

Abstract
Objectives. We compared reports of sexual behaviors given in standard face-to-face interviews with reports given in audio computer-assisted self-interviews (ACASIs) and culturally specific interactive interviews among adolescents in India. We sought to determine which of the interview methods leads to higher reporting of sexual behaviors among economically disadvantaged 15–19-year-olds in urban India.
Methods. We conducted a randomized trial in which each participant (583 boys and 475 girls) was assigned to 2 interview methods: face-to-face interview and ACASI or interactive interview. We used matched case–control analyses to assess differences in the individual’s reporting on the 2 methods.
Results. Female participants consistently reported fewer sexual behaviors in ACASIs than in face-to-face interviews, whereas male participants’ reports differed according to type of sexual behavior and interview mode. Both male and female participants reported more sexual behaviors during interactive interviews than during face-to-face interviews. Twenty-eight percent of male participants reported having engaged in heterosexual intercourse in interactive interviews, as compared with 20% in face-to-face interviews (P< .01); the corresponding percentages for female participants were 7% and 2% (P<.01).
Conclusions. Our results showed that young people were more likely to report sexual behaviors in culturally specific interactive interviews than in face-to-face interviews. By contrast, ACASIs did not uniformly lead to higher reporting levels than did face-to-face interviews.
Sexual health issues can be intensely private and at the same time circumscribed by strict social norms. Understandably, it is often difficult to gather accurate information on sexual behaviors,1 and this is especially the case with young people in settings where premarital sexual experience is taboo. However, such information is essential if reproductive health programs aimed at young people are to be effective. Given that the global population of 10- to 19-year-olds is 1.2 billion,2 there is an urgent need for initiatives targeting the needs of this group.
In India, adolescent health issues have been largely neglected, even though the country is home to 230 million adolescents.3–5 The sexual health of young men and young women has gained attention in India only recently, and this attention has been the result of concern that adolescents will be the group worst hit by the country’s AIDS epidemic.6,7
Face-to-face interviews are the most frequently used method of obtaining information on adolescents’ sexual behaviors. However, they may lead to underreporting because of concerns about privacy and confidentiality, fear of judgment on the part of interviewers, and social desirability bias (i.e., the desire to present oneself in a manner that will be viewed favorably by others).8–10 Audio computer-assisted self-interviews (ACASIs) have been suggested as an effective alternative that will encourage honest reporting of sensitive behaviors.1,11–15 ACASIs involve a standardized measurement system in which all respondents answer the same questions; as a result, interviewer biases are limited. Also, ACASIs feature quality checks (e.g., monitoring of response consistency) and efficient multilingual administration, and they create an automatic data set that can be used immediately.1,12–16
However, the ACASI format does not provide an opportunity to probe or clarify potentially misunderstood or unclear questions. Respondents can skip questions, or they can respond to questions without according them a sufficient amount of thought.9
The ACASI format has not been used extensively in developing countries. However, in a recent Brazilian study in which biomarkers for sexually transmitted infections were used to validate interview-based reports of sexual behaviors among literate women aged 18 to 40 years, results showed that ACASIs led to significantly higher reporting rates than did face-to-face interviews.17 The results of a methodological experiment conducted in Kenya18 showed a mixed pattern. ACASIs produced a more diverse picture of adolescent sexual activity than did face-to-face interviews. However, adolescent girls were significantly more likely to report having had sexual intercourse in face-to-face interviews than in ACASIs or self-administered interviews.18,19
In another study, designed to assess the feasibility of ACASI in Zimbabwe, 86% of women preferred ACASIs to face-to-face interviews. However, 53% of women with a primary school education or less reported problems with computer use (as compared with only 10%–12% of women in higher educational groups).16
Finally, a randomized trial conducted in Pune, India,20 that involved 1500 unmarried men aged 18 to 22 years compared reports of stigmatized sexual behaviors in ACASIs, face-to-face interviews, and self-administered interviews. Results showed that respondents more frequently reported behaviors such as masturbation, oral sex, and homosexual activity in ACASIs than in face-to-face interviews. Although ACASIs were successful in eliciting information among computer-literate college students, results from less-educated men living in economically disadvantaged neighborhoods were mixed. Men living in these neighborhoods more often reported having sexual intercourse in face-to-face interviews than in ACASIs (35% vs 11%; P = .001).
