

Abstract
Objectives. We measured the psychosocial effect of orphanhood in a sub-Saharan African population and evaluated a new framework for understanding the causes and consequences of psychosocial distress among orphans and other vulnerable children.
Methods. The framework was evaluated using data from 5321 children aged 12 to 17 years who were interviewed in a 2004 national survey in Zimbabwe. We constructed a measure of psychosocial distress using principle components analysis. We used regression analyses to obtain standardized parameter estimates of psychosocial distress and odds ratios of early sexual activity.
Results. Orphans had more psychosocial distress than did nonorphans. For both genders, paternal, maternal, and double orphans exhibited more-severe distress than did nonorphaned, nonvulnerable children. Orphanhood remained associated with psychosocial distress after we controlled for differences in more-proximate determinants. Maternal and paternal orphans were significantly more likely than were nonorphaned, nonvulnerable children to have engaged in sexual activity. These differences were reduced after we controlled for psychosocial distress.
Conclusions. Orphaned adolescents in Zimbabwe suffer greater psychosocial distress than do nonorphaned, nonvulnerable children, which may lead to increased likelihood of early onset of sexual intercourse and HIV infection. The effect of strategies to provide psychosocial support should be evaluated scientifically.
HIV epidemics in sub-Saharan Africa are giving rise to ever larger numbers of orphaned children. Between 1990 and 2010, the Joint United Nations Programme on HIV/AIDS estimates that the total number of children younger than 18 who have lost 1 or both parents to AIDS will increase from 550 000 (1.9% of all orphans) to 18.4 million (36.8%).1 The devastating sociodemographic effects of HIV epidemics1–3 have raised widespread concern about the psychosocial effects of orphanhood,4–6 and substantial funds are being invested in programs to provide psychosocial support to orphans.7–9
In a small study of 41 pairs of orphans and nonorphans, Makame et al.10 found that orphans had higher scores for internalizing problems compared with nonorphans and that nearly 3 times as many orphans as nonorphans had contemplated suicide. However, the empirical basis for understanding the extent, nature, causal mechanisms, and consequences of orphanhood in the context of large-scale HIV epidemics remains extremely weak.4,6,11
There has been progress in developing theoretical frameworks on the effects of HIV-associated orphanhood.12 However, there has been relatively little focus on developing frameworks that identify the causal pathways through which orphan experience can lead to psychosocial distress or the consequences of psychosocial distress for child development.1,13 Such frameworks have not previously been tested with data.
Our study had 2 objectives: first, to propose a new theoretical framework for studying the causes and consequences of psychosocial problems among orphans and other children made vulnerable by HIV/AIDS and, second, to test and evaluate aspects of this framework using data from a large-scale, population-based, national survey in Zimbabwe.
METHODS
Theoretical Framework
Our aim (Figure 1 ▶) was to identify and improve understanding of interrelationships between (1) HIV/AIDS-associated parental illness and death, (2) the psychosocial distress that manifests in children affected by HIV/AIDS, and (3) children’s development and future life chances. Our theoretical framework was developed from literature that addresses causes and consequences of psychosocial distress among children from developed and developing countries.
FIGURE 1—
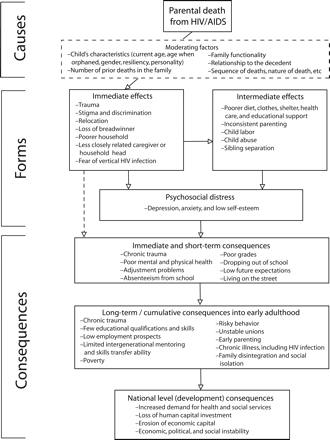
Theoretical framework on the causes and consequences of psychosocial distress among children orphaned and made vulnerable by HIV/AIDS.
Note. Dotted line indicates that the pathway does not involve psychosocial distress. The effects of the different processes in the framework are expected to vary depending on the social context.
We proposed that the effect of parental (or other caregiver) loss is moderated by the number, sequence, and timing of previous deaths in the family and the cause of parental death, by the child’s characteristics, and by family and other social and contextual circumstances,14 which inhibit or facilitate the development of psychosocial distress. Children may experience a number of shocks and changes before or immediately after the death of the parent. These include trauma and major adjustments in place of residence, childcare arrangements, and available financial resources.15,16 These changes may be so devastating and demanding that they cause psychosocial distress including depression, anxiety, and low self-esteem.4,10 However, some of the changes in children’s circumstances may be more subtle and have a less direct and more gradual effect on their psychosocial well-being. Over time, orphaned children may develop a sense of relative deprivation as their poorer circumstances coupled with stigma and discrimination result in their continually having reduced access to services and material resources.4,10
We hypothesized that psychological distress resulting from parental illness and loss could have a number of immediate or short-term adverse consequences during childhood including chronic trauma, adjustment problems, low future expectations, poor health, reduced school attendance and performance, school drop-out, and living on the streets.4,10 The compounding effects of problems that result from parental and caregiver loss, and other life stressors experienced during childhood, may affect the opportunities an orphaned child will be able to access during adulthood and his or her ability to capitalize on these opportunities.17,18 For example, chronic trauma and low qualifications and skills could translate into limited employment prospects, early parenting, unstable relationships, social isolation, poverty, and behaviors that predispose toward poor health outcomes, including HIV infection.19
Disadvantages and psychosocial distress experienced during childhood not only affect orphans’ ability to capitalize on occupational and social opportunities for their own survival as adults but also have implications for their ability to contribute to national development. Failure to carve out productive lives for themselves will result in their being dependent on government and relatives for health and social services and may mean that their children will endure a further cycle of poverty and ill health. Inability to cater to their own needs and those of their children would render current generations of orphans a threat to future economic, political, and social security.
