| No risk-reduction strategy | 85.1 | 85.1 | 26.0 | 26.0 |
| REA | 5.1 | 3.4 | 0.5 | 0.3 |
| RAPLOA-40 | 12.9 | 12.9 | 2.0 | 2.0 |
| RAPLOA-20 | 5.6 | 5.6 | 0.6 | 0.6 |
| REA/RAPLOA-40 | 12.4 | 11.0 | 2.0 | 1.9 |
Figure 4.
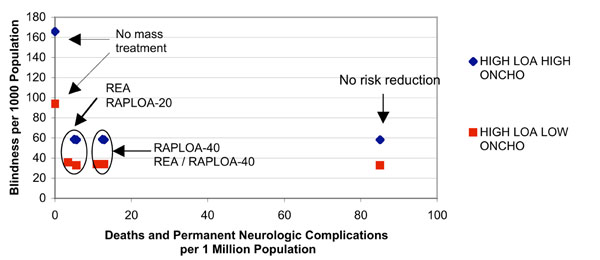
Estimated rates of lifetime blindness (per 1000 population) and of death and chronic disability from L. loa encephalopathy, under conditions of 1) no mass treatment with Mectizan®; 2) mass treatment with no risk reduction strategy; and 3) mass treatment using REA, RAPLOA-40, RAPLOA-20, or combined REA/RAPLOA-40. Data are shown for two levels of loiasis co-endemicity, both with highly endemic onchocerciasis. Similar patterns are observed in areas of low onchocerciasis endemicity (data not shown).
Discussion
The occurrence of L. loa encephalopathy following mass treatment with Mectizan® has negatively affected onchocerciasis control efforts in central Africa, which rely on a strategy of mass treatment with Mectizan® using CDTI. The lack of a rapid epidemiologic assessment tool to estimate risk of L. loa encephalopathy following Mectizan® treatment has severely limited attempts to expand onchocerciasis control into areas thought to be co-endemic for L. loa. RAPLOA could represent a significant advance in this regard. Validation of RAPLOA is currently ongoing and discussions are now underway about how best to apply RAPLOA programmatically to reduce risk of treatment-related L. loa encephalopathy and its complications.
Our model showed the substantial public health benefits of Mectizan® distribution, expressed either as DALYs or as blindness prevention, even in areas with co-endemic loiasis in which no measures to reduce L. loa associated risk were implemented. The model also indicated that all four risk-reduction strategies would substantially decrease the risk of death and permanent disability from L. loa encephalopathy temporally related to Mectizan® treatment (Figure 4). However, among the four strategies, differences were noted. Two approaches – the currently recommended REA and RAPLOA-20 – resulted in the greatest reductions in death and permanent disability from L. loa encephalopathy. In comparison, risk of death and permanent disability was about twice as high for the strategy based on RAPLOA-40. We found no advantage to a strategy that would employ a combination of REA and RAPLOA-40.
The currently recommended approach for reducing risk of death and permanent neurologic complications from L. loa encephalopathy incurs significant programmatic costs. These costs result from village-by-village assessments of onchocerciasis endemicity by REA, as well as the need to 1) educate at-risk communities about L. loa encephalopathy, 2) establish surveillance for treatment-related SAEs, and 3) provide appropriate supportive medical and nursing care for those who develop L. loa encephalopathy following mass treatment. Community education, surveillance, and supportive medical care are key elements in all four risk-reduction strategies evaluated in our model. Village-by-village RAPLOA would likely take about as long to execute as REA and would consume comparable financial and human resources. Data on the geographic distribution of high-intensity L. loa microfilaremia are limited. Thus, it is not yet certain that the results from a RAPLOA assessment in a small sample of villages would accurately predict the risk of SAEs throughout an entire area. In the absence of such a sampling scheme, village-by-village assessment using RAPLOA would be necessary and would likely provide no significant cost savings over village-by-village REA.
If RAPLOA is validated and found to be operationally reproducible and feasible, however, it would offer several advantages. Data collected through RAPLOA could significantly enhance our understanding of the epidemiology of high-density L. loa microfilaremia and provide an opportunity to refine the predictions of the environmental risk model map. The current approach of REA assumes that the map is 100% accurate in identifying areas that are highly endemic for loiasis. In these areas, onchocerciasis control programs are required invariably to carry out REA in every village and, in all villages where mass treatment with Mectizan® is offered, to bear the additional costs of enhanced training, SAE surveillance, and reinforcing health systems for the clinical management of L. loa encephalopathy. However, the environmental risk model map predicts risk of loiasis on the basis of environmental features that indicate favorable habitat for the Chrysops vector. It is possible (and likely) that many areas conducive to the vector do not have significant transmission of L. loa. Use of RAPLOA may reveal the absence of high-density L. loa microfilaremia (as predicted by history of eyeworm) throughout much of central Africa where the environmental risk model map currently predicts L. loa to be highly endemic. In these areas, mass treatment with Mectizan® could be instituted with no need for enhanced SAE training, surveillance, and medical systems. This would result in large cost savings at the regional level and vastly simplified program operations. Because the actual prevalence of high-density L. loa microfilaremia throughout much of central Africa is unknown and cost data were not available, we could not account for these potential advantages of RAPLOA in the decision model. Finally, the RAPLOA approach may prove useful in the Global Programme to Eliminate Lymphatic Filariasis for assessing risk of treatment-related L. loa encephalopathy in areas that are co-endemic for L. loa and Wuchereria bancrofti. In most of sub-Saharan Africa, this programme relies on mass treatment with both Mectizan® and albendazole [14].