We conducted a randomized crossover study in Delhi, India, in which we compared young people’s reports of their sexual behaviors in standard face-to-face interviews with their reports in ACASIs and interactive interviews. We hypothesized that, in comparison with face-to-face interviews, ACASIs and interactive interviews would produce less social desirability bias and would encourage more-honest reporting of sexual behaviors and experiences.
METHODS
Study Design
Participants were young people from economically disadvantaged urban neighborhoods in Dakshin Puri, Delhi, India. A household enumeration in November 2003 and March to April 2004 preceded the trial. All households in 5 contiguous neighborhoods were enumerated, and we identified 1205 unmarried boys and girls aged 15 to 19 years in 2118 households.
The 3 interview methodologies compared in this study—ACASI, interactive, and face to face—involved the same closed-ended questions. Interview methodologies were pretested in April and May 2004 in a disadvantaged neighborhood that we did not include in the trial. We organized a 7-day training program for 24 interviewers in July 2004 to communicate our research aims and procedures as well as specific survey protocols (e.g., not probing during the interviews and refraining from demonstrating strong reactions to respondents’ responses). Interviewers were told that breach of respondents’ confidentiality could be a basis for dismissal from the survey team.
The randomized trial was conducted between August and November 2004. All unmarried 15- to 19-year-olds living in 4 neighborhoods of Dakshin Puri were eligible to participate. In families with more than 1 eligible adolescent, all eligible adolescents were invited to participate. Community sensitization initiatives, which took place at least once a week, were organized before the recruitment process began. These initiatives helped to introduce the trial and the team members to the community in an informal manner, to identify support groups from within the community, and to divide the neighborhood into subareas for recruitment of participants.
At the interview site, the research assistant gave each participant an envelope bearing an identification number with a slip that specified the interview sequence and type of interview methodology to which they would be assigned. All of the participants provided sociodemographic information and then completed 2 interviews in a predetermined sequence (Figure 1 ▶). Interviewers and participants were gender matched, and all interviews were administered on the same day.
FIGURE 1—

Flowchart of study randomization plan among young people aged 15 to 19 years: Delhi, India, 2004.
Note. ACASI = audio computer-assisted self-interview.
To maintain respondents’ confidentiality, we did not ask whether more than 1 adolescent from the same household was taking part in the trial and did not include an identification variable for matching by household. Considering the nature of the survey, complete privacy was necessary to ensure confidentiality, and privacy was maintained across the 3 interview methods. During administration of face-to-face and interactive interviews, only 1 interviewer and 1 respondent were present in the room. In another room, 2 or 3 computers facing opposite directions were used to administer ACASIs through headphones.
We used Stata version 7 to determine the random allocation sequence.21 To assess the influence of the order in which interviews were administered on participants’ responses, we randomized young people into 1 of 4 interview groups: (1) face-to-face interview followed by ACASI, (2) ACASI followed by face-to-face interview, (3) face-to-face interview followed by interactive interview, or (4) interactive interview followed by face-to-face interview. The planned sample size for the trial was 960, with 120 male participants and 120 female participants randomized to each of the 4 groups. At a power of 80% and an alpha level of .025 (allowing comparisons between more than 2 groups), this sample size would have allowed detection of differences by interview mode of 8% or more. The final sample included 583 boys and 475 girls.
On average, 90 to 120 minutes were required to administer the full protocol. Interviewers rotated through the different interview methodologies. Several steps were implemented to ensure data quality. Data were checked daily, and clarifications were sought from the interviewers if reports of very sensitive behaviors (e.g., having engaged in sexual intercourse) were more or less frequent than expected. For the first 2 or 3 weeks, the interviewers, the principal investigator, Jaya, and the individual responsible for checking the data met every 2 or 3 days for clarifications and feedback. Later, these meetings were held once a week to sort out issues as they arose. Interviewers were encouraged to share any difficulties they had in asking questions.
Interview Methodologies
The face-to-face interview methodology was developed in collaboration with Samudayik Shakti, a nongovernmental social organization in Delhi. The questionnaire used in these interviews was pretested with 25 girls and 23 boys and underwent 7 revisions before it was finalized. This questionnaire provided cues for developing the questionnaires used in the ACASIs and interactive interviews.
