

Abstract
Clubfoot correction by the Ponseti method is highly successful with an average of 5 casts in the majority of patients. However, early experience with the technique demonstrated that many cases required more than 5 casts for correction. The purpose of this study was to evaluate the effects of timing of cast removal before subsequent manipulation and casting in the correction of clubfoot using the ponseti method. We reviewed 90 patients (129 clubfeet) treated between december 2000 and June 2006. two groups were evaluated. group a: 44 patients (63 clubfeet) had their cast removed by the parents the night before the visit. group b: 46 patients (66 feet) had their cast removed in the clinic just before the new casts were applied. Overall, full correction was obtained in 128 (99%) clubfeet, with only 1 clubfoot requiring surgical release. group a required an average of 10 casts (range: 4 to 22), compared to 5 casts (range: 4 to 10) in group b (p=0.001). average time for correction was 13 weeks in group a and 6 weeks in group b (p=0.001). there were 20 relapses (22%), 12 (27%) in group a and 8 (17%) in group b (p=0.42). in conclusion, removing the cast just before the new cast is applied significantly decreases the number of casts required for correction and shortens the length of treatment.
INTRODUCTION
Idiopathic clubfoot is the most common musculoskeletal birth defect, affecting an average of 1 in 750 newborns. Most orthopedists agree that initial treatment should be non-surgical and started soon after birth. In the past few years, several reports have demonstrated successful correction in >95% of the clubfeet using the Ponseti method.1–18 Interestingly, there is some variation in the reported average number of casts required to obtain full correction. At our institution in Chile, early experience with this method demonstrated that many patients required more than 5 casts for correction. We hypothesized that these feet were more severely involved, therefore, requiring more casts. However, it has been our practice to request the parents to remove the cast the night before the visit to allow for skin care. This recommendation differs from the Ponseti method which requires the cast to be removed just before the new cast is applied. The purpose of this study was to evaluate the effects of timing of cast removal in clubfoot correction by the Ponseti method.
MATERIALS AND METHODS
We reviewed the records of 90 patients with congenital idiopathic clubfoot (129 clubfeet) consecutively treated by one of the authors (GTL) between December 2000 and June 2006. Positional and syndromic clubfeet were not included. Institutional review board approval was obtained. No patient has been lost to follow-up.
The treatment technique followed the principles of correction described by Ponseti.19–21 However, at our institution we have traditionally asked the parents to remove the cast the night before the visit to allow for skin care. Therefore, our method should be considered a modification of the Ponseti protocol that requires the cast to be removed just before the new cast is applied. Importantly, after a visit to the University of Iowa in October 2003, we modified our cast removal protocol to precisely follow the Ponseti recommendations. Based on this change, we evaluated two groups of patients based on the timing of cast removal. Group A: 44 patients (63 clubfeet) were studied retrospectively. These patients had their cast removed by the parents the night before the visit. Group B: 46 patients (66 feet) were studied prospectively. They had their cast removed in the clinic just before the new casts were applied.
We evaluated the following variables: age of the patient at first visit to our institution; previous treatment before referral: type, number of casts, tendoachilles tenotomy; number of casts required at our institution; need for percutaneous tendoachilles tenotomy; degree of ankle dorsiflexion after tenotomy; and compliance with the foot abduction brace. These variables were in turn related to the need for extensive corrective surgery and the incidence of relapses. Fisher's exact tests, t-tests, and odds ratios were used as appropriate.
RESULTS
Sixty-four patients (71%) were males. The majority of patients were otherwise healthy (72%) and most children (92%) were full-term, without complications during pregnancy or delivery. Seventy-nine patients (60%) were first-born. Thirty-three patients (22%) had a positive family history of clubfoot deformity. Developmental dislocation of the hip was observed in 10% of the patients. At initial Ponseti casting, all patients but three were younger than 6 months old.
Three patients had some manipulations and casting before their initial visit to our institution. None of these patients had a percutaneous tendoachilles tenotomy. These three patients came to the clinic with all the components of the deformity uncorrected. Clubfoot correction was obtained in all clubfeet but one (n=128, 99% correction). This patient from Group A had a very stiff, bilateral deformity.
As shown in Figure 1, there was a significant difference between groups in the average number of casts required for correction: 10 casts (range, 4 to 22) in Group A, and 5 casts (range, 4 to 10) in Group B (p=0.001). In addition, there was a significant difference in the time from first cast to correction. In Group A, it took an average of 13 weeks compared to 6 weeks in Group B (p=0.001). Percutaneous tendoachilles tenotomy was performed in 81% of the cases overall, but the Group B patients required far fewer tenotomies than the Group A patients (Group A, 98% vs Group B, 65%) (Figure 2). Average ankle dorsiflexion post-tenotomy was 20 degrees (range, 0 to 35 degrees), with no significant differences between groups. The patients started to walk at an average age of 14 months (range, 12 to 20 months).
Figure 1.