A major challenge to all four risk-reduction strategies is the potential for misclassification, which may be substantial. Unfortunately, the cost of being able to rapidly detect and treat all cases of L. loa encephalopathy temporally related to Mectizan® treatment appears to be the establishment of surveillance and medical systems that, in many areas, may be unnecessary. The principal disadvantage of RAPLOA-20 is its relatively low specificity, which could result in large areas of central Africa being misclassified as high risk for L. loa encephalopathy and unnecessary expenditures of health resources. Because RAPLOA-40 is more specific, its use would avoid many of these unnecessary costs. However, our model suggests that RAPLOA-40 could result in twice as many L. loa associated deaths and cases of chronic disability, because this technique allows communities classified as low risk to have as many as 2% of persons with ≥30,000 L. loa mf/ml blood. These communities could therefore receive Mectizan® in the absence of adequate surveillance and systems to rapidly detect and treat L. loa encephalopathy. The magnitude of this problem would depend on the degree to which communities with persons at risk for L. loa encephalopathy are geographically clustered within areas classified as high risk by RAPLOA-40. If they are not tightly clustered, but rather scattered in relatively small numbers throughout central Africa, Mectizan®-related L. loa encephalopathy will be difficult to predict and even harder to prevent. The apparent clustering of reported cases of L. loa encephalopathy in certain regions of Cameroon is a reassuring sign in this regard. Further research on the performance of RAPLOA and on the geographic clustering of communities with persons with high microfilarial loads is urgently needed.
As with any decision model, the accuracy of our conclusions is limited by the uncertainty surrounding our assumptions. For many of our assumptions, published data are lacking and we relied on expert opinion and unpublished data available to the MDP. Even when data were available, especially on the epidemiology and health risks of L. loa, they were limited to a few studies in specific areas; the degree to which these data are representative for other areas in central Africa is not known. When we performed sensitivity analyses for the key variables in our model, our basic conclusions did not substantially change (data not shown).
Our decision model significantly underestimates the health benefits of Mectizan®. We considered as treatment-related benefits only prevention of onchocercal blindness and skin disease, and omitted benefits resulting from Mectizan®'s action against intestinal helminths, Strongyloides stercoralis, Wuchereria bancrofti, and a variety of ectoparasites. Our assumption that drug coverage was 65% is consistent with population-based coverage figures reported from onchocerciasis control programs in Africa. However, by assuming that this coverage was systematic, 35% of persons in affected communities would never have received Mectizan®. This assumption limited both the health benefits of Mectizan® and the number of persons with L. loa-associated encephalopathy. In a sensitivity analysis that assumed a random coverage pattern, with up to 100% of those targeted for mass treatment receiving one or more doses of Mectizan®, the conclusions of our model did not change. The relative effectiveness of each of the four strategies in reducing onchocercal blindness and the risk of L. loa associated death and disability remained constant (data not shown).
Conclusion
In central Africa where onchocerciasis and loiasis are co-endemic, L. loa encephalopathy has occurred following mass treatment with Mectizan®. In some cases, this has resulted in death or chronic disability. A new rapid assessment technique called RAPLOA may provide programme managers with an important tool with which to assess L. loa endemicity and the risk of treatment-related L. loa encephalopathy. Our decision model suggests that use of RAPLOA-20 or the current approach of REA would lead to the greatest reductions in death and permanent disability associated with L. loa encephalopathy. However, use of REA would result in fewer communities receiving Mectizan®. Compared to REA, the usefulness of RAPLOA, both in preventing blindness and avoiding L. loa encephalopathy following Mectizan® treatment in co-endemic areas, is highly dependent on the RAPLOA cutoff point. Full programmatic implementation of RAPLOA will require testing of the method in other areas of central Africa, an improved understanding of geographic clustering of high-density L. loa microfilaremia, sampling strategies that would avoid the need for RAPLOA assessments in all communities, cost analyses, and confirmation that the questionnaire can be administered easily and reliably by field staff.
List of abbreviations
APOC African Programme for Onchocerciasis Control
CDTI Community-directed treatment with ivermectin
DALY Disability-adjusted life year
MEC Mectizan® Expert Committee
MDP Mectizan® Donation Program
MSD Merck, Sharpe, and Dohme, Inc.
RAPLOA Rapid assessment procedure for Loa loa. The RAPLOA technique to which we refer in this paper uses a "restricted definition" of eyeworm [10,11]: the subject must recognize a photograph of eyeworm as the same condition that he or she is reporting, and the eyeworm episode must have lasted no more than 7 days.
REA Rapid epidemiologic assessment (for onchocerciasis)
REMO Rapid epidemiologic mapping of onchocerciasis
SAE Serious adverse event
TCC Technical Consultative Committee of the African Programme for Onchocerciasis Control
Competing interests
None declared.
