

Abstract
Early 20th-century cardiovascular voluntary organizations in the United States drew strength from the well-established antituberculosis movement. By midcentury, heart disease among the young and tuberculosis had declined in this country. The international fight against tuberculosis has gathered force since the 1990s. Meanwhile, support for international cardiovascular interventions has lagged behind.
We trace the divergent path of the international cardiovascular movement and suggest ways in which it could once again learn from the trials and achievements of tuberculosis control.
AT THE BEGINNING OF THE 20TH century, heart disease began to replace tuberculosis as the leading cause of death in the United States. Nascent institutions concerned with this rising threat looked to the remarkable success of voluntary tuberculosis control organizations for inspiration and support. Indeed, many of the movement’s forefathers saw heart disease control as a natural extension of the antituberculosis campaigns. These organizations did not dwell on the obvious differences between the two diseases. Rather, the future leaders of the American Heart Association (AHA) and the American College of Cardiology used the metaphor of tuberculosis as a devastating and, until the 1950s, weakly treatable chronic disease to engage public support for heart failure care and research.
By midcentury, heart disease and tuberculosis efforts enjoyed the advent of effective treatments. At the same time, the two campaigns began to diverge in the minds of public health officials and the populace. In part, changing epidemiology caused this shift; however, voluntary organizations played a large role in defining how the United States and the world should conceptualize and confront these two problems. Under their influence, cardiovascular disease came to represent an affliction of tobacco use, dietary excess, and sedentary lifestyle. Meanwhile, tuberculosis came in and out of view as a disease of the poor that was too difficult to treat in most Third World settings.
As the 21st century begins, the struggle to eliminate tuberculosis as a global killer has finally gained the support it deserves.1 Since the 2001 creation of the Global Fund to Fight AIDS, Tuberculosis, and Malaria, some have announced a new era of global health.2 Others have lamented that tuberculosis, HIV, and malaria have captured all the passion and resources of recent international health initiatives.3
Advocates for cardiovascular disease have emphasized that heart disease is the leading cause of death in developing countries and have called for cost-effective interventions to prevent heart attack and stroke.4,5 Those intent on targeting public resources to the poorest citizens in developing countries have noted that infectious diseases still account for most illness in these populations.6 Yet the established heart conditions that now affect the poorest billion persons in the world—rheumatic heart disease, cardiomyopathies, malignant hypertension—have, like tuberculosis, receded from the epidemiology—and the consciousness—of countries like the United States.
In 1993, the World Bank’s landmark development report, Investing in Health, illuminated the global burden of death and disability from both tuberculosis and cardiovascular disease. Preliminary estimates for 1990 put the fraction of disability-adjusted life years lost to these conditions at 3% and 9%, respectively, in developing countries.7 In 2006, updated disease burden models once again made clear the global importance of these problems among young adults (Table 1 ▶).8
Table 1—
Percentage of Disability-Adjusted Life Years Lost to Tuberculosis and Cardiovascular Disease (CVD) in Sub-Saharan Africa and other Low- and Middle-Income Countries: 2001
| Sub-Saharan Africa, % | Low- and Middle-Income Countries, % | |||
| All Ages | 15–44 y | All Ages | 15–44 y | |
| Tuberculosis | 2.3 | 1.4 | 2.6 | 1.3 |
| Ischemic CVD | 1.3 | 0.1 | 5.2 | 0.6 |
| Noncoronary CVD | 3.3 | 0.9 | 7.9 | 1.1 |
| Total CVD | 4.6 | 1.0 | 13.0 | 1.7 |
Source. Reference 8.
Note. Low income and middle income was defined as per capita yearly income of $905 or less and $906 to $11 115, respectively, as determined by 2006 gross national income.
Activists can probably remember, however, the neglect of both cardiovascular disease and tuberculosis only a decade ago. Whereas investment in global tuberculosis programs grew by more than 10 times during the 1990s alone, global cardiovascular interventions have stagnated.9,10 In 2007, despite continued challenges of drug-resistance and HIV co-infection, the World Health Organization announced that the global tuberculosis epidemic had stabilized.11
As it did a century ago, the success of the antituberculosis movement has lessons for cardiovascular disease and global health equity.
HISTORICAL TIES IN THE UNITED STATES
Tuberculosis and cardiovascular disease represent different categories of illness—a single pathogen that affects multiple organs in one case, damage to one organ system from a range of insults in the other. It comes as a surprise, then, that a movement to control cardiovascular disease saw its model in tuberculosis advocacy.
All efforts to label pathologies both reveal and conceal the biosocial mechanisms of disease.12 At the same time, these labels create targets for intervention and advocacy. Vital statistics—first assembled by local governments and nation-states and later through the World Health Organization—have elided the analytic distinction between tuberculosis and heart disease. Despite the many pathways to cardiovascular injury, interventions for the established disease rely on a common set of technologies.
The heart disease movement in the United States drew material and moral support from tuberculosis associations through the 1940s. For much of this period, the lack of curative therapies for both of these conditions led to a focus on research and long-term care of the chronically ill. By the 1950s, the introduction of antituberculosis chemotherapy on the one hand and the mass production of penicillin and antihypertensive medications on the other led to the near-elimination of tuberculosis and heart disease mortality among young adults.
FIGHTING TUBERCULOSIS, FIGHTING HEART DISEASE
Robert Koch’s 1882 discovery of Mycobacterium tuberculosis inspired the creation of the first disease-specific voluntary (or nongovernmental) organization in the United States. Founded in 1904, forty years before the isolation of streptomycin, the National Tuberculosis Association (NTA) sought to raise the standard of care for tuberculosis patients throughout the country.13
To counter skepticism about the impact of intervention on the ongoing decline of tuberculosis mortality, the NTA launched Framingham Community Health and Tuberculosis Demonstration project in Framingham, Mass, with the support of the Metropolitan Life Insurance Company.14 Although less famous than the Framingham Heart Study that would follow more than 30 years later, the demonstration project was a success. Between 1916 and 1923, the study contributed to a 68% decline in tuberculosis mortality in Framingham.13
In 1910, “diseases of the heart” replaced tuberculosis as the official leading cause of death in the United States.15 This ill-defined group of conditions owed its new-found stature, in part, to the decline in tuberculosis deaths.16 By 1915, Lewis Connor, a New York internist, had led the New York Academy of Medicine in the creation of the Association for the Relief and Prevention of Heart Disease in New York City (later referred to simply as the New York Heart Association).17 As cardiology began to emerge as a specialty, the field’s own voluntary and professional organizations took the model of tuberculosis control as their template. With little treatment to offer beyond nitroglycerine, mercurial diuretics, Southey’s tubes, and digitalis, Connor and his colleagues focused on extending tuberculosis-style rehabilitation services to patients with heart failure.18 Of the seven original aims of the New York Heart Association, three concerned research and four involved vocational and convalescent services.17 Its now famous classification scale of heart failure symptoms aimed in part to encourage convalescent or nursing homes to admit cardiac patients thought too sick to rehabilitate.