Life Circumstances in Zimbabwe
The theoretical framework was evaluated in Zimbabwe. The predominant traditional cultures are patrilineal (i.e., lineage is recognized through the father’s line) and patrilocal (i.e., the wife moves in with the husband’s family or to the husband’s community) and based around a strong extended family system but are being eroded by forces of socioeconomic development.20,21 Nonorphaned children generally live with their biological parents but may reside with other relatives for socialization, education, and other reasons. Paternal orphans typically live with their mothers but the circumstances of children whose mothers have died vary; some live with their fathers and stepmothers, whereas others stay with maternal relatives or elderly grandparents.22
Children divide their time between home and school duties. Typically, duties at home include washing dishes, sweeping the yard, fetching water, weeding and watering plants, and preparing meals. School attendance is mandatory at the primary school level and continues to provide a good standard of education in academic and vocational skills to prepare students for the minimum of 5 O-level exam passes (taken by students around age 15) needed for employment in the country’s shrinking but still relatively substantial formal sector. Attending school is also important in socialization (e.g., through inculcation of roles and responsibilities, provision of role models, and opportunities to form friendships) and offers access to counseling from teachers and links to important resources including life skills and HIV/AIDS education.23 However, illness or death of household members is increasingly common because of HIV/AIDS and can result in children failing to attend school, because fees go unpaid or the children are needed at home to carry out household chores.21 Lack of school materials such as uniforms and even clean clothes can make orphans and other children from poor families miss school because they feel ashamed of their appearance.
Data
We tested the relations between orphanhood, psychosocial status and selected mediating factors, and the consequences of psychosocial distress on patterns of sexual intercourse using data from the Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe 2004. The survey was designed to improve understanding of the circumstances of orphans and vulnerable children and to collect baseline values for outcome indicators. The survey was sponsored by the Government of Zimbabwe and UNICEF as part of the Government of Zimbabwe–UNICEF–European Union Country Orphan and Vulnerable Children Program.
The survey was designed on the basis of international guidelines for orphan and vulnerable children research24 and is detailed elsewhere.25 Briefly, the survey was conducted between November and December 2004 in 21 purposively selected districts of Zimbabwe. The districts were selected on the basis of poverty and education levels. In each district, 8 census enumeration areas were selected initially according to probability proportional to size, from which 5 were purposively chosen to ensure representative geographical coverage. In Zimbabwe, census enumeration areas are delineated to contain around 100 households. Thus, approximately 500 eligible households were expected to be found in each district. Assuming an average of 0.7 orphans per household, it was expected that approximately 350 orphans would be enumerated in each district.
The survey was conducted in 2 parts. In an initial household survey, data were collected for the general demographic, socioeconomic, and health status of all household members. Two children (1 boy and 1 girl) aged 12–17 years were then selected at random from each household and asked questions that related to psychosocial distress and sexual intercourse. Up to 3 visits were made for each of the 2 interviews (household and individual) to maximize participation. Questionnaires were translated into the 2 most common local languages (Shona and Ndebele) and then back-translated into English and checked to ensure the accuracy of the original translation. Given the sensitive nature of some of the questions, children were interviewed on their own by enumerators of the same gender.
Data Analysis
Orphans were subdivided into those who had lost both of their parents (double orphans), their mother only (maternal orphans), and their father only (paternal orphans). In a recent study in eastern Zimbabwe, 82% of orphaned children had a parent living with HIV 3 years previously.26 Vulnerable children were defined as those who were either living in a household that experienced the death of an adult other than a parent in the last year or who lived in a household with a chronically ill person.
The outcome measure of psychosocial distress was derived from emotional, psychological, physical, behavioral, and social-connectedness questions (available as a supplement to the online version of this article at http://www.ajph.org) purposively selected from the Child Behavior Checklist, Rand Mental Health Inventory, and Beck’s Depression Inventory.27–30 Similar questions have been used successfully in studies in Bulawayo, Zimbabwe,31 and other settings in sub-Saharan Africa.10,32–35 Principle components analysis36 was used to reduce the number of variables and to identify the underlying structure. We conducted separate analyses for social connectedness and psychosocial distress variables. In each case, the first factor was the only factor to account for more than 10% of the variance (98.2% for social connectedness and 22.7% for psychosocial distress) and was used as the outcome measure in the primary analyses. All variable loadings on this factor were more than 0.3 for both social connectedness and psychosocial distress. The Cronbach α test37 was applied to all variables that contributed to each outcome measure, to assess the internal consistency of the measures used. Power calculations indicated that the sample size in the Zimbabwe survey was sufficient to detect an effect of orphanhood on the psychosocial distress outcome variable (an estimated effect size of 0.17 with 90% power at a significance level of 95%, assuming an equal standard deviation for the outcome in both groups).
Ordinary least squares regression was used to calculate standardized parameter estimates and test for associations between orphanhood and vulnerable child experience and psychosocial distress, and to assess the effects of the hypothesized immediate and intermediate determinants including gender, school enrollment, relationship to household head, location of residence, poverty (living in the poorest quintile of households as measured by the Demographic and Health Surveys wealth index38), social connectedness, and external support. These effects were tested initially in age-adjusted models and then in multivariate models. Logistic regression was used to test the hypothesized associations between psychosocial distress and having started to have sexual intercourse, after we controlled for possible confounding variables. To limit confounding with orphan and vulnerable child status, the hypothesized determinants of psychosocial distress and early sexual intercourse were evaluated initially in nonorphaned, non-vulnerable children.