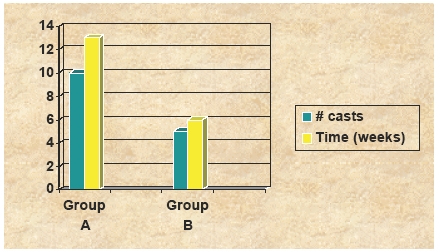
Aaverage number of casts required for correction, and time (weeks) from first visit to the performance of the tendoachilles tenotomy.
Figure 2.
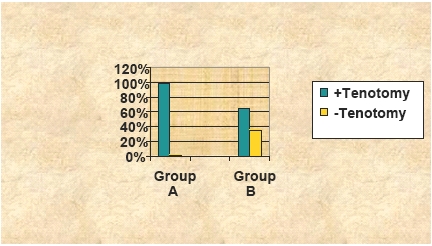
Ppercentage of patients requiring tendoachilles tenotomy to obtain full correction of the clubfoot deformity.
Four patients (4%) had a cast complication that included skin redness or slight swelling of the toes. These complications were attributed to a deficient casting technique. No infections, skin necrosis, neurovascular compromise or profuse bleeding post-tenotomy were observed. One patient had a slight over-correction that resolved over time and that did not affect when he started walking or the need for orthopedic shoes or inserts.
There were 20 relapses (22%) after initial successful treatment: 12 (27%) in Group A and 8 (17%) in Group B (p=0.42). The average age at relapse was 14 months (range, 4 to 27 months). Relapses were not significantly related to age at presentation or previous unsuccessful treatment at another institution. Relapses were, however, associated with non-compliance with the foot-abduction brace (p=0.001). Relapses were treated with a second series of manipulation and casting, followed by the use of the foot-abduction brace. Two patients required a second tendoachilles tenotomy, and another patient required tendoachilles lengthening and anterior tibialis transfer to the third cuneiform to prevent further relapses.
At the last follow up, patients were evaluated for foot/calf shape and range of motion of the ankle. All patients had normal looking feet (although slightly smaller than the normal side) but smaller calf muscle mass. Plantar-flexion (average=36 degrees) and dorsi-flexion (average=22 degrees) were also slightly decreased compared to accepted normal values. No patient had pain or limitation of activities of daily living. All patients used regular shoes.
DISCUSSION
This report is the first from Chile demonstrating a very high correction rate (99%) for idiopathic clubfoot using the Ponseti method, and confirms the results of other recently published series.1–18 Importantly, we have found that the timing of cast removal is associated with a dramatic decrease in the number of casts required for correction and also in the length of treatment. Both of these outcomes can have significant financial benefits for the families. Based on the very low complication rate in this series, we see no need to remove the cast the night before for skin care as traditionally recommended at many institutions. In addition, this study also demonstrates that following the published Ponseti technique and protocol to the smallest detail greatly improves the chance of achieving the outstanding results published by many other groups.
We have observed a high rate of relapses (22%) and, as many other groups have pointed out, most of these cases were due to non-compliance with the brace.1,3,5,6,8–11,13,14 This problem stresses the need for developing educational programs for the parents as well as other healthcare providers to maximize bracing compliance. It has been our experience that other physicians who are not very familiar with the method and protocol recommendations have allowed parents to discontinue the use of the brace much earlier than required. These cases almost always result in relapse.
We have also changed our clinic schedule to accommodate all clubfoot patients on a single day. This practice allows parents to share their concerns and questions with other parents, and to see that the results are predictable and lead to normal foot function. It also creates an environment of “peer pressure” where parents who are not compliant with the brace are exposed to other parents and children who are wearing the brace. It allows parents the opportunity to share techniques leading to easier brace wear. Furthermore, it has helped in the development of a network of parents in our country that are very supportive of the method.
Finally, it is also very important to work with local orthothic providers to understand the method and to help in the development of a brace suited for the financial conditions of the family as well as the country. Ultimately, it would be ideal if there were a standardized, comfortable and low-cost brace that would work for all families, both in developed and undeveloped countries.
In conclusion, removing the cast just before the new one is applied significantly decreased the number of casts required for correction and shortened the time of treatment. Following the principles and technical details of the Ponseti method will assure optimal results in almost all patients.