The early founders of heart disease organizations were explicit in their emulation of tuberculosis control efforts. Haven Emerson, one of the founders of the AHA, had worked under the tuberculosis pioneer Herman Biggs before succeeding him as commissioner of New York City’s health department.19 Writing in a publication of the Michigan Tuberculosis Association, Emerson described heart disease control as a natural extension of the tuberculosis movement:
At every point of prevention and treatment, the same diagnostic chest clinic, occasional hospital care, social and nursing follow-up in the home, educational service and occupational guidance and placement are needed as have been found indispensable in the tuberculosis campaign. . . . With heart experts to supplement the tuberculosis specialists, the whole machinery of tuberculosis societies and public institutions can be made immediately available for heart patients.20(p21)
An editorial in the Michigan Tuberculosis Association publication went on to predict,
In many ways the fight against heart disease will be similar to the war now waged against tuberculosis. . . . The American Heart Association is young in years, but its members are many of them old in experience, in fighting both heart disease and tuberculosis. With lessons of other campaigns to guide them, their attack on heart disease should be swift and sure.21(p2)
In fact, the burgeoning heart disease movement gleaned more than its model of chronic disease control from the tuberculosis campaigns. In 1926, the New York Tuberculosis Association absorbed the New York Heart Association physically and financially; in 1928, it published the first edition of the now famous New York heart failure classification system in its tuberculosis journal.22 The New York Heart Association would not have its own offices again until 1945.
At the same time, in 1926, the NTA likewise extended an invitation to the AHA to share in its funds and office space. The decline in tuberculosis mortality and the success of its Christmas Seals campaign had left the NTA with a surplus, of which the AHA was one of the main beneficiaries.13 Indeed, the NTA provided most of the AHA’s budget and kept the organization alive through the Depression. The AHA even considered a merger with the NTA during the early 1950s.
In 1948, the US Public Health Service decided to do something about coronary artery disease. It looked to the Framingham Tuberculosis Demonstration for direction.23 In the same year, hearings on the creation of a National Heart Institute (NHI) would cite a poll finding that 83% of Americans thought that Congress “should put aside $100 million to be used in research on tuberculosis and disease of the heart and arteries.”24(p15) The NHI, with the advice of the Boston cardiologist Paul Dudley White, took over direction of the Framingham project. However, in a divergence from the tuberculosis model, the NHI would steer the Framingham Heart Project toward research rather than disease control.
DECLINE IN TUBERCULOSIS AND CARDIOVASCULAR MORTALITY
Mortality from tuberculosis had begun to fall in many countries before the discovery of effective chemotherapy.25 Debate continues about the determinants of this decline.26 To some extent, US voluntary organizations for the control of tuberculosis took credit for epidemiological trends driven by larger social forces.27 By 1973, tuberculosis mortality had fallen to 1.5 per 100 000 persons, down from 194 per 100 000 persons in 1900. Not until the 1980s would an outbreak of multidrug-resistant tuberculosis in New York City bring the disease to the country’s—and the world’s—attention again.28
Although the total death rate from heart disease in the United States did not begin to decline until the 1960s, mortality from these conditions among young adults fell much earlier. This trend mirrored the decline of tuberculosis during this period (Figure 1 ▶).
FIGURE 1—
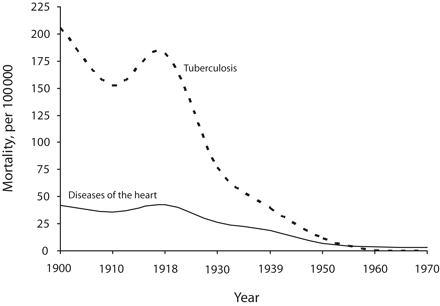
Mortality from heart disease and tuberculosis among people aged 15 to 24 years: United States, 1900–1970.
Source. National Center for Health Statistics.29
In his autobiography, Paul Dudley White described penicillin as one of the early breakthroughs in cardiology.30 By the 1950s, the availability of penicillin made endocarditis and syphilitic aortitis treatable diseases.31 Mortality from rheumatic heart disease, which had preoccupied the founders of the New York Heart Association, and from rheumatic fever, which had driven White into cardiology (it had killed his sister), continued to decline following the wide use of this antibiotic.32
In the case of both tuberculosis and heart disease, the United States entered a period after the 1950s in which economic progress reinforced the benefits of new technologies and knowledge. The emergence of multidrug regimens for hypertension and heart failure mirrored the development of short-course chemotherapy for tuberculosis.33 Reserpine and chlorthiazide had already provided effective and safe hypertension treatment by the late 1950s.23,34 Beta blockers and calcium channel blockers made greater reductions in blood pressure possible in the 1960s.35 The Framingham Heart Study reported the virtual eradication of malignant hypertension by the 1970s.36 By 1960, only 0.8% of the men in the Framingham cohort had severe hypertension (defined as greater than 210/120 mm Hg) compared with 1.8% a decade earlier.
The introduction of loop diuretics in the 1960s resulted in approximately a 70% reduction in the short-term risk of death for patients with heart failure.37 With the decline of rheumatic fever and hypertension, heart failure in the United States increasingly became a disease among elderly persons with coronary disease. The average age at heart failure diagnosis in the Framingham study rose from 57 in the 1950s to 76 in the 1980s.38 Coronary disease, which had caused 22% of heart failure cases in the 1950s, accounted for 67% of cases in the same cohort by the 1980s. By 1991, more than 4 of 5 heart failure cases in Olmsted County, Minn, were older than 65 years and almost half were over 80.39
By the 1960s, mortality from coronary disease had begun to decline as well, in part because of awareness of the risk factors identified in Framingham—tobacco in particular—and because of the treatment of hypertension and management of myocardial infarction in coronary care units.40 The decline in coronary mortality continued into the 1980s and 1990s with antiplatelet, fibrinolytic, and percutaneous therapies for acute myocardial infarction.41
DIVERGENT PATHS IN TUBERCULOSIS AND CARDIOVASCULAR CONTROL
Neither the tuberculosis nor the heart disease movements quickly extended their efforts to developing countries, but for different reasons. Tuberculosis had become a disease of poor nations, and its treatment was complex. The failures of cheap but ineffective control efforts discouraged much progress until the 1990s. By contrast, the rise of coronary disease in wealthy nations focused cardiovascular epidemiology on atherosclerosis; other causes of heart failure, by then increasingly rare in the developed world, began to drop from the heart disease movement’s attention. This notion of heart disease as a problem of rich countries, as well as alarm over the cost of cardiac care, limited the international heart movement to calls for prevention. Ironically, as tuberculosis initiatives at the end of the century would show, voluntary disease control movements had the greatest potential in the poorest socioeconomic substrate.