RESULTS
A total of 12356 households were identified. These households contained 31415 children aged 0 to 17 years, of whom 13688 (44%) were orphaned or vulnerable children and 451 (1.5%) had missing information on their parental or vulnerability status. Of the 5328 individuals aged 12 to 17 years selected for our study, 5295 (99%) were interviewed about their psychosocial well-being and experiences of sexual intercourse. Of these, 87% (n=4660: 548 double orphans; 281 maternal orphans; 1123 paternal orphans; 543 nonorphaned, vulnerable children; and 2165 nonorphaned, nonvulnerable children) had complete information on psychosocial distress and social connectedness variables. Cronbach’s α was 0.76 and 0.78, respectively, for the psychosocial distress (16 items) and social connectedness (9 items) variables, which indicated high levels of internal consistency.
Overall, girls were found to have more psychosocial distress than did boys (B=0.30; 95% confidence interval [CI]=0.21, 0.40). No difference was found between younger (aged 12–14 years) and older (aged 15–17 years) children (P=.6). Compared with nonorphans, orphans had more psychosocial distress for both boys (B=0.13; 95% CI=0.06, 0.20) and girls (B=0.20; 95% CI=0.11, 0.29) and at younger (B=0.14; 95% CI=0.07, 0.22) and older (B=0.18; 95% CI=0.10, 0.27) ages. Orphans whose fathers or mothers had died within the last year showed signs of more-severe psychosocial distress than did those whose parents had died further into the past (data not shown), but these differences were not significant (P >.05). For both genders, each type of orphan exhibited more-severe distress than did nonorphaned, nonvulnerable children (Figure 2 ▶). Nonorphaned, vulnerable boys, but not girls, also showed evidence of more psychosocial distress compared with nonorphaned, nonvulnerable children. (B=0.13; 95% CI=0.01, 0.24).
FIGURE 2—

Effects of orphan and vulnerable child status on (a) psychosocial distress, (b) early sexual intercourse, and (c) high-risk sexual intercourse: Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe 2004.
Note. Horizontal lines represent the 95% confidence intervals.
As explained in the “Methods” section, the intermediate or more-proximate determinants of psychosocial distress in children were initially identified in nonorphaned, nonvulnerable children. The results of the bivariate and multivariate analyses were very similar, so only the results from the multivariate analysis are reported here. Variables that were positively associated with psychosocial distress were residing in an urban area (B= 0.16; 95% CI = 0.04, 0.28), on a commercial farm (B= 0.46; 95% CI = 0.08, 0.84), in a poor household (B= 0.14; 95% CI = 0.04, 0.24) or in a household that had received external support (B= 0.21; 95% CI = −0.01, 0.44), and being unrelated to the closest caregiver (B = 0.14; 95% CI = 0.03, 0.24). Residing in a household headed by a woman (B= −0.11; 95% CI=−0.19, −0.02) and receiving psychosocial support from the closest caregiver (B= −0.05; 95% CI = −0.09, −0.01) had protective effects against psychosocial distress. No significant effects were observed for relationship to household head or age of household head. It should be noted, however, that in some cases, lack of significant results in the above determinants could be the result of low numbers of nonorphaned, nonvulnerable children who had experienced these circumstances.
Table 1 ▶ shows the frequencies of the hypothesized sociodemographic determinants of psychosocial distress by form of orphan or vulnerable child experience. Nonorphaned, vulnerable children and maternal orphans were the most likely to be found in towns and commercial farms. Double and paternal orphans were found disproportionately in poorer households and those headed by women and more frequently reported having received external support and being out of school. All types of orphaned and vulnerable children were more likely than were nonorphaned, nonvulnerable children to be living in a household headed by a person younger than 20 and, with the exception of nonorphaned, vulnerable children, were more likely to be found in households headed by a nonrelative and to be unrelated to their closest adult. Overall (i.e., including among respondents of both genders regardless of whether they had ever had sexual intercourse), reports of forced sexual intercourse were relatively rare but were more common among paternal orphans.
TABLE 1—
Adjusted Odds Ratios (AORs) for Selected Sociodemographic Determinants of Psychosocial Distress Among Children Aged 12 to 17 Years, by Type of Experience: Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe, 2004
| Double Orphans | Maternal Orphans | Paternal Orphans | Other Vulnerable Children | ||||||||||
| Determinant | No. (%) | AOR (95% CI) | P | No. (%) | AOR (95% CI) | P | No. (%) | AOR (95% CI) | P | No. (%) | AOR (95% CI) | P | Nonorphaned, nonvulnerable children, No. (%) |
| Total sample | 548 (100) | 281 (100) | 1123 (100) | 543 (100) | 2165 (100) | ||||||||
| Location: Urban and commercial farms vs subsistence farms | 70 (13) | 1.0 (0.8, 1.3) | .969 | 46(17) | 1.3 (0.9, 1.9) | .098 | 128 (12) | 0.9 (0.7, 1.1) | .298 | 85 (18) | 1.4 (1.1, 1.8) | .011 | 273 (13) |