The ACASI software was developed by Geetika Software of India. Each question had a maximum of 4 response options (yes, no, do not know, no response) that were represented by visual images. The participant heard the question and the possible responses through headphones and used the computer mouse to click on the selected response. Voiceovers were gender matched. If necessary, participants could listen to a question a second time and modify their responses.
The ACASI methodology was pretested with 9 male and 10 female participants. Pretesting suggested that participants were able to use this methodology even though they had had minimal or no exposure to computers. Before they began their self-interviews, participants were trained with 5 dummy questions on movie stars to help them practice using the mouse. Also, interviewers were available outside the room if participants needed clarifications.
The interactive interviews were developed in collaboration with Vikalp Design of India. They were interviewer administered and were supported by several audiovisual aids. Pretesting of these interviews focused on cultural sensitivity, comprehension, and relevance of the audiovisual aids. The interviews were pre-tested with 10 male and 9 female participants from the same neighborhood in which the face-to-face interviews had been pretested.
Interactive interviews included a 5-segment audio drama that re-created realistic situations as a means of decreasing participants’ embarrassment in reporting on issues related to sexuality. Male and female dolls were used to ask questions on sensitive issues such as same-sex behaviors. Participants were given a confidential individual response sheet for answering questions regarding heterosexual behaviors. The response sheet included appropriate visuals enabling illiterate participants to mark their responses. The interviewer explained the questions on the master sheet while the participant followed on his or her sheet. After marking their responses, participants folded the response sheet and dropped it into a box. The response sheet for female participants is shown in Figure 2 ▶.
FIGURE 2—
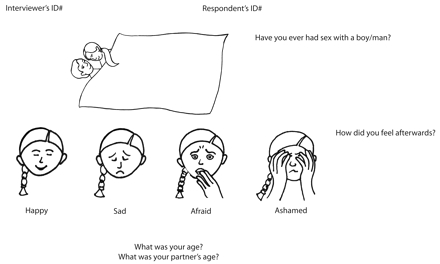
Confidential response sheet used by female respondents to report sexual behaviors in interactive interviews: Delhi, India, 2004.
Statistical Analyses
We used Stata to analyze the data. We conducted all analyses separately for male and female participants, and we conducted multivariate logistic regression analyses to determine whether the order in which interviews were administered affected participants’ responses. The order in which interviews were administered was not significantly related to reporting levels (data not shown). Hence, we collapsed the data according to interview method. We conducted analyses comparing individual responses on either face-to-face interviews and ACASI, or face-to-face interviews and interactive interviews. We examined whether randomization was successful by comparing the sociodemographic characteristics of individuals in the 2 groups. We used the χ2 test to assess categorical variables and the Bartlett test of equal variance to assess continuous variables. We conducted a matched case–control analysis to examine individual-level differences in responses.
RESULTS
Although we identified 1205 eligible adolescents at the time of the household enumeration, we identified 1293 eligible adolescents (719 boys, 574 girls) during the actual recruitment process conducted 6 to 9 months later; 1058 adolescents (583 boys and 475 girls) participated in the trial. The overall response rate was 82% (81% for male participants and 83% for female participants). There were very few questions on which responses were missing (0.2% to 1%). Average ages were 17 years for male participants and 16 years for female participants. Approximately one third of the participants were enrolled in school at the time of the trial.
Nearly three quarters of male participants (73%) and more than half of female participants (54%) reported having had a job. Thirty-six percent of male participants and 56% of female participants were members of families with a monthly income of less than 3000 rupees ($70). Almost three fourths of the participants were Hindu. Table 1 ▶ presents a comparison of the distribution of sociodemographic characteristics between the 2 groups (ACASI and face-to-face interviews, and interactive interviews and face-to-face interviews) by gender.