TUBERCULOSIS IN LOW-INCOME COUNTRIES
The threat of tuberculosis had almost vanished from view in most wealthy countries by the 1970s. Many of these countries began to dismantle their control programs—in some cases prematurely.42 In most of Africa, Asia, and Latin America—and in pockets within high-income countries, such as New York City’s Harlem—tuberculosis continued to spread in areas with incomplete or absent treatment programs.
The International Union Against Tuberculosis (IUAT) first convened in Paris in 1920.43 At first, its small budget was only enough to support a few scientific conferences and a bulletin. By the end of the century, however, the union’s model of tuberculosis control would set the standard for developing countries.
By the 1960s, the availability of multidrug regimens had made it technically possible to cure tuberculosis in 12 months. The cost and complexity of long-course tuberculosis treatment meant, however, that except in a handful of low-income countries, few national tuberculosis programs had developed outside Europe and the United States. According to the IUAT’s director of scientific activities, Donald Enarson, the IUAT and the World Health Organization, misled by faulty transmission models, encouraged countries to begin nationwide isoniazid monotherapy.44 This strategy ultimately led to poor treatment outcomes and, in some regions, to isoniazid resistance as well. By the beginning of the 1970s, the World Health Organization had all but declared the defeat of this approach, encouraging developing countries to put aside tuberculosis interventions until they had first established primary health care systems.
By the late 1970s, however, the IUAT, now led by the Czechoslovakian Karel Styblo, had reignited the strategy of vertical tuberculosis control. In 1977, the IUAT collaborative program had piloted a 12-month treatment regimen in Tanzania. The poor results convinced Styblo to use more-expensive rifampin- and pyrazinamide-containing regimens to shorten the course to 8 months. The new program, which focused on effective treatment of highly transmissible smear-positive cases, increased cure rates from 52% to 80%. During the 1980s, the IUAT—later renamed the International Union Against Tuberculosis and Lung Disease (IUATLD)—expanded its new model to other countries in Africa, Latin America, and the Middle East.43
GLOBAL TUBERCULOSIS CONTROL DURING THE 1990S
The success of the union’s model won the support of the World Bank, whose project for disease control priorities called tuberculosis control one of the three most cost-effective interventions it had evaluated.45 In 1991, WHO adopted the IUATLD model and called for a 70% detection rate and an 85% cure rate worldwide for patients with the most contagious forms of tuberculosis by the year 2000.46
WHO’s Mario Raviglione has described the growth in external financing for tuberculosis control during the 1990s.9 Under the banner of the IUATLD model—now called DOTS (Directly Observed Therapy Short Course)—between 1990 and 2000, overseas development assistance for tuberculosis increased from $16 million to $190 million. During the same period, the WHO tuberculosis unit grew from a two-officer program to a large “Stop TB” partnership.
Inadequate tuberculosis control resources, however, continued to sidetrack control strategies during this period. Even as the problem of multidrug-resistant disease became apparent, WHO refused to endorse costly treatment of multidrug-resistant patients in developing countries until the late 1990s.1 Once WHO agreed on the need for treatment, negotiated drug purchases led to a decline in treatment cost of more than 90%.47
Following the 2001 report of the Commission on Macroeconomics and Health and the emergence of the Global Fund to Fight AIDS, Tuberculosis, and Malaria, financing for tuberculosis in low-income countries continued to grow.48 By 2004, WHO had reported that over half of new smear-positive tuberculosis cases in the world received treatment under a DOTS program, with cure rates higher than 80%.15
In a 2003 interview with the authors, Stop TB’s Leopold Blanc described the shift in perspective that made such progress possible: “Countries . . . need to think about what they have to do to reach their target—not what they can do with the money they have. . . . Control is not done with funds in mind. You always have to think about needs.”
INTERNATIONAL CARDIOLOGY FROM THE 1950S TO THE 1980S
During the late 19th and early 20th centuries, health interventions by colonial governments had focused initially on epidemics that were a danger to European administrators and settlers.49 The health of the native population received attention only when infectious disease and death during childbirth threatened to upset economic productivity.50 Cardiovascular conditions were thus not a concern to authorities in much of Asia and Africa until the post-independence period.51 Early cardiovascular epidemiologists had also emphasized the relative absence of heart disease in these populations.