| Povertya: Poorest quintile vs higher | 128 (23) | 1.6 (1.2, 2.0) | <.001 | 43 (15) | 0.9 (0.6, 1.3) | .577 | 232 (21) | 1.3 (1.1, 1.6) | .003 | 87 (16) | 1.0 (0.7, 1.2) | .758 | 359 (17) |
| Gender of household head: Woman vs man | 266 (49) | 2.8 (2.3, 3.3) | <.001 | 87 (31) | 1.3 (1.0, 1.7) | .055 | 854 (76) | 9.3 (7.8, 11.0) | <.001 | 160 (30) | 1.2 (1.0, 1.5) | .061 | 552 (26) |
| Relationship to household head | |||||||||||||
| Not related vs related or self | 24 (4) | 2.3 (1.4, 3.9) | .001 | 17 (6) | 3.4 (1.9, 6.1) | <.001 | 41 (4) | 2.0 (1.3, 3.2) | .002 | 10 (2) | 1.0 (0.5, 2.1) | .915 | 39 (2) |
| Self | 10 (2) | . . . | 5 (2) | . . . | 8 (1) | . . . | 10 (2) | . . . | 0 (0) | ||||
| Age of household head, y: <20 vs ≥ 20 | 26 (5) | 11.5 (5.4, 24.8) | <.001 | 6(2) | 5.0 (1.7, 14.1) | .003 | 19 (2) | 4.1 (1.8, 9.0) | .001 | 15 (3) | 7.0 (3.0, 16.1) | <.001 | 9 (0) |
| Relationship to closest adult: Not related vs related | 125 (23) | 1.5 (1.2, 1.9) | .001 | 59 (21) | 1.4 (1.0, 1.9) | .042 | 217 (19) | 1.3 (1.0, 1.5) | .020 | 80 (15) | 0.9 (0.7, 1.2) | .618 | 341 (16) |
| Support from closest adult: Social Connectedness (index) | 548 (100) | −0.03 (−0.1, 0.1) | .499 | 281 (100) | 0.00 (−0.1, 0.1) | .966 | 1,123 (100) | −0.04 (−0.1, 0.0) | .281 | 543 (100) | 0.02 (−0.1, 0.1) | .661 | 2,165 (100) |
| External psychosocial support: Some support vs no support | 34 (6) | 2.2 (1.5, 3.4) | <.001 | 11 (4) | 1.4 (0.7, 2.6) | .361 | 51 (5) | 1.6 (1.1, 2.3) | .017 | 19 (4) | 1.2 (0.7, 2.0) | .511 | 64 (3) |
| School enrollment: Not enrolled vs enrolled | 174 (33) | 1.5 (1.2, 1.9) | <.001 | 79 (30) | 1.2 (0.9, 1.6) | .300 | 320 (30) | 1.3 (1.1, 1.6) | .002 | 127 (24) | 1.0 (0.8, 1.3) | .702 | 502 (24) |
| Sexual abuse: Forced sexual intercourse vs none | 2 (0) | 2.1 (0.4, 11.7) | .387 | 0 (0) | . . . | 10 (1) | 5.0 (1.6, 16.0) | .007 | 0 (0) | . . . | 4 (2) | ||
| Chronically ill adult in household: Yes vs. no | 43 (8) | . . . | 46 (16) | . . . | 139 (12) | . . . | 214 (39) | . . . | 0 (0) | ||||
Note. CI = confidence interval. Double orphans had lost both of their parents, maternal orphans had lost their mother only, and paternal orphans had lost their father only. Vulnerable children were defined as those who were either living in a household that experienced the death of an adult other than a parent in the last year or who lived in a household with a chronically ill person.
aPoverty was measured in quintiles derived from the Demographic and Health Surveys wealth index.
After we controlled for differences in exposure to sociodemographic determinants of psychosocial distress that were hypothesized to lie on the causal pathway between orphanhood and psychosocial distress, the strength of the observed associations was reduced (Table 2 ▶). However, these associations remained statistically significant.
TABLE 2—
Effect of Orphan and Vulnerabilty Status on Psychosocial Distress Among Children Aged 12 to 17 Years After Accounting for the Effects of Observed Intermediate Determinants: Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe, 2004
| Double Orphans | Maternal Orphans | Paternal Orphans | ||||||||
| Determinant | No. | Ba (95% CI) | P | No. | Ba (95% CI) | P | No. | Ba (95% CI) | P | Nonorphaned, nonvulnerable children,b No. |
| Age- and gender-adjusted models: Orphan | 548 | 0.25 (0.16, 0.34) | < .001 | 281 | 0.22 (0.10, 0.34) | < .001 | 1123 | 0.13 (0.06, 0.20) | < .001 | 2165 |
| Multivariate models | ||||||||||
| Orphan | 548 | 0.21 (0.11, 0.30) | < .001 | 281 | 0.19 (0.07, 0.30) | .002 | 1123 | 0.12 (0.04, 0.20) | .003 | 2165 |
| Location (compared with subsistence farms): Urban and commercial farms | 70 | 0.21 (0.10, 0.31) | < .001 | 46 | 0.19 (0.07, 0.30) | .001 | 128 | 0.17 (0.07, 0.27) | .001 | 273 |
| Poverty: Poorest quintilec | 128 | 0.14 (0.04, 0.23) | .004 | 43 | 0.10 (0.00, 0.20) | .056 | 232 | 0.10 (0.02, 0.19) | .018 | 359 |
| Gender of household head: Woman | 266 | −0.08 (−0.16, 0.00) | .047 | 87 | −0.11 (−0.19, −0.02) | .012 | 854 | −0.05 (−0.12, 0.03) | .211 | 552 |
| Age of household head: < 20 y | 26 | 0.61 (0.27, 0.95) | < .001 | 6 | 0.75 (0.26, 1.24) | .003 | 19 | 0.01 (−0.35, 0.37) | .954 | 9 |
| Relationship of closest adult: Not related | 125 | 0.14 (0.04, 0.23) | .004 | 59 | 0.14 (0.04, 0.25) | .006 | 217 | 0.17 (0.08, 0.25) | < .001 | 341 |
| Support from closest adult: Social Connectedness (index) | 548 | −0.03 (−0.07, 0.01) | .100 | 281 | −0.05 (−0.09, −0.01) | .010 | 1123 | −0.04 (−0.07, −0.01) | .014 | 2165 |
| External psychosocial support: Some support (compared with none) | 34 | 0.31 (0.12, 0.50) | .002 | 11 | 0.22 (0.00, 0.44) | .049 | 51 | 0.14 (−0.04, 0.32) | .117 | 64 |
| School enrollment status: Out of school | 174 | 0.15 (0.06, 0.24) | .001 | 79 | 0.20 (0.11, 0.29) | < .001 | 320 | 0.22 (0.14, 0.30) | < .001 | 502 |
| R2 | .054 | .049 | .044 | |||||||
Note. CI = confidence interval. Double orphans had lost both of their parents, maternal orphans had lost their mother only, and paternal orphans had lost their father only. Vulnerable children were defined as those who were either living in a household that experienced the death of an adult other than a parent in the last year or who lived in a household with a chronically ill person.