TABLE 1—
Sociodemographic Characteristics of Respondents Aged 15 to 19 Years, by Randomization Group: Delhi, India, 2004
| Boys (n = 583) | Girls (n = 475) | |||||
| Characteristic | ACASI and Face-to-Face Interviews | Interactive and Face-to-Face Interviews | Pa | ACASI and Face-to-Face Interviews | Interactive and Face-to-Face Interviews | Pa |
| Sample, no. | 290 | 293 | 233 | 242 | ||
| Age, y, mean (SD) | 16.8 (1.4) | 17.0 (1.5) | .8 | 16.3 (1.4) | 16.2 (1.4) | .7 |
| Enrolled in school, % | 32.4 | 31.7 | .9 | 30.0 | 35.1 | .2 |
| Ever worked, % | 71.0 | 75.1 | .3 | 50.2 | 57.4 | .1 |
| Family income, rupees,b % | .7 | .8 | ||||
| ≤ 3000 | 34.8 | 36.5 | 55.4 | 56.6 | ||
| > 3000 | 65.2 | 63.5 | 44.6 | 43.4 | ||
| Religion, % | .6 | .9 | ||||
| Hindu | 72.1 | 73.7 | 74.7 | 74.4 | ||
| Other | 27.9 | 26.3 | 25.3 | 25.6 | ||
| Area of residence, % | .5 | .3 | ||||
| Sanjay Camp | 40.7 | 41.3 | 41.6 | 33.1 | ||
| Subhash Camp | 43.8 | 46.4 | 47.2 | 55.8 | ||
| Mini Subhash Camp | 5.5 | 5.8 | 4.7 | 4.6 | ||
| Shaheed Camp | 10.0 | 6.5 | 6.4 | 6.6 | ||
Note. ACASI = audio computer-assisted self-interview.
aFrom χ2 test (categorical variables) or Bartlett’s test for equal variance (continuous variables).
b3000 rupees = $70.
Table 2 ▶ shows individual-level differences in reports of sexual behaviors and experiences by interview mode and gender. Twenty-seven percent of male participants reported in ACASIs that they had engaged in heterosexual sexual intercourse, as compared with 21% in face-to-face interviews (P = .03). Female participants reported fewer sexual behaviors in ACASIs than in face-to-face interviews. For example, 14% reported having been forcibly touched in ACASIs, as compared with 38% in face-to-face interviews (P < .001).
TABLE 2—
Individual-Level Differences in Reports of Sexual Behaviors and Experiences Among 15- to 19-Year-Olds, by Sex and Type of Interview: Delhi, India, 2004
| Boys (n = 290) | Girls (n = 233) | Boys (n = 293) | Girls (n = 242) | |||||||||
| ACASI, % | FTF, % | Pa | ACASI, % | FTF, % | Pa | Interactive, % | FTF, % | Pa | Interactive, % | FTF, % | Pa | |
| Ever interacted with opposite sex | 39.3 | 40.0 | .9 | 15.5 | 50.2 | <.001 | 44.0 | 41.6 | .4 | 50.8 | 54.5 | .2 |
| Ever had opposite-gender friendb | .2 | .04 | .003 | .09 | ||||||||
| Yes | 53.8 | 50.0 | 30.0 | 36.9 | 58.4 | 51.9 | 26.9 | 31.0 | ||||
| No | 45.9 | 50.0 | 70.0 | 63.1 | 41.6 | 48.1 | 73.1 | 69.0 | ||||
| Did not respond | 0.3 | . . . | . . . | . . . | . . . | . . . | . . . | . . . | ||||
| Ever especially liked someone from the opposite sex | 63.8 | 54.5 | <.001 | 30.9 | 38.2 | .02 | 61.1 | 54.9 | .005 | 42.1 | 35.5 | .04 |
| Ever had a casual relationship with someone from the opposite sex | 7.6 | 7.6 | 1.0 | 3.9 | 3.4 | 1.0 | 9.9 | 11.9 | .5 | 2.5 | 6.2 | .05 |
| Ever emotionally attached to someone from the opposite sex | 17.6 | 28.3 | <.001 | 6.0 | 17.2 | <.001 | 29.4 | 30.4 | .8 | 25.2 | 14.9 | <.001 |
| Ever touched someone from the opposite sex | 10.7 | 21.7 | <.001 | 1.3 | 6.0 | .003 | 22.2 | 22.9 | .8 | 4.1 | 5.8 | .4 |
| Ever had sexual intercourse with someone from the opposite sexb | .03 | .2 | .002 | .002 | ||||||||
| Yes | 26.9 | 21.4 | 3.4 | 1.3 | 28.4 | 19.5 | 7.1 | 1.7 | ||||
| No | 73.1 | 77.9 | 92.7 | 98.7 | 71.6 | 79.5 | 92.9 | 98.3 | ||||
| Did not respond | . . . | 0.01 | 3.9 | . . . | . . . | 1.0 | . . . | . . . | ||||
| Ever been forcibly touched | 26.2 | 21.4 | .09 | 14.2 | 38.4 | <.001 | 26.6 | 21.8 | .04 | 36.0 | 33.9 | .5 |
| Ever experienced an attempt at forced sexual intercourse | 11.4 | 7.9 | .10 | 2.6 | 1.3 | .5 | 12.3 | 8.5 | .03 | 1.6 | 1.6 | 1.0 |
| Ever had sexual intercourse with someone from the same sexb | 1.0 | .5 | .6 | .06 | ||||||||
| Yes | 6.2 | 6.6 | 1.4 | 0.4 | 7.8 | 6.8 | 2.1 | . . . | ||||
| No | 92.8 | 93.5 | 98.7 | 99.6 | 91.8 | 93.2 | 97.9 | 100.0 | ||||
| Did not respond | 1.0 | . . . | . . . | . . . | 0.3 | . . . | . . . | . . . | ||||
Note. ACASI = audio computer-assisted self-interview; FTF = face-to-face interview. Sample sizes varied for some subgroup comparisons.