In a 1929 Lancet paper on blood pressure among 1000 rural Kenyan men, C.P. Donnison wrote that during his two years near Lake Victoria he had observed little cardiac pathology:
The results of this investigation thus lend support to the view that hyperpiesia and arteriosclerosis are diseases associated with civilization. . . . I think almost everybody who has been closely associated with the African native will agree that he very rarely can be described as living a high pressure existence.52(p7)
Also, reviews on rheumatic fever and rheumatic heart disease at first reported these conditions as uncommon outside temperate countries. In a 1915 analysis for the Lancet, J.P. Clarke wrote,
there is no rheumatic fever and no rheumatoid arthritis in the Malay Peninsula, and I shall produce some figures which will show that it is extremely probable that neither of these diseases occurs in any part of the tropics.53(p1169)
Fed by limited and conflicting autopsy and clinical reports, the impression of cardiovascular disease in Africa, Asia, and Latin America evolved during the 1940s.54–56 By World War II, the importance of heart disease in these regions had come into greater focus.57 By the late 1950s, hospital series showed that heart failure claimed a significant proportion of admissions even in sub-Saharan Africa (Table 2 ▶).58
Table 2—
Fraction of Medical Admissions Because of Heart Failure Reported in Sub-Saharan Africa and in Asia: 1951–1969
| Author | Year | Country | City or Region | Heart Failure Cases, No., (%) |
| Beet (1956)58 | 1951–1955 | Nigeria | Jos and Katsina | 2700 (7) |
| Obineche (1976)59 | 1969 | Angola | Lusaka | 170 (11) |
| Rowland (1965)60 | 1961–1962 | Sierra Leone | Freetown | 224 (12) |
| Alimurung et al. (1955)54 | 1947–1953 | Philippines | Manila | 4304 (14) |
| Mathur (1960)61 | 1946–1957 | India | Agra | 2145 (8) |
| Vakil (1962)62 | 1946–1955 | India | Bombay | 6825 (7) |
In 1960, White sent two of his colleagues, David Miller and Steven Spencer, to Albert Schweitzer’s clinic in Lambaréné, Gabon, for 6 months. White had met Schweitzer during a tour of Africa in 1959, and the two met again briefly in France later that year. In 1962, Miller, Spencer, and White published a survey of cardiovascular disease at the Schweitzer hospital and surrounding villages in the American Journal of Cardiology.63 “To discover . . . that three quarters of the inpatients and outpatients at this famous hospital have definite evidence of one or more cardiovascular diseases was indeed unexpected,”63(p432) they wrote. Although many of these patients had only incidental electrographic abnormalities, at least 7% had overt heart failure, 12% had rheumatic heart disease, and 7% had hypertension or hypertensive heart disease. To conclude their report, White et al. called for action:
The high prevalence of mitral stenosis is astonishing. With our present knowledge of the cause and surgical relief of rheumatic heart disease, we believe strongly that it is a duty to help bring to these sufferers the benefits of better penicillin prophylaxis and of cardiac surgery when indicated. The same responsibility exists for those with correctable congenital cardiovascular defects. . . . We hope, however, that this report may increase the reader’s awareness of our opportunity and obligation to share more generously the life-saving measures of modern medical science with those elsewhere who need so much and have so little [italics in original].63(p445)
This impassioned call for action, however, seemed to have little impact on an audience preoccupied by the First World’s rising problem of coronary disease. Indeed, the International Society of Cardiology, of which White was co-founder, had heralded this shift in focus away from the heart diseases caused by pestilence and famine at its second meeting in 1954, six years before White published an account of his African travels.64 Conference chairman Ancel Keys outlined the new agenda:
Lately, the antibiotics have given us a great tool for control of heart disease resulting from infection. So much cannot be said for the kinds of heart disease that are, so to speak, self-generating. . . . Basically the question is this: What are the differences between populations who differ in their burden of coronary and other degenerative heart disease?65(p7)
In one of only two presentations from Africa—out of a total of 16 talks—the South African John Higginson adduced evidence that, compared with the population of Denmark (where early research on atherosclerosis was conducted), the Bantus had low prevalence of atherosclerosis, which correlated with low serum cholesterol levels and a low-fat diet.66
With the false notion of the heart-healthy native alive and well, the model of a transition from infectious diseases of poverty to degenerative diseases of affluence increasingly came to frame the problem of heart disease in the Third World.67 Some initiatives, such as penicillin prophylaxis for rheumatic heart disease, continued—albeit at a limited level—through this period.68 However, many efforts in the developing world were not aimed at control of heart disease but rather at explaining what protected those populations from acquiring the atherosclerotic pathologies common in Europe and North America.
In his 1974 introduction to a volume on tropical cardiology, Zdenek Fejfar made clear the WHO cardiovascular unit’s focus on coronary disease and risk factors, with an emphasis on research and prevention rather than treatment in the developing world.69(p1) He wrote,
Ischemic heart disease with coronary atherosclerosis as the underlying cause, is associated with affluence in the industrialized, socio-economically advanced society. In the so-called developing world the growth of a similar type of society is increasing the menace of ischemic heart disease becoming the world’s largest epidemic of this century, unless we can find a way of controlling and reversing the present trend.69
Fejfar went on to outline WHO’s pilot programs for hypertension in Belgium, Finland, France, Israel, Italy, Japan, Mongolia, and the Soviet Union. In his view, WHO-supported research on conditions such as Chagas’ disease and endomyocardial fibrosis found utility, in part, in their potential to contribute to advances in ischemia.
From the 1960s to the 1980s, leaders in West and East Africa fought to put nonischemic cardiovascular diseases on the global agenda.70 Figures like J.O.M. Pobee in Ghana, Paul D’Arbela in Uganda, Hilary Ojiambo in Kenya, and William Makene in Tanzania had recognized the importance of congenital and rheumatic disease, hypertension, and cardiomyopathies in their countries.71–74 These voices were drowned out by harsh social policy and—in Uganda at least—by civil strife.
Lack of funds for heart disease prevention and treatment in the Third World mirrored a lack of donor enthusiasm.74 Indeed, the International Society of Cardiology (later the World Heart Federation) never had a large amount of funding. Even with its minimal activities, the organization’s budget often ran into the red, at times surviving only with support from the AHA.76
By the end of his career, White himself appeared to change focus, devoting much of his energies to the establishment of new heart foundations and cardiovascular societies in Asia, Africa, and the Americas. In these endeavors, he seemed as interested in cold war peace-making efforts as in promoting public health intervention.
Meanwhile, the understanding of coronary disease epidemiology and treatment in the developed world made great strides. Between 1958 and 1970, Keys and his colleagues at the University of Minnesota would go on to carry out the Seven Countries comparison of coronary risk factors in the United States, Finland, the Netherlands, Italy, Yugoslavia, Greece, and Japan.77 The study showed the importance of cholesterol in the population distribution of coronary artery disease. In 1978, convincing evidence emerged that mortality from coronary heart disease had been declining in the United States and Europe since the late 1960s.23 This revelation prompted WHO to undertake an unprecedented 26-country study to monitor trends in coronary artery disease and stroke.78 The Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA) project found that between the mid-1980s and the 1990s, improvements in coronary care accounted for as much as 61% of the decline in case fatality and 52% of the decline in coronary events.79 During this same period, the climate of austerity enforced by international lenders limited the scale of international health development for tuberculosis and cardiovascular disease alike.80
INTERNATIONAL CARDIOLOGY IN THE 1990S
During the 1990s, while tuberculosis rose to disease priority status, cardiovascular control efforts continued to lag. During this period, probably no other institution had a bigger impact on international health policy and financing than the World Bank.81 In 1993, the World Bank’s development report, Investing in Health, released preliminary results of a new Global Burden of Disease study.7 Among other surprising findings, the report highlighted the epidemiological significance of both tuberculosis and cardiovascular disease in developing countries.
Whereas the light shed on tuberculosis led to a decade of growth in overseas development assistance for treatment of this disease, the focus of cardiovascular policy turned largely to prevention. Meanwhile, only a trickle of international assistance went to cardiovascular disease control. For example, Yach et al. found that by 2002, only 0.1% of the $2.9 billion in global aid for overseas health sector development went to chronic diseases of any kind.82 The same review found that only 2.5% of World Bank loans over a five-year period focused on these conditions.