aAdjusted standardized parameter estimate from ordinary least squares regression comparing orphaned and vulnerable children to nonorphaned, nonvulnerable children.
bNo difference was observed among nonorphaned vulnerable children compared with nonorphaned, nonvulnerable children in the age- and gender-adjusted model (P = .316).
cPoverty was measured in quintiles derived from the Demographic and Health Surveys wealth index.
Of the children surveyed, 10.5% (251 out of 2398) of boys and 8% (181 out of 2262) of girls aged 12 to 17 years reported having had sexual intercourse. Overall, orphaned and vulnerable children were more likely to have had sexual intercourse than were nonorphaned, nonvulnerable children, but the difference was not statistically significant for either gender (boys: 11.4% vs 9.3%; age-adjusted odds ratio [OR] = 1.25; 95% CI = 0.95, 1.64; girls: 9.2% vs 6.7%; age-adjusted OR = 1.35, 95% CI = 0.98, 1.86). Maternal orphans (boys: age-adjusted OR = 1.88; 95% CI = 1.13, 3.15; girls: age-adjusted OR = 2.01; 95% CI = 1.15, 3.49), and paternal orphans (both genders combined: gender and age-adjusted OR = 1.29; 95% CI = 1.00, 1.67) but not double orphans (both genders combined, P ≥ .99) were more likely than were nonorphaned, nonvulnerable children to have started having sexual intercourse (Figure 2 ▶). Other vulnerable children were also more likely to have started having sexual intercourse, but the difference was not statistically significant (both genders combined, P = .087).
When the analysis was restricted to unmarried individuals, maternal orphans (adjusted OR = 1.70; 95% CI = 1.11, 2.63), paternal orphans (adjusted OR = 1,41, 95% CI = 1.07, 1.86), and vulnerable children (adjusted OR = 1.58; 95% CI = 1.11, 2.24) were all more likely than were nonorphaned, nonvulnerable children to report commencement of sexual intercourse, but there was still no difference for double orphans (P ≥ .99).
Of those who had started having sexual intercourse, 56% (141 out of 251) of the boys and 44% (79 out of 181) of the girls reported high-risk sexual intercourse. Overall, orphaned or vulnerable children who had started to have sexual intercourse were nonsignificantly more likely to have had high-risk sexual intercourse than were their nonorphaned, nonvulnerable counterparts (boys: 59.3% vs 52.0%; adjusted OR=1.60, 95% CI=0.93, 2.75; girls: 48.1% vs 40.6%; adjusted OR=1.38; 95% CI=0.75, 2.56). Male paternal orphans (adjusted OR=1.96; 95% CI=1.00, 3.82) and female nonorphaned, vulnerable children (adjusted OR=3.09; 95% CI=1.09, 8.76) were more likely than were nonorphaned, nonvulnerable children to have had high-risk sexual intercourse (Figure 2 ▶).
Once again, the results of the univariate and multivariate analyses of intermediate determinants for sexual intercourse debut among nonorphaned, nonvulnerable children were similar for both genders. Therefore, only the results of the multivariate analysis are reported. No longer being enrolled in school was associated with early onset of sexual intercourse (boys: adjusted OR = 2.52; 95% CI = 1.61, 3.94; girls: adjusted OR = 7.10; 95% CI = 3.90, 12.92). A higher score on the psychosocial distress scale was also positively associated with onset of sexual intercourse (boys: adjusted OR = 1.36; 95% CI = 1.06, 1.75; girls: adjusted OR = 1.23; 95% CI = 1.01, 1.50). Among girls, living in a household headed by a woman was associated with early sexual intercourse (adjusted OR = 1.81; 95% CI = 1.02, 3.19). Among both genders, greater poverty showed a non-significant reduction in the likelihood of sexual intercourse, but the numbers of cases were small. Care must be taken when interpreting these results, because the associations identified could be the result of reverse causality (e.g., early onset of sexual intercourse could lead to leaving school at a younger age or psychosocial distress rather than vice versa).
After also adjusting for differences in location of residence, exposure to extreme poverty, gender of household head, school enrollment, and psychosocial distress (Table 3 ▶), only maternal orphans remained associated with early onset of sexual intercourse (adjusted OR = 1.71; 95% CI = 1.14, 2.55). Unmarried maternal orphans were more likely than were unmarried nonorphaned, nonvulnerable children to be living in a household headed by a grandparent, which in turn was associated with increased risk of having sexual intercourse. After further adjusting for relationship to household head, maternal orphans also ceased to show a significant association with early onset of sexual intercourse among unmarried individuals (P = .2).