aExact McNemar significance probabilities from matched case–control analyses.
b“No” responses and “did not respond” were collapsed to allow determination of P values.
Male participants consistently reported more behaviors and experiences in interactive interviews than in face-to-face interviews. Twenty-eight percent reported having had sexual intercourse in interactive interviews, as compared with 20% in face-to-face interviews (P = .002), and 27% reported having been forcibly touched in interactive interviews, as opposed to 22% in face-to-face interviews (P = .04). In addition, 12% of male participants reported in interactive interviews that someone had attempted to coerce them into having sexual intercourse, as compared with 9% in face-to-face interviews (P = .03). Female participants also reported sexual behaviors more often in interactive interviews than in face-to-face interviews; for instance, 7% reported having had sexual intercourse in interactive interviews, in comparison with 2% in face-to-face interviews (P = .002).
DISCUSSION
We found that participants’ reports of their sexual behaviors differed according to the interview methodology used. Both boys and girls reported more behaviors in interactive interviews than in face-to-face interviews. Because the audiovisual aids in the interactive interview materials were contextually specific and locally developed, we believe that these differences may have been because of respondents’ enhanced comprehension and comfort level with interactive interviews.
Contrary to our hypothesis, ACASIs did not uniformly lead to higher levels of reporting. There was no consistent pattern in male participants’ reports of their sexual behaviors in ACASIs and face-to-face interviews. However, female participants consistently reported fewer behaviors in ACASIs than in face-to-face interviews. It is likely that participants’ lack of exposure to computers led to apprehension in reporting behaviors in ACASIs. Although we did not specifically assess why the different interview methodologies produced differing responses, participants may have been more familiar with face-to-face interviews and may have felt more comfortable in being able to voice their concerns with an interviewer.
There were several limitations of our study and ways in which future research could better assess methodological differences. First, all of the questions included in this study were of a sensitive nature in a context of strong social norms against adolescents and young adults interacting with members of the opposite gender. Whereas our goal was to compare reporting of sensitive behaviors across different interview modes, future studies of this type should include questions on nonsensitive behaviors to provide a better perspective on methodology effects.
Second, although we included face-to-face exit interviews as part of our study, these interviews focused on young people’s overall methodology preferences. Future investigations would benefit from including a specific link between potential outcomes of interest (e.g., history of sexual intercourse) and preferred interview mode.
Third, our findings may have limited generalizability to young people living in economically disadvantaged urban areas in India. However, this is an important group to study given their limited access to reliable sources of information on reproductive health and their likelihood of engaging in high-risk behaviors. In addition, few community-based studies on young people’s sexual behaviors have been conducted in India.22,23
Fourth, the main reasons for nonparticipation were work schedule conflicts (for male participants) and lack of parental permission (for female participants). However, nonparticipation rates should not have affected the conclusions of this study because its purpose was to compare different interview methods. Also, the high response rate of 82% allows us an increased level of confidence in our findings.