The lack of an aggressive response to cardiovascular disease in developing countries during the 1990s likely stemmed from two sources. First, inadequate public resources limited health services to a fraction of national needs. External financing to fill the gaps in spending focused on priorities that often excluded cardiovascular interventions. Second, a concern to target programs at the poorest may have led to a preference for communicable disease initiatives. In this setting, reviews of cardiovascular disease in developing countries emphasized projections of vascular epidemics and counseled policy interventions for behavior change. Few called for treatment of established rheumatic disease, hypertension, and heart failure in sub-Saharan Africa or vascular events in Eastern Europe, Asia, and Latin America.
In an attempt to shift away from haphazard priority setting, the World Bank urged countries to rely on cost-effectiveness analysis. As early as 1993, the bank’s disease control priorities project found antianginal drugs, aspirin for heart attacks, secondary prophylaxis, and even valve surgery for rheumatic heart disease potentially attractive.83 But these preliminary estimates argued against pharmacotherapy for undifferentiated hypertension and hyperlipidemia or for thrombolysis in most developing country settings. Compared with tuberculosis chemotherapy at $3 per disability-adjusted life year saved, even penicillin to prevent recurrence of rheumatic fever at $100 to $200 per disability-adjusted life year saved looked like a relatively bad investment.
A companion volume to the 1993 development report concluded that, in that era before highly active antiretroviral therapy,
medical management of hypertension (US $2000), medical management of hyper-cholesterolemia (US $4000), antiviral therapy for acquired immuno-deficiency syndrome (AIDS) (US $5000), and coronary artery bypass surgery (US $5000) are all immensely unattractive investments for public funds. Furthermore, these four conditions can be effectively and economically reduced by primary prevention involving behavioral and dietary practices. This is a short list of some of the more obvious examples of technologies for which government spending should be discouraged. There are others.”84(p273)
One philosophy of targeting, best articulated by the World Bank’s Davidson Gwatkin, argued that because communicable disease affected the poor out of proportion to the rich, governments in low- and middle-income countries should focus on these diseases rather than on noncommunicable threats.6
In 1996, Christopher Murray and Alan Lopez reported 30-year global burden of disease projections in the journal Science.85 The study predicted that coronary heart disease and stroke—6.2% of disease burden globally in 1990—would account for 10% of this burden in developing countries by 2020. The report led to a series of articles in scientific journals that called for action to prevent the coming cardiovascular plague, culminating with the World Heart Federation’s 1999 white book, Impending Global Pandemic of Cardiovascular Diseases.86
The organizations created during the 1990s to carry the banner of cardiovascular crisis, most notably the International Heart Health Society, founded in 1992, continued to emphasize the importance of prevention over treatment. These groups saw the use of technology to treat established disease as a dangerous model to export from the United States and Europe to developing countries.87 The focus on behavioral prevention of vascular risk was inspired by Geoffrey Rose’s 1985 call for communitywide disease interventions and Finland’s battle to reduce dietary fat during the 1970s.88,89
The 1998 US Institute of Medicine report on control of cardiovascular disease in developing countries echoed the concerns of the World Bank and others who argued that
The only rational approach to [cardiovascular disease] prevention in all countries is one that gives the greatest priority to population-based primary prevention. Where resources are scarce . . . this strategy should be the only one adopted.90(p987)
Although the Institute of Medicine encouraged research on multidrug vascular risk packages, the predominant sentiment supported behavioral strategies.91(p41)
The Committee for Control of Cardiovascular Disease in Developing Countries wrote,
The demands on governments worldwide for inappropriate curative services may be due, in part, to a lack of information about what is cost-effective. The emphasis on treatment over prevention results in health care systems being oriented to expensive technologies for diagnosis and treatment of heart disease, rather than to community and medical education programs to reduce the risk of [cardiovascular disease]. Transferring the Western paradigm of health care will place unrealistic burdens on health care systems with extremely limited resources.91
Even in its recommendations for the former Soviet Union, where men’s life expectancy dropped by 6 years during the 1990s—in large part because of death from cardiovascular disease—a 1997 report from the US National Research Council focused on alcohol, tobacco, and diet as more efficient targets than health system interventions.92
LESSONS FROM TUBERCULOSIS CONTROL
Between 2001 and 2006, international resources for health in developing countries almost doubled.93 In 2004, a report from Columbia University’s Earth Institute, A Race Against Time, protested that “the great contemporary communicable diseases—HIV/AIDS, but also tuberculosis and malaria . . . have captured virtually all the attention and money devoted to international health problems.”3(p14) Others have argued that HIV initiatives can strengthen health system capacity to provide primary care.94
At this turning point in global health history, international cardiovascular initiatives should take stock of three lessons from the new era of tuberculosis control.5,95
First, effective demonstration projects formed the foundation of the expansion of tuberculosis control programs during the 1990s. Use of inadequate regimens had sullied the reputation of tuberculosis interventions prior to the 1980s, when the IUATLD began to promote a more expensive, but also more effective, strategy.
For some cardiovascular conditions, pilot projects have already demonstrated effectiveness and feasibility in resource-poor settings. WHO’s support for secondary prophylaxis for rheumatic fever has yielded successful programs in Africa, Asia, and Latin America. Cuba has achieved hypertension treatment and control rates several times higher than those of Western European countries.96 In the realm of acute coronary syndrome and heart failure management, however, few high-profile models have surfaced in resource-poor settings. A recent review of countrywide successes in international health did not identify a single cardiovascular example.97
Second, although economic evaluation of tuberculosis programs helped to attract the attention of the World Bank in the early 1990s, false assumptions about the economics of epidemic control also stalled implementation of interventions for drug-resistant tuberculosis at the end of the decade. The breakthrough in international tuberculosis control during the late 1990s came in part through a shift from optimization within budget constraints to target-based strategies driven by moral imperatives.47,98
Third, to take tuberculosis interventions to scale has required external financing in low-income countries. During the 1990s, this financing often came from the World Bank. Since 2001, new mechanisms for global health delivery have begun to develop in the context of priority initiatives. Funding to establish rheumatic heart disease, heart failure, and hypertension services to scale in sub-Saharan Africa may not come, however, from vertical cardiovascular programs.
In the case of tuberculosis, vertical programs generated the possibility of treatment in the absence of strong health systems. The socioeconomic context that shifted the focus of international health in the 1980s and 1990s away from primary health care to selective interventions has undoubtedly restricted the delivery of necessary services.99 The lack of public financing for the spectrum of cardiovascular disorders in most middle-and low-income countries represents one aspect of this phenomenon. Recently, however, resources for vertical interventions such as those that target tuberculosis, HIV, and malaria have begun to help rebuild primary care.100 Some have called this a diagonal approach.101 This process may offer an opportunity for the development of cardiovascular programs as one aspect of health system strengthening in some of the poorest countries.