TABLE 3—
Effect of Orphan and Vulnerable Children Status on Onset of Sexual Intercourse Among Children Aged 12 to 17 Years After Accounting for Effects of Psychosocial Distress and Other Observed Intermediate Determinants: Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe, 2004
| Double Orphans | Maternal Orphans | Paternal Orphans | Other Vulnerable Children | ||||||||||
| Determinate | No. | AORa (95% CI) | P | No. | AORa (95% CI) | P | No. | AORa (95% CI) | P | No. | AORa (95% CI) | P | Nonorphaned, nonvulnerable children, No. |
| Age- and gender-adjusted models: Orphaned and vulnerable children | 548 | 0.97 (0.69, 1.38) | .875 | 281 | 1.95 (1.34, 2.84) | .001 | 1123 | 1.29 (1.00, 1.67) | .049 | 543 | 1.34 (0.96, 1.87) | .087 | 2165 |
| Multivariate models | |||||||||||||
| Orphaned and vulnerable children | 548 | 0.78 (0.54, 1.13) | .196 | 281 | 1.71 (1.14, 2.55) | .009 | 1123 | 1.07 (0.80, 1.47) | .667 | 543 | 1.29 (0.91, 1.83) | .149 | 2165 |
| Location (compared with subsistence farms): Urban and commercial farms | 70 | 0.79 (0.50, 1.25) | .313 | 46 | 0.74 (0.46, 1.19) | .211 | 128 | 0.80 (0.53, 1.20) | .278 | 94 | 0.74 (0.47, 1.19) | .222 | 273 |
| Poverty: Poorest quintile | 128 | 0.56 (0.36, 0.86) | .008 | 43 | 0.61 (0.39, 0.95) | .029 | 232 | 0.70 (0.49, 1.00) | .049 | 87 | 0.69 (0.45, 1.05) | .086 | 359 |
| Gender of household head: Woman | 266 | 1.29 (0.94, 1.78) | .117 | 87 | 1.42 (1.02, 1.97) | .036 | 854 | 1.18 (0.88, 1.59) | .273 | 160 | 1.53 (1.12, 2.10) | .008 | 552 |
| School enrollment status: Out of school | 174 | 3.76 (2.77, 5.11) | <.001 | 79 | 3.39 (2.48, 4.64) | <.001 | 320 | 3.55 (2.72, 4.65) | <.001 | 127 | 3.76 (2.78, 5.09) | <.001 | 502 |
| Psychosocial distress: Greater variable score | 548 | 1.34 (1.18, 1.53) | <.001 | 281 | 1.31 (1.15, 1.49) | <.001 | 1123 | 1.24 (1.10, 1.39) | <.001 | 543 | 1.35 (1.18, 1.54) | <.001 | 2165 |
| Pseudo-R2 | .166 | .176 | .159 | .172 | |||||||||
Note. AOR = adjusted odds ratio; CI = confidence interval. Double orphans had lost both of their parents, maternal orphans had lost their mother only, and paternal orphans had lost their father only. Vulnerable children were defined as those who were either living in a household that experienced the death of an adult other than a parent in the last year or who lived in a household with a chronically ill person.
aOdds ratios were adjusted for age and gender and, in multivariate models, observed determinants of commencement of sexual intercourse.
Being out of school and increased psychosocial distress were positively and independently associated with early onset of sexual intercourse for each form of orphanhood and vulnerability, regardless of whether those who were already married were included (P < .005, in all cases). Residence in the poorest quintile of households was associated with reduced likelihood of early onset of sexual intercourse in each orphanhood or vulnerability status subgroup.
DISCUSSION
In 2005, HIV prevalence among adults aged 15 to 49 years and the number of children aged 0 to 14 years orphaned by HIV/AIDS in Zimbabwe were estimated at 20% (range: 17%–24%) and 1 050 000, respectively.39 Against the backdrop of this large-scale, maturing epidemic, we found evidence that orphaned adolescents had elevated psychosocial distress and were more likely than were nonorphaned, nonvulnerable children to have begun sexual activity. Differences in age, gender, place of residence, exposure to severe poverty, relationship to household head, school enrollment, and support from closest adult and from external sources explained only a small part of the increased psychosocial distress seen in orphaned children. However, more-pronounced psychosocial distress showed an independent association with early onset of sexual intercourse.
Our findings are consistent with those from previous studies that have also found increased psychosocial distress among girls, orphans, and children living in poverty or not enrolled in school.6,10,11 However, our study, to our knowledge, was the first to obtain statistically robust measurements from a large national sample, to distinguish the effects by type of orphan experience, and to apply data to a theoretical framework for understanding how psychosocial distress can arise among orphaned and vulnerable children and the consequences during and after childhood.
Limitations
The cross-sectional nature of the survey made it difficult to draw firm inferences on directions of causality—e.g., between psychosocial distress and early sexual intercourse. Nonetheless, our results were consistent with the causal pathway hypothesized in the conceptual framework, wherein parental death causes psychosocial distress, which in turn leads to early onset of sexual intercourse. The data suggest that poverty and not being in school can mediate the relationship between form of orphanhood and psychosocial distress. However, because the determinants tested here explained only a small part of the increase in psychosocial distress, factors such as trauma, stigma, and discrimination, which could not be measured using the current data, might also be important.
In a study in eastern Zimbabwe,40 children reported that being in poorer households and being out of school were sources of distress. For example, poverty could result in lack of presentable clothing, which could lead to absence from social gatherings or visits to relatives and created difficulties in finding friends. Children who did not attend school lacked information and felt excluded from social circles. However, within households, it was said that orphans could receive less-preferential treatment in the allocation of resources, including clothing, than the families’ own biological children. Among children in school, orphans had less time for and less help with homework compared with nonorphans.
Poorer districts were purposefully selected in the Survey on Orphans and Vulnerable Children in Rural and Urban High Density Zimbabwe 2004, so the data probably over-represent poorer households; therefore, we cannot be certain that the relations found between orphanhood, psychosocial distress, and early onset of sexual intercourse hold at a national level. Although our summary indicator of psychological distress showed good internal reliability, as with all such questionnaire-based assessments applied to new populations, we cannot be sure that the measure captured all culturally important aspects of psychosocial distress, nor can we be certain that the weightings assigned to variables (through principle components analysis) reflect their intrinsic seriousness (“thinking of killing yourself” vs “being happy”).