In comparison with other studies assessing premarital sexual activity among young people in India, results from this study show high levels of reporting, particularly for girls in a population-based sample. Studies have typically shown that 15% to 30% of male participants and fewer than 10% of female participants report premarital sexual experience.22 We found that 28% of male participants and 7% of female participants reported having had heterosexual intercourse.
Eight percent of male participants and 2% of female participants reported having had homosexual experiences. More than one quarter of male participants (27%) and 38% of female participants reported having been touched against their will, and 12% of male participants and 3% of female participants reported that someone had attempted to force them to have sexual intercourse.23–25 Our findings underscore the need for interventions promoting sexual health among unmarried young people living in urban areas of India, given that a substantial proportion of these young people engage in premarital sexual intercourse and report nonconsensual sexual experiences that can have devastating long-term consequences.24–26
In addition, although we were unable to assess which interview method provided the most-valid responses, our findings reflect the growing evidence that use of ACASIs is not feasible in all settings. As an example, studies conducted in Kenya19 and Pune, India,20 also did not show that young people consistently provided more-accurate reports of sensitive behaviors in ACASIs than in other types of interviews.
In the context of our study setting, in which there was, in general, minimal familiarity with computers and many young people are at very low literacy levels, interactive interviews may have decreased some of the barriers associated with young people’s reports of their sexual behaviors. On the basis of our results, as well as those of other studies, future research needs to carefully consider whether ACASIs should be the “gold standard” interview methodology in settings in which people have little or no exposure to computers.
Acknowledgments
This study was funded by a Mellon grant from the Johns Hopkins University Population Center, a dissertation grant from the Bill and Melinda Gates Institute of Population and Reproductive Health, and the Woodrow Wilson–Johnson & Johnson Dissertation Fellowship in Women’s Health.
We thank Samudayik Shakti and Sampurna Trust, Delhi, India, for their collaboration, partnership, and active support throughout the data collection process. We acknowledge assistance from Geetika Software, Udaipur, India, in developing and administering audio computer-assisted self-interviews and Vikalp Design, Udaipur, India, for its assistance in developing interactive interviews. We thank the interviewers and data management team for their help. Finally, we are grateful to all of the study participants.
Human Participant Protection This study was approved by the Johns Hopkins Bloomberg School of Public Health institutional review board and a local institutional review board in India. Participants and guardians of minors provided written informed consent.
Peer Reviewed
Contributors Jaya was involved in study design, data collection, and analysis and interpretation of results. M. J. Hindin assisted with design, analysis, and interpretation and contributed to revisions of the article. S. Ahmed assisted with analysis and interpretation and contributed to revisions of the article.
References
- 1.Des Jarlais D, Paone D, Milliken J, et al. Audio-computer interviewing to measure risk behavior for HIV among injecting drug users: a quasi-randomized trial. Lancet. 1999;353:1657–1662. [DOI] [PubMed] [Google Scholar]
- 2.United Nations. World population prospects: the 2004 revision population database. Available at: http://esa.un.org/unpp/. Accessed August 1, 2005.
- 3.National Family Health Survey (NFHS-2) 1998–99. Mumbai, India: National Institute for Population Sciences; 2000.
- 4.Putting reproductive health within the wider context of adolescent lives: challenges and experiences. Paper presented at: International Conference on Adolescent Reproductive Health: Evidence and Program Implications for South Asia, November 2000, Mumbai, India.
- 5.Report of the Working Group on Adolescents for the Tenth Five Year Plan (2002–2007). New Delhi, India: Planning Commission, Government of India; 2001.
- 6.Adolescents in India: A Profile. New York, NY: United Nations Population Fund; 2000.
- 7.United Nations. At the crossroads: accelerating youth access to HIV/AIDS interventions. Available at: http://www.unfpa.org/upload/lib_pub_file/316_filename_UNFPA_Crossroads.pdf. Accessed August 5, 2005.