Authors' contributions
All authors participated fully in extensive critical discussions as the model developed and in writing the paper. DA conceived of the study, helped develop the decision model, and was the primary author of the paper. RR developed the decision model and helped write the paper. NAYT-D conceived of the study, provided data, helped develop the decision model, and helped write the paper. FOR conceived of the study, provided critical data and perspective, helped refine the model, and helped write the paper. All authors read and approved the final manuscript.
Supplementary Material
Assumptions used in the decision model
Acknowledgments
Acknowledgements
The authors would like to thank Dr. Bjorn Thylefors, Director, Mectizan® Donation Program, for helpful discussions on study conceptualization and for his expert opinion on parameters for the model.
Contributor Information
David G Addiss, Email: dga1@cdc.gov.
Richard Rheingans, Email: rrheing@sph.emory.edu.
Nana AY Twum-Danso, Email: ntwumdanso@taskforce.org.
Frank O Richards, Email: fxr1@cdc.gov.
References
- Ducorps M, Gardon-Wendel N, Ranque S, Ndong W, Boussinesq M, Gardon J, Schneider D, Chippeaux J-P. Effets secondaires du traitement de la loase hypermicrofilarémique par l'ivermectine. Bulletin de la Societe de Pathologie Exotique et de ses Filiales. 1995;88:105–112. [PubMed] [Google Scholar]
- Gardon J, Gardon-Wendel N, Demanga-Ngangue , Kamgno J, Chippaux J-P. Serious reactions after mass treatment of onchocerciasis with ivermectin in an area endemic for Loa loa infection. Lancet. 1997;350:18–22. doi: 10.1016/S0140-6736(96)11094-1. [DOI] [PubMed] [Google Scholar]
- Noma M, Nwoke BEB, Nutall I, Tambala PA, Enyong P, Namsenmo A, Remme J, Amazigo UV, Kale OO, Sékétéli A. Rapid epidemiological mapping of onchocerciasis (REMO): its application by the African Programme for Onchocerciasis Control (APOC) Ann Trop Med Parasitol. 2002;96:29–40. doi: 10.1179/000349802125000637. [DOI] [PubMed] [Google Scholar]
- TDR (UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases) Guidelines for analysis of REMO data using GIS TDR/TDF/COMDT/98.3. Geneva World Health Organization. 1998.
- Anonymous Central Nervous System Complications of Loiasis and Adverse CNS Events following Treatment: Report of an Invited Consultation, 2–3 October 1995. Atlanta Mectizan Donation Program. 1996.
- Amazigo UV, Breiger WR, Katabarwa M, Akigun O, Ntep M, Boatin M, N'Doyo J, Noma M, Sékétéli A. The challenges of community-directed treatment with ivermectin (CDTI) within the African Programme for Onchocerciasis Control (APOC) Ann Trop Med Parasitol. 2002;96:41–58. doi: 10.1179/000349802125000646. [DOI] [PubMed] [Google Scholar]
- Homeida M, Braide E, Elhassan E, Amazigo UV, Liese B, Benton B, Noma M, Etya'alé D, Dadzie KY, Kale OO, Sékétéli A. APOC's strategy of community-directed treatment with ivermectin (CDTI) and its potential for providing additional health services to the poorest populations. Ann Trop Med Parasitol. 2002;96:93–104. doi: 10.1179/000349802125000673. [DOI] [PubMed] [Google Scholar]
- Thomson MC, Obsomer V, Dunne M, Connor SJ, Molyneux DH. Satellite mapping of Loa loa prevalence in relation to ivermectin use in west and central Africa. Lancet. 2000;356:1077–1078. doi: 10.1016/S0140-6736(00)02733-1. [DOI] [PubMed] [Google Scholar]
- Mectizan Expert Committee Recommendations for the treatment of onchocerciasis with Mectizan® in areas co-endemic for onchocerciasis and loiasis. Atlanta Mectizan Donation Program. 2000.
- TDR (UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases) Rapid assessment procedures for loiasis: report of a multi-centre study. TDR/IDE/RP/RAPL/01.1. Geneva World Health Organization. 2001.
- Takougang I, Meremikwu M, Wandji S, Yenshu EV, Aripko B, Lamlenn SB, Eka BL, Enyong P, Meli J, Kale O, Remme JH. Rapid assessment method for prevalence and intensity of Loa loa infection. Bull World Health Org. 2002;80:852–858. [PMC free article] [PubMed] [Google Scholar]
- Murray CJL, Lopez AD. The Global Burden of Disease. Cambridge Harvard University Press. 1996.
- Chippaux JP, Boussinesq M, Gardon J, Gardon-Wendel N, Ernould JC. Severe adverse reaction risks during mass treatment with ivermectin in loiasis-endemic areas. Parasitol Today. 1966;12:448–450. doi: 10.1016/0169-4758(96)40006-0. [DOI] [PubMed] [Google Scholar]
- World Health Organization Lymphatic filariasis. Weekly Epidemiological Record. 2002;77:125–132. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Assumptions used in the decision model