References
- 1.Abdelgawad AA, Lehman WB, van Bosse HJ, Scher DM, Sala DA. Treatment of idiopathic clubfoot using the Ponseti method: minimum 2-year follow-up. J Pediatr Orthop B. 2007;16(2):98–105. doi: 10.1097/BPB.0b013e32801048bb. [DOI] [PubMed] [Google Scholar]
- 2.Bor N, Herzenberg JE, Frick SL. Ponseti management of clubfoot in older infants. Clin Orthop Relat Res. 2006;(444):224–8. doi: 10.1097/01.blo.0000201147.12292.6b. [DOI] [PubMed] [Google Scholar]
- 3.Changulani M, Garg NK, Rajagopal TS, Bass A, Nayagam SN, Sampath J, Bruce CE. Treatment of idiopathic club foot using the Ponseti method. Initial experience. J Bone Joint Surg Br. 2006;88(10):1385–7. doi: 10.1302/0301-620X.88B10.17578. [DOI] [PubMed] [Google Scholar]
- 4.Chotel F, parot R, Durand JM, Garnier E, Hodgkinson I, Berard J. Initial management of congenital varus equinus clubfoot by Ponseti's method. Rev Chir Orthop Reparatrice Appar Mot. 2002;88(7):710–7. [PubMed] [Google Scholar]
- 5.Colburn M, Williams M. Evaluation of the treatment of idiopathic clubfoot by using the Ponseti method. J Foot Ankle Surg. 2003;42(5):259–67. doi: 10.1016/s1067-2516(03)00312-0. [DOI] [PubMed] [Google Scholar]
- 6.Dobbs MB, Rudzki JR, Purcell DB, Walton T, Porter KR, Gurnett CA. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am. 2004;86-A(1):22–7. doi: 10.2106/00004623-200401000-00005. Jan. [DOI] [PubMed] [Google Scholar]
- 7.Eberhardt O, Schelling K, Parsch K, Wirth T. Treatment of congenital clubfoot with the Ponseti method. Z Orthop Ihre Grenzgeb. 2006;144(5):497–501. doi: 10.1055/s-2006-942239. [DOI] [PubMed] [Google Scholar]
- 8.Goksan SB, Bursali A, Bilgili F, Sivacioglu S, Ayanoglu S. Ponseti technique for the correction of idiopathic clubfeet presenting up to 1 year of age. A preliminary study in children with untreated or complex deformities. Arch Orthop Trauma Surg. 2006;126(1):15–21. doi: 10.1007/s00402-005-0070-9. [DOI] [PubMed] [Google Scholar]
- 9.Goksan SB. Treatment of congenital clubfoot with the Ponseti method. Acta Orthop Traumatol Turc. 2002;36(4):281–7. [PubMed] [Google Scholar]
- 10.Gupta A, Singh S, Patel P, Patel J, Varshney MK. Evaluation of the utility of the Ponseti method of correction of clubfoot deformity in a developing nation. Int Orthop. 2006 doi: 10.1007/s00264-006-0284-7. Nov 18; [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop. 2002;22(4):517–21. [PubMed] [Google Scholar]
- 12.lehman WB, Mohaideen A, Madan S, Scher DM, van Bosse HJ, Iannacone M, Bazzi JS, Feldman DS. A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot. J Pediatr Orthop B. 2003;12(2):133–40. doi: 10.1097/01.bpb.0000049579.53117.4a. [DOI] [PubMed] [Google Scholar]
- 13.Morcuende JA, Dolan LA, Dietz FR, Ponseti IV. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics. 2004;113(2):376–80. doi: 10.1542/peds.113.2.376. [DOI] [PubMed] [Google Scholar]
- 14.Morcuende JA, Abbasi D, Dolan LA, Ponseti IV. Results of an accelerated Ponseti protocol for clubfoot. J Pediatr Orthop. 2005;25(5):623–6. doi: 10.1097/01.bpo.0000162015.44865.5e. [DOI] [PubMed] [Google Scholar]
- 15.Radler C, Suda R, Manner HM, Grill F. Early results of the Ponseti method for the treatment of idiopathic clubfoot. Z Orthop Ihre Grenzgeb. 2006;144(1):80–6. doi: 10.1055/s-2006-921413. [DOI] [PubMed] [Google Scholar]
- 16.Segev E, Keret D, Lokiec F, Yavor A, Wientroub S, Ezra E, Hayek S. Early experience with the Ponseti method for the treatment of congenital idiopathic clubfoot. Isr Med Assoc J. 2005;7(5):307–10. [PubMed] [Google Scholar]
- 17.Shack N, Eastwood DM. Early results of a physiotherapist-delivered Ponseti service for the management of idiopathic congenital talipes equinovarus foot deformity. J Bone Joint Surg Br. 2006;88(8):1085–9. doi: 10.1302/0301-620X.88B8.17919. [DOI] [PubMed] [Google Scholar]
- 18.Tindall AJ, Steinlechner CW, Lavy CB, Mannion S, Mkandawire N. Results of manipulation of idiopathic clubfoot deformity in Malawi by orthopaedic clinical officers using the Ponseti method: a realistic alternative for the developing world? J Pediatr Orthop. 2005;25(5):627–9. doi: 10.1097/01.bpo.0000164876.97949.6b. [DOI] [PubMed] [Google Scholar]
- 19.Ponseti IV, Smoley EN. Congenital Clubfoot: The Results of Treatment. Bone and Joint Surg. 1963;45-A:261–27. [Google Scholar]
- 20.Ponseti IV. Congenital Clubfoot. Fundamentals of Treatment. Oxford: Oxfprd Medical Publications; 1996. [Google Scholar]
- 21.Morcuende JA, Weinstein SL, Dietz FR, Ponseti IV. Plaster Cast Treatment of Clubfoot:The Ponseti Method of Manipulation and Casting. J. Pediatr. Orthop. 1994;3(Part B):161–167. [Google Scholar]