- 8.Gregson S, Zhuwau T, Ndlovu J, Nyamukapa CA. Methods to reduce social desirability bias in sex surveys in low-development settings: experience in Zimbabwe. Sex Transm Dis. 2002;29:568–575. [DOI] [PubMed] [Google Scholar]
- 9.Ghanem KG, Hutton HE, Zenilman JM, Zimba R, Erbelding EJ. Audio computer assisted self interview and face to face interview modes in assessing response bias among STD clinic patients. Sex Transm Infect. 2005; 81:421–425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kissinger P, Rice J, Farley T, et al. Application of computer assisted interviews to sexual behavior research. Am J Epidemiol. 1999;149:950–954. [DOI] [PubMed] [Google Scholar]
- 11.Tourangeau R. Survey research and societal change. Annu Rev Psychol. 2004;55:775–801. [DOI] [PubMed] [Google Scholar]
- 12.Turner C, Ku L, Rogers LD, Linberg LD, Pleck JH, Sonenstein FL. Adolescent sexual behavior, drug use and violence: increased reporting with computer survey technology. Science. 1998;280:867–873. [DOI] [PubMed] [Google Scholar]
- 13.Johnson A, Copas AJ, Erens B, et al. Effect of computer assisted self-interviews on reporting of sexual HIV risk behaviors in a general population sample: a methodological experiment. AIDS. 2001;15:111–115. [DOI] [PubMed] [Google Scholar]
- 14.Williams ML, Freeman RC, Bowen AM, et al. A comparison of the reliability of self-reported drug use and sexual behaviors using computer-assisted versus face-to-face interviewing. AIDS Educ Prev. 2000;12: 199–213. [PubMed] [Google Scholar]
- 15.Webb P, Zimet GD, Fortenberry D, Blythe MJ. Comparability of a computer-assisted versus written method for collecting health behavior information from adolescent patients. J Adolesc Health. 1999;24: 383–388. [DOI] [PubMed] [Google Scholar]
- 16.Wijgert J, Padian N, Shiboski S, Turner C. Is audio computer assisted self-interviewing a feasible method of surveying in Zimbabwe? Int J Epidemiol. 2000;29: 885–890. [DOI] [PubMed] [Google Scholar]
- 17.Hewett P, Mensch, B, Roeria M, et al. Using STI biomarkers to validate the reporting of sexual behavior within an experimental evaluation of interviewing methods. Paper presented at: annual meeting of the Population Association of America, March 2006, Los Angeles, Calif.
- 18.Hewett P, Mensch BS, Erulkar AS. Consistency in the reporting of sexual behavior by adolescent girls in Kenya: a comparison of interviewing methods. Sex Transm Infect. 2004;80(suppl 2):ii43–ii48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mensch B, Hewett PC, Erulkar AS. The reporting of sensitive behavior by adolescents: a methodological experiment in Kenya. Demography. 2003;40: 247–268. [DOI] [PubMed] [Google Scholar]
- 20.Potdar R, Koenig M. Does audio-CASI improve reports of risk behavior? Evidence from a randomized field trial among urban male youth in India. Stud Fam Plann. 2005;36:107–116. [DOI] [PubMed] [Google Scholar]
- 21.Schulz KF, Grimes DA. Generation of allocation sequences in randomized trials: chance, not choice. Lancet. 2002;359:515–519. [DOI] [PubMed] [Google Scholar]
- 22.Jejeebhoy S, Sebastian MP. Actions That Protect: Promoting Sexual and Reproductive Health and Choice Among Young People in India. New Delhi, India: Population Council, South and East Asia; 2003.
- 23.Jejeebhoy S. Adolescent sexual and reproductive behavior: a review of the evidence from India. Soc Sci Med. 1998;46:1275–1290. [DOI] [PubMed] [Google Scholar]
- 24.Brown A, Jejeebhoy S, Shah I, Yount KM. Sexual Relations Among Young People in Developing Countries: Evidence From WHO Case Studies. Geneva, Switzerland: World Health Organization; 2001.
- 25.Sodhi G, Verma M. Sexual coercion among unmarried adolescents of an urban slum in India. Available at: http://www.who.int/reproductive-health/publications/towards_adulthood/. Accessed October 22, 2007.
- 26.Population Council. Nonconsensual sexual experiences of young people in developing countries: a consultative meeting. Available at: http://www.popcouncil.org/pdfs/TABriefs/GFD_Brief-7_NONCONSENSUALSEX.pdf. Accessed August 15, 2005.