Conclusions
The substantive findings of the study provide important new information to guide policy on forms of psychosocial support and optimal targeting strategies for orphans and vulnerable children. The results suggest that all forms of orphans are at increased vulnerability to psychosocial distress and may be in need of support. Although the statistical models explained only a part of this increased vulnerability, the results did confirm—for those aged 12 to 17 years—earlier suggestions23 that school enrollment can help to mitigate the psychosocial distress associated with orphanhood. Similarly, extreme poverty, which was indicated by being in a household in the poorest quintile, was found to be associated with psychosocial distress for all types of orphans, so targeted alleviation of poverty could also have a part to play.
Social connectedness, defined as being related to the closest adult and receiving meaningful support from this adult, was associated with reduced psychosocial distress. Thus, support that enables orphaned and vulnerable children to remain in households with close relatives could also reduce psychosocial distress. A negative association has been found between external psychosocial support and greater psychosocial distress, which is troubling; however, this could reflect that successful targeting outweighed the initial effectiveness of these programs.
In Zimbabwe, median age at first sexual intercourse is later than in many other African countries (18 years among girls and 19 years among boys41). Nevertheless, our finding that maternal orphans, in particular, are at risk for early onset of sexual intercourse is consistent with findings from other studies in urban and rural areas, which have shown a consequent increase in HIV infection among adolescent girls.42,43 Thus, programs to reduce psychosocial distress among orphaned and vulnerable children could contribute to reducing the spread of HIV infection.
Acknowledgments
We were funded by UNICEF and the Ministry of Public Service, Labor, and Social Welfare, Zimbabwe (grant SSA/ZIMA/2005/00001555-0), the World Bank (grant 2005/304304), the Wellcome Trust (grant 069516/Z/02/Z), and the Southern African AIDS Trust.
We thank the research assistants for collecting the data, and colleagues for support during the preparation of this article.
Peer Reviewed
Contributors C.A. Nyamukapa, S. Gregson, and M.C.H. Jukes developed the theoretical framework, designed the study, and drafted the article. B. Lopman and H. J. Watts assisted with the statistical analysis. S. Saito and R. Monasch coordinated the Survey on Orphans and Other Vulnerable Children in Rural and High Density Zimbabwe 2004 and prepared the data for analysis. All authors contributed to the study design, interpretation of the results, and writing the article.
Human Participation Protection Ethical clearance was obtained for the survey from the Government of Zimbabwe’s Ministry of Public Service Labor, and Social Welfare, the Ministry of Education, Sports and Culture, and the National AIDS Council.
References
- 1.UNAIDS, UNICEF, USAID. Children on the Brink 2004. Washington, DC: TvT Associates; 2004.
- 2.Barnett T, Whiteside A. AIDS in the 21st Century: Disease and Globalization. Basingstoke, England: Palgrave MacMillan; 2002.
- 3.Gilborn LZ, Nyonyintono R, Kabumbuli R, Jagwe-Wadda G. Making a difference for children affected by AIDS: baseline findings from operations research in Uganda. Horizons Baseline Report. Washington, DC: Population Council; 2001.
- 4.Foster G. Beyond education and food: psychosocial well-being of orphans in Africa. Acta Paediatrica. 2002;91:502–504. [DOI] [PubMed] [Google Scholar]
- 5.Levine C. Orphans of the HIV epidemic: unmet needs in six US cities. AIDS Care. 1995;7(suppl 1): S57–S62. [DOI] [PubMed] [Google Scholar]
- 6.Atwine B, Cantor-Graae E, Banjunirwe F. Psychological distress among AIDS orphans in rural Uganda. Soc Sci Med. 2005;61:555–564. [DOI] [PubMed] [Google Scholar]
- 7.Investing in Our Future: Psychosocial Support for Children Affected by AIDS: A Case Study in Zimbabwe and the United Republic of Tanzania. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS; 2001.
- 8.Providing Psychosocial Support for AIDS-Affected Children: Operations Research Informs Programmes in Zimbabwe and Rwanda. New York, NY: Population Council; 2005.
- 9.Phiri S, Webb D. The impact of HIV/AIDS on orphan programmes and policy responses. In: Andrea Cornia G, ed. AIDS, Public Policy and Child Well-Being; Florence, Italy: UNICEF; 2002:1–33.
- 10.Makame V, Ani C, Grantham-McGregor S. Psychosocial well-being of orphans in Dares-Salaam, Tanzania. Acta Paediatrica. 2002;91:459–465. [DOI] [PubMed] [Google Scholar]
- 11.Bhargava A. AIDS epidemic and the psychological well-being and school participation of Ethiopian orphans. Psychol Health Med. 2005;10:263–275. [Google Scholar]
- 12.Foster G, Williamson J. A review of current literature on the impact of HIV/AIDS on children in sub-Saharan Africa. AIDS. 2000;14(suppl 3):S275–S284. [PubMed] [Google Scholar]
- 13.Richter L, Manegold J, Pather R. Family and Community Interventions for Children Affected by AIDS. Cape Town, South Africa: Human Sciences Research Council; 2004.
- 14.Dowley L. Childhood bereavement following parental death. J Child Psychiatr. 2000;41:819–830. [PubMed] [Google Scholar]
- 15.Hosegood V, Ford K. The impact of HIV/AIDS on children’s living arrangements and migration in rural South Africa. Paper presented at: African Migration in Comparative Perspective; June 4–7, 2003; Johannesburg, South Africa.