Figure 2.
Paul Dudley and Albert Schweitzer in Alsace, France, 1958.
Source. Reprinted with permission by the Albert Schweitzer Fellowship.
Acknowledgments
We thank the John D. and Catherine T. MacArthur Foundation, whose research and writing grant from the Program on Global Security and Sustainability made this project possible. The Division of Cardiology at the Beth Israel Deaconess Medical Center, Boston, Mass, and the Institute for Global Health at the University of California, San Francisco, provided institutional support for G. Bukhman during the writing of this article.
We also thank Allan Brandt and 2 anonymous reviewers for their comments at an earlier stage.
Peer Reviewed
Contributors G. Bukhman conceptualized the study and wrote the initial draft. Both authors contributed equally to the research and writing.
References
- 1.Kim JY, Mukherjee JS, Rich ML, Mate K, Bayona J, Becerra MC. From multidrug-resistant tuberculosis to DOTS expansion and beyond: making the most of a paradigm shift. Tuberculosis. 2003;83(1–3):59–65. [DOI] [PubMed] [Google Scholar]
- 2.Cohen J. Global health. The new world of global health. Science. 2006;311:162–167. [DOI] [PubMed] [Google Scholar]
- 3.Leeder S, Raymond S, Greenberg H. A Race Against Time: The Challenge of Cardiovascular Disease in Developing Economies. New York, NY: Center for Global Health and Economic Development, Columbia University; 2004.
- 4.Lopez AD, Disease Control Priorities Project. Global Burden of Disease and Risk Factors. New York, NY: Oxford University Press; 2006.
- 5.Levy D, Brink S. A Change of Heart: How the Framingham Heart Study Helped Unravel the Mysteries of Cardiovascular Disease. 1st ed. New York, NY: Knopf; 2005.
- 6.Gwatkin DR, Guillot M, Heuveline P. The burden of disease among the global poor. Lancet. 1999;354:586–589. [DOI] [PubMed] [Google Scholar]
- 7.World Bank. World Development Report: Investing in Health. Washington, DC: Oxford University Press; 1993.
- 8.Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL. Disease Control Priorities Project. Global Burden of Disease and Risk Factors. New York, NY: Oxford University Press; 2006.
- 9.Raviglione MC, Pio A. Evolution of WHO policies for tuberculosis control, 1948–2001. Lancet. 2002;359:775–780. [DOI] [PubMed] [Google Scholar]
- 10.Yach D. Partnering for better lung health: improving tobacco and tuberculosis control. Int J Tuberc Lung Dis. 2000; 4:693–697. [PubMed] [Google Scholar]
- 11.Global Tuberculosis Control: Surveillance, Planning, Financing. Geneva, Switzerland: World Health Organization; 2007.
- 12.Krieger N. Epidemiology and the web of causation: has anyone seen the spider? Soc Sci Med. 1994;39:887–903. [DOI] [PubMed] [Google Scholar]
- 13.Shryock RH. National Tuberculosis Association, 1904–1954: A study of the Voluntary Health Movement in the United States. New York, NY: Arno Press; 1977.
- 14.Armstrong DB. The medical aspects of the Framingham Community Health and Tuberculosis Demonstration. Int J Epidemiol. 2005;34(6):1183–1187. [DOI] [PubMed] [Google Scholar]
- 15.Hilbrich L, Sleight P. Progress and problems for randomized clinical trials: from streptomycin to the era of megatrials. Eur Heart J. 2006;27:2158–2164. [DOI] [PubMed] [Google Scholar]
- 16.Carter KC. Causes of disease and causes of death. Contin Chang. 1997;12: 189–198. [Google Scholar]
- 17.De la Chapelle CE. The New York Heart Association, Origins and Development, 1915–1965. New York, NY: New York Heart Association; 1966.
- 18.Ventura HO, Mehra MR. Bloodletting as a cure for dropsy: heart failure down the ages. J Card Fail. 2005;11:247–252. [DOI] [PubMed] [Google Scholar]
- 19.Frieden TR, Lerner BH, Rutherford BR. Lessons from the 1800s: tuberculosis control in the new millennium. Lancet. 2000;355:1088–1092. [DOI] [PubMed] [Google Scholar]
- 20.Emerson H. Cited in: Am Heart Assoc Bull. 1925;1(1). Quoted in: Moore WW. Fighting for Life: The Story of the American Heart Association, 1911–1975. 1st ed. Dallas, Tex: American Heart Association; 1983.
- 21.Michigan Tuberculosis Association, editorial commentary. Cited in: Am Heart Assoc Bull. 1925;1(1):2. Quoted in: Moore WW. Fighting for Life: The Story of the American Heart Association, 1911–1975. 1st ed. Dallas, Tex: American Heart Association; 1983. [Google Scholar]
- 22.Pardee HEB, New York Tuberculosis and Health Association. Criteria for the Classification & Diagnosis of Heart Disease. New York, NY: P.B. Hoeber Inc; 1928.
- 23.Kannel WB, Levy D. Commentary: medical aspects of the Framingham Community Health and Tuberculosis Demonstration. Int J Epidemiol. 2005;34(6):1187–1188. [DOI] [PubMed] [Google Scholar]
- 24.National Heart Lung and Blood Institute. A Salute to the Past. Washington, DC: National Institutes of Health; 1987.
- 25.Murray JF. A Century of tuberculosis. Am J Respir Crit Care Med. 2004;169(11):1181–1186. [DOI] [PubMed] [Google Scholar]
- 26.Fairchild AL, Oppenheimer GM. Public health nihilism vs pragmatism: history, politics, and the control of tuberculosis. Am J Public Health. 1998;88:1105–1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bates B. Bargaining for Life: A Social History of Tuberculosis, 1876–1938. Philadelphia: University of Pennsylvania Press; 1992.
- 28.Bloom BR, Murray CJ. Tuberculosis: commentary on a reemergent killer. Science. 1992;257:1055–1064. [DOI] [PubMed] [Google Scholar]
- 29.Centers for Disease Control and Prevention. Mortality data from the National Vital Statistics System. Available at: http://www.cdc.gov/nchs/deaths.htm. Accessed April 7, 2007.
- 30.White PD. My Life and Medicine: An Autobiographical Memoir. Boston, Mass: Gambit; 1971.