- 16.Ansell N, Young L. Enabling households to support successful migration of AIDS orphans in southern Africa. AIDS Care. 2004;16:3–10. [DOI] [PubMed] [Google Scholar]
- 17.Punamki R. From childhood trauma to adult well-being through psychosocial assistance of Chilean families. J Community Psychol. 2001;29:281–303. [Google Scholar]
- 18.Ferguson D, Horwood LJ. Early problems and later life opportunities. J Child Psychol Psychiatr. 1998; 39:1097–1108. [PubMed] [Google Scholar]
- 19.Lightfoot M, Gwadz M. Four year behavioural outcomes of an intervention for parents living with HIV and their adolescent children. AIDS. 2003;17: 1217–1225. [DOI] [PubMed] [Google Scholar]
- 20.Bourdillon MFC. Where are the Ancestors? Changing Culture in Zimbabwe. Harare: University of Zimbabwe; 1993.
- 21.Nyamukapa CA, Gregson S. Extended family and women’s roles in safeguarding orphans’ education in AIDS-afflicted rural Zimbabwe. Soc Sci Med. 2005;60: 2155–2167. [DOI] [PubMed] [Google Scholar]
- 22.Foster G, Shakespeare R, Chinemana F, et al. Orphan prevalence and extended family care in a peri-urban community in Zimbabwe. AIDS Care. 1995;7: 3–17. [DOI] [PubMed] [Google Scholar]
- 23.Kelly MJ. The Encounter Between HIV/AIDS and Education. Harare, Zimbabwe: United Nations Educational, Scientific and Cultural Organization; 2000.
- 24.UNICEF. Technical Consultations on Indicators Development for Children Orphaned and Made Vulnerable by HIV/AIDS: Guidelines for Sampling Orphans and Other Vulnerable Children. 2–4 April, 2003 Gabarone, Botswana; UNICEF; 2003.
- 25.Survey on Orphans and Other Vulnerable Children in Rural and Urban High Density Zimbabwe 2004/2005: Baseline Survey for the Government of Zimbabwe and UNICEF Country Programme in 21 Districts. Harare, Zimbabwe: UNICEF; 2005.
- 26.Watts H, Lopman B, Nyamukapa CA, Gregson S. Rising incidence and prevalence of orphanhood in Manicaland, Zimbabwe, 1998 to 2003. AIDS. 2005; 19:717–725. [DOI] [PubMed] [Google Scholar]
- 27.Beck AT, Ward CM, Mendelson M, Mock JE, Erbaugh JK. An inventory for measuring depression. Arch Gen Psychiatr. 1961;4:561–571. [DOI] [PubMed] [Google Scholar]
- 28.Kendall PC, Hollon SD, Beck AT, Hammen CL, Ingram RE. Issues and recommendations regarding use of the Beck Depression inventory. Cognit Ther Res. 1997;11:289–299. [Google Scholar]
- 29.Hays RD, Sherbourne CD, Mazel RM. The RAND 36-item health survey 1.0. Health Econ. 1993;2: 217–227. [DOI] [PubMed] [Google Scholar]
- 30.Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991 Profile. Burlington: University of Vermont; 1991.
- 31.Gilborn L, Apicella L, Brakarsh L, et al. Orphans and vulnerable youth in Bulawayo, Zimbabwe: an exploratory study of psychosocial well-being and psychosocial support. Horizons Final Report. Washington, DC: Population Council; 2006.
- 32.Kortmann F. Psychiatric case finding in Ethiopia: shortcomings of the self-reporting questionnaire. Cult Med Psychiatry. 1990;14:381–391. [DOI] [PubMed] [Google Scholar]
- 33.de Jong JTVM. A Descent into African Psychiatry. Amsterdam, The Netherlands: Royal Tropical Institute; 1987.
- 34.World Health Organization. A User’s Guide to the Self-Reporting Questionnaire. Geneva, Switzerland: Division of Mental Health, World Health Organization; 1994.
- 35.Thurman TR, Snider L, Boris N, et al. Psychosocial support and marginalization of youth-headed households in Rwanda. AIDS Care. 2006;18(3): 220–229. [DOI] [PubMed] [Google Scholar]
- 36.Kline P. An Easy Guide to Factor Analysis. London, England: Routledge; 1994.
- 37.Nunnally JC. Psychometric Theory. New York, NY: McGraw Hill; 1979.
- 38.Rutstein SO, Johnson K. The DHS Wealth Index. DHS Comparative Reports No. 6. Bethesda, Md; ORC Macro; 2004.
- 39.Zimbabwe National HIV and AIDS Estimates 2005. Harare: Zimbabwe Ministry of Health and Child Welfare; 2005.
- 40.Nyamukapa CA. Psychosocial disorders in orphans and vulnerable children in Zimbabwe. Paper presented at: Zimbabwe National OVC Research Conference; April 23–27, 2006; Harare, Zimbabwe.
- 41.Evidence for HIV Decline in Zimbabwe: A Comprehensive Review of the Epidemiological Data. Geneva, Switzerland; UNAIDs; 2005.
- 42.Gregson S, Nyamukapa CA, Garnett GP, et al. HIV infection and reproductive health in teenage women orphaned and made vulnerable by AIDS in eastern Zimbabwe. AIDS Care. 2005;17:785–794. [DOI] [PubMed] [Google Scholar]
- 43.Birdthistle I, Glynn JR, Floyd S, et al. From affected to infected? Understanding the sexual health risks to adolescent girls affected by AIDS in urban Zimbabwe. Paper presented at: 16th Biennial Meeting of the International Society for Sexually Transmitted Disease Research; July 16, 2005; Amsterdam, Netherlands.