- 31.Lerner PI. Producing penicillin. N Engl J Med. 2004;351:524. [DOI] [PubMed] [Google Scholar]
- 32.Gordis L. The virtual disappearance of rheumatic fever in the United States: lessons in the rise and fall of disease. T. Duckett Jones memorial lecture. Circulation. 1985;72:1155–1162. [DOI] [PubMed] [Google Scholar]
- 33.Cleland JG, Clark AL. Delivering the cumulative benefits of triple therapy to improve outcomes in heart failure: too many cooks will spoil the broth. J Am Coll Cardiol. 2003;42:1234–1237. [DOI] [PubMed] [Google Scholar]
- 34.Vakil RJ. Rauwolfia serpentina in the treatment of high blood pressure: a review of the literature. Circulation. 1955;12:220–229. [DOI] [PubMed] [Google Scholar]
- 35.Moser M. Historical perspective on the management of hypertension. Am J Med. 1986;80(5B):1–11. [DOI] [PubMed] [Google Scholar]
- 36.Cowie MR, Mosterd A, Wood DA, et al. The epidemiology of heart failure. Eur Heart J. 1997;18:208–225. [DOI] [PubMed] [Google Scholar]
- 37.Faris R, Flather MD, Purcell H, Poole-Wilson PA, Coats AJ. Diuretics for heart failure. Cochrane Database Syst Rev. 2006;1:CD003838. [DOI] [PubMed] [Google Scholar]
- 38.Freudenberg N, Fahs M, Galea S, Greenberg A. The impact of New York City’s 1975 fiscal crisis on the tuberculosis, HIV, and homicide syndemic. Am J Public Health. 2006;96:424–434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: a study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation. 1998;98:2282–2289. [DOI] [PubMed] [Google Scholar]
- 40.Goldman L, Cook EF. The decline in ischemic heart disease mortality rates: an analysis of the comparative effects of medical interventions and changes in lifestyle. Ann Intern Med. 1984;101:825–836. [DOI] [PubMed] [Google Scholar]
- 41.Hunink MG, Goldman L, Tosteson AN, et al. The recent decline in mortality from coronary heart disease, 1980–1990: the effect of secular trends in risk factors and treatment. JAMA. 1997;277:535–542. [PubMed] [Google Scholar]
- 42.Lerner BH. New York City’s tuberculosis control efforts: the historical limitations of the “war on consumption.” Am J Public Health. 1993;83:758–766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Enarson D, Rouillon A. A history of the IUATLD. TB Notes. 2000;33–37.
- 44.Enarson DA. Tuberculosis control in low-income countries. In: Reichman LB, Hershfield ES, eds. Tuberculosis: A Comprehensive International Approach. 2nd ed. New York, NY: Marcel Dekker Inc; 2000:55–75.
- 45.Murray CJ, Styblo K, Rouillon A. Tuberculosis in developing countries: burden, intervention and cost. Bull Int Union Tuberc Lung Dis. 1990;65:6–24. [PubMed] [Google Scholar]
- 46.Kochi A. The global tuberculosis situation and the new control strategy of the World Health Organization. Tubercle. 1991;72:1–6. [DOI] [PubMed] [Google Scholar]
- 47.Gupta R, Kim JY, Espinal MA, et al. Public health: responding to market failures in tuberculosis control. Science. 2001;293:1049–1051. [DOI] [PubMed] [Google Scholar]
- 48.Sachs JD, Amoako KY, Aninat E, et al. Macroeconomics and Health: Investing in Health for Economic Development. Geneva, Switzerland: World Health Organization; 2001.
- 49.Manderson L. Public health developments in colonial Malaya: colonialism and the politics of prevention. Am J Public Health. 1999;89:102–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hunt NR. A Colonial Lexicon of Birth Ritual, Medicalization, and Mobility in the Congo. Durham, NC: Duke University Press; 1999.
- 51.Cooper F, Packard RM. International Development and the Social Sciences: Essays on the History and Politics of Knowledge. Berkeley: University of California Press; 1997.
- 52.Donnison CP. Blood pressure in the African native: its bearing upon the aetiology of hyperpiesia and arteriosclerosis. Lancet. January 5, 1929;6–7.
- 53.Clarke J. Rheumatic fever and rheumatoid arthritis: the geographical factor. Lancet. June 5, 1915:1169–1171.
- 54.Alimurung MM, Herrera F Jr, Guytingco A, Cruz PM. Heart disease in the Philippines: a seven-year (1947–1953) postwar survey of four Manila general hospitals. Am Heart J. 1955;50:293–302. [DOI] [PubMed] [Google Scholar]
- 55.Chavez I. The incidence of heart disease in Mexico. Am Heart J. 1942;24: 88–98. [Google Scholar]
- 56.Davies J. Pathology of Central African natives. Mulago Hospital Post Mortem Studies, IX: cardiovascular diseases. East Afr Med J. 1948;25:454–467. [PubMed] [Google Scholar]
- 57.Padmavati S. Rheumatic fever and rheumatic heart disease in developing countries. Bull World Health Organ. 1978;56:543–550. [PMC free article] [PubMed] [Google Scholar]
- 58.Beet EA. Rheumatic heart disease in Northern Nigeria. Trans R Soc Trop Med Hyg. 1956;50(6):587–592. [DOI] [PubMed] [Google Scholar]
- 59.Obineche EN. Pattern of cardiovascular disease in Lusaka. A review. East Afr Med J. 1976;53(8):435–439. [PubMed] [Google Scholar]
- 60.Rowland HA. Cardiovascular disease in Sierra Leone. West Afr Med J. 1965;14:99–114. [PubMed] [Google Scholar]
- 61.Mathur KS. Problem of heart disease in India. Am J Cardiol. 1960;5(1):60–65. [Google Scholar]
- 62.Vakil RJ. Cardiovascular diseases in India. Am J Cardiol. 1962;10:380–389. [DOI] [PubMed] [Google Scholar]
- 63.Miller DC, Spencer SS, White PD. Survey of cardiovascular disease among Africans in the vicinity of the Albert Schweitzer Hospital in 1960. Am J Cardiol. 1962;10:432–446. [DOI] [PubMed] [Google Scholar]
- 64.White PD. Notes on cardiovascular disease in Africa as encountered by an American physician on a brief visit to that continent in March and April, 1959. Am Heart J. 1961;61:133–134. [DOI] [PubMed] [Google Scholar]
- 65.Keys A, White PD, eds. Cardiovascular Epidemiology. New York, NY: Harper & Brothers; 1958.
- 66.Higginson J. Atherosclerosis, diet, and serum cholesterol in the South African Bantu. In: Keys A, White PD, eds. Cardiovascular Epidemiology. New York, NY: Harper & Brothers; 1958:34–41.
- 67.Omran AR. The epidemiologic transition: a theory of the epidemiology of population change. Milbank Mem Fund Q. 1971;49:509–538. [PubMed] [Google Scholar]
- 68.Strasser T, Dondog N, El Kholy A, et al. The community control of rheumatic fever and rheumatic heart disease: report of a WHO international cooperative project. Bull World Health Organ. 1981;59:285–294. [PMC free article] [PubMed] [Google Scholar]
- 69.Fejfar Z. Introduction. In: Shaper AG, Hutt MSR, Fejfar Z, eds. Cardiovascular Disease in the Tropics. London, England: British Medical Association; 1974:1–6.
- 70.Iliffe J. East African Doctors: A History of the Modern Profession. Cambridge, England: Cambridge University Press; 2002.
- 71.D’Arbela PG, Kanyerezi RB, Tulloch JA. A study of heart disease in the Mulago hospital, Kampala, Uganda. Trans R Soc Trop Med Hyg. 1966;60:782–790. [DOI] [PubMed] [Google Scholar]
- 72.Pobee JO. Cardiovascular research: a luxury in tropical Africa? East Afr Med J. 1987;64:396–410. [PubMed] [Google Scholar]
- 73.Ojiambo HP. Postgraduate medical training in Kenya. Lancet. 1967;2: 1414–1416. [DOI] [PubMed] [Google Scholar]
- 74.Makene WJ, Muindi JR. Some observations on congestive cardiac failure in African patients in Dar es Salaam. East Afr Med J. 1976;53:326–331. [PubMed] [Google Scholar]
- 75.Agarwal BL. Rheumatic heart disease unabated in developing countries. Lancet. 1981;2:910–911. [DOI] [PubMed] [Google Scholar]
- 76.Paul O. Take Heart: The Life and Prescription for Living of Dr Paul Dudley White. Boston, Mass: Harvard University Press; 1986.
- 77.Blackburn H. Introduction to Ancel Keys Lecture. Ancel Keys, pioneer. Circulation. 1991;84:1402–1404. [DOI] [PubMed] [Google Scholar]
- 78.Tunstall-Pedoe H, World Health Organization. MONICA Project. MONICA, Monograph, and Multimedia Sourcebook: World’s Largest Study of Heart Disease, Stroke, Risk Factors, and Population Trends 1979–2002. Geneva, Switzerland: World Health Organization; 2003.
- 79.Tunstall-Pedoe H, Vanuzzo D, Hobbs M, et al. Estimation of contribution of changes in coronary care to improving survival, event rates, and coronary heart disease mortality across the WHO MONICA Project populations. Lancet. 2000;355:688–700. [DOI] [PubMed] [Google Scholar]
- 80.Kim JY, Millen J, Gershman J, Irwin A. Dying for Growth: Global Inequality and the Health of the Poor. Monroe, Me: Common Courage Press; 2000.
- 81.Benatar SR. The World Bank, listening and learning. Lancet. 1996;347:1047. [DOI] [PubMed] [Google Scholar]
- 82.Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. 2004;291(21):2616–2622. [DOI] [PubMed] [Google Scholar]
- 83.Jamison DT, World Bank. Disease Control Priorities in Developing Countries. New York, NY: Oxford University Press; 1993.
- 84.Feachem RG. The Health of Adults in the Developing World. New York, NY: Oxford University Press; 1992.
- 85.Murray CJ, Lopez AD. Evidence-based health policy—lessons from the Global Burden of Disease Study. Science. 1996;274:740–743. [DOI] [PubMed] [Google Scholar]
- 86.Chockalingam A, Balaguer-Vintro I, eds. Impending Global Pandemic of Cardiovascular Disease. Challenges and Opportunities for Prevention and Control of Cardiovascular Diseases in Developing Countries and Economies in Transition. Barcelona, Spain: Prous Science; 1999. [PubMed]
- 87.The Victoria Declaration on Heart Health. Victoria, British Columbia: International Heart Health Conference; 1992.
- 88.Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14(1): 32–38. [DOI] [PubMed] [Google Scholar]
- 89.Puska P. The North Karelia Project: 20 Year Results and Experiences. Helsinki, Finland: National Public Health Institute; 1995.
- 90.Beaglehole R. Primary prevention must have priority. Bull World Health Organ. 2001;79(10):986–987. [Google Scholar]
- 91.Howson CP, Reddy KS, Ryan TJ, Bale JR, eds. Control of Cardiovascular Diseases in Developing Countries: Research, Development, and Institutional Strengthening. Washington, DC: National Academy Press; 1998.
- 92.Bobadilla JL, Costello CA, Mitchell F. Premature Death in the New Independent States. Washington, DC: National Academy Press; 1997. [PubMed]
- 93.Okie S. Global health—the Gates–Buffett effect. N Engl J Med. 2006;355:1084–1088. [DOI] [PubMed] [Google Scholar]
- 94.Sachs JD. Beware false tradeoffs. Foreign Affairs, January 23, 2007. Available at: http://www.foreignaffairs.org/special/global_health/sachs. Accessed March 1, 2007.
- 95.Yach D, Leeder SR, Bell J, Kistnasamy B. Global chronic diseases. Science. 2005;307:317. [DOI] [PubMed] [Google Scholar]
- 96.Ordunez-Garcia P, Munoz JL, Pedraza D, Espinosa-Brito A, Silva LC, Cooper RS. Success in control of hypertension in a low-resource setting: the Cuban experience. J Hypertens. 2006;24:845–849. [DOI] [PubMed] [Google Scholar]
- 97.Levine R, Kinder M, What Works Working Group. Millions Saved: Proven Successes in Global Health. Washington, DC: Center for Global Development; 2004.
- 98.Farmer P. The major infectious diseases in the world—to treat or not to treat? N Engl J Med. 2001;345:208–210. [DOI] [PubMed] [Google Scholar]
- 99.Walsh JA, Warren KS. Selective primary health care: an interim strategy for disease control in developing countries. N Engl J Med. 1979;301:967–974. [DOI] [PubMed] [Google Scholar]
- 100.Walton DA, Farmer PE, Lambert W, Leandre F, Koenig SP, Mukherjee JS. Integrated HIV prevention and care strengthens primary health care: lessons from rural Haiti. J Public Health Policy. 2004;25:137–158. [DOI] [PubMed] [Google Scholar]
- 101.Frenk J. Bridging the divide: global lessons from evidence-based health policy in Mexico. Lancet. 2006;368:954–961. [DOI] [PubMed] [Google Scholar]