

Abstract
PURPOSE
To describe population and survival characteristics in non-vitamin, non-mineral (NVNM) supplement users in a population-based cohort study.
METHODS
People from 43 to 86 years of age living in Beaver Dam, Wisconsin participated in a baseline examination in 1988–1990 (n=4,926) and three follow-up examinations at 5-year intervals (n=3,722, 2,962, 2,375 at each prospective examination). Medication and supplement use, medical and lifestyle factors were collected during the examination and survival was monitored through 2002.
RESULTS
NVNM supplement use increased from 5% at baseline, to 6% at the second, to 21% at the third to 30% at the fourth examination. In general, younger age, vitamin or mineral use, and taking more medications was directly related to NVNM supplement use, while current smoking and history of other systemic diseases (e.g., cardiovascular disease, cancer) was inversely related to NVNM supplement use. After adjusting for age, sex, and other medical and lifestyle factors, users of NVNM supplements had lower mortality (hazard ratio=0.74, 95% confidence interval: 0.57, 0.95, p=0.02) than non-users.
CONCLUSIONS
NVNM supplement users had a healthier lifestyle and fewer co-morbid medical conditions and were more likely to survive after adjusting for these factors than non-users.
Keywords: complementary and alternative medicine; herbal; longitudinal; non-vitamin, non-mineral; population-based; survival
Use of non-vitamin, non-mineral (NVNM) supplements is increasing;1–3 estimates of the prevalence of use since 1988 in the United States have ranged from 3% to 33% with higher prevalence shown in more recent studies.2–14 Differences in definition of NVNM supplements, population demographics, and year of study make these estimates difficult to compare. Studies suggest that these supplements are most often used as a complement to conventional medical care in the United States.13,15 The majority of studies have found that users compared to non-users of NVNM supplements have a healthier lifestyle (e.g., non-smoking, exercising, consuming a “healthy” diet).5,9,12,13 Prevalence of NVNM supplement use has been shown to be higher in women,5,9,13 middle versus young or old age,5,9,12,13 and among persons living in the West or Midwest versus other parts of the United States.7
The aforementioned studies lacked follow-up information to monitor changes in usage over time. Also, there are no known population-based studies investigating survival among users versus non-users of NVNM supplements. We have the opportunity to investigate changes in prevalent use of these supplements, as well as possible changes in associations of such use with demographic and personal characteristics, among users and non-users of NVNM supplements at four examination phases coursing over 15 years in a population-based cohort study. In addition, we investigate survival associated with such use over this interval.
MATERIALS AND METHODS
Population
A private census of Beaver Dam, Wisconsin, was performed in 1987–1988 to identify all eligible residents.16 Of the 5,924 eligible, 4,926 (83%) persons 43–86 years of age participated in the baseline examination in 1988–1990. Ninety-nine percent of the population was white and 56% were female. The cohort was re-examined at 5- (n=3,722), 10- (n=2,962), and 15-year (n=2,375) follow-up examinations. There was greater than 80% participation among survivors at each examination.16–19 Differences between participants and non-participants have been presented elsewhere.16–19 In general, participants at each examination phase were younger, had lower blood pressure, and had fewer co-morbid conditions than non-participants. All data were collected with Institutional Review Board approval from the University of Wisconsin-Madison in conformity with all federal and state laws, and the study was in adherence to the tenets of the Declaration of Helsinki.
Procedures
Participants were examined at the study suite in a local hospital, nursing home, or in their homes. The same protocols for measurements relevant to this investigation were used at each examination.20 Height, weight, and blood pressures were measured. Non-fasting blood specimens were collected for measurement of serum cholesterol (total and high density lipoprotein [HDL]) and measurement of serum glucose and glycosylated hemoglobin to aid in defining diabetes status.20 Medical and lifestyle information was obtained at a face-to-face interview.
All medications and supplements (prescription and over the counter) currently being taken by the participant were brought to the examination. The generic (or active ingredient) or brand name was recorded separately for regular (at least once per week) and occasional use (less than once per week). If medications were not brought to the examination, a follow-up telephone call was made. Non-vitamin, non-mineral supplements included herbal preparations and other botanicals, amino acids, other dietary supplements not approved by the Food and Drug Administration, or any combination of the above with other supplements.21 The majority of NVNM supplements were taken at least once per week. We include occasional use (less than once per week) in our definition because exclusion of this category did not alter the results (data not shown).
Deaths were confirmed with cause of death information obtained through matching to the Wisconsin Department of Health and Family Services or the National Death Index for all known deaths as well as persons with whom we had lost contact. We ascertained mortality between the baseline examination and December 31, 2002.
Statistics
Frequencies, t-tests, chi-squared tests, and logistic regression were used to calculate prevalence and associations with NVNM supplement use. In the logistic regression models, the probability of being a user of NVNM supplements was calculated. Age at the baseline examination in categories (43–54, 55–64, 65–74, and 75–86 years) and sex were included in each model. Step-wise procedures were used to determine which other variables to include in the models. For comparability, in the final models we included all covariates that were statistically significant at any of the four examinations.
Cox hazard regression was used to model survival. We incorporated the changing usage pattern of NVNM supplements and other relevant confounding variables into the modeling as follows. First, separate models were used to model each 5-year interval between examination phases (i.e., baseline until the time of the 5-year follow-up; 5-year follow-up to the time of the 10-year follow-up; and 10-year follow-up until death or censoring at the end of December 2002). The covariates were updated to their current values at the start of each interval using time-varying covariate techniques.22 Specifically, these models were combined into a single model using a strata variable for the 5-year interval in the PHREG procedure of SAS version 9.1.23 Models first controlled for age (continuous) and sex and then were further adjusted for vitamin and mineral use, history of arthritis, cardiovascular disease, emphysema, smoking, cancer, diabetes, level of education, body mass index (<25, 25–29.9, 30+ kg/m2), systolic blood pressure, sedentary lifestyle, and total to HDL cholesterol. SAS, version 9 was used for all analyses.23
RESULTS
Prevalence of use of NVNM supplements
The prevalence of use of NVNM supplements increased from 5% at the 1988–1990 examination to 30% at the 2003–2005 examination (Table 1). Lecithin, garlic, omega-3 fatty acids, ginseng, glucosamine, ginkgo biloba, and saw palmetto were the most commonly used NVNM supplements. Use of lecithin remained fairly consistent at each examination, while all other NVNM supplements had increased use at later examinations. At the 1988–1990 and 1993–1995 examination, garlic and lecithin were the most commonly used NVNM supplements. At the 1998–2000 examination, garlic remained the most commonly used NVNM supplement, but glucosamine, ginkgo biloba, and ginseng were now more commonly used than lecithin. Increasing use of glucosamine and omega-3 fatty acids continued at the 2003–2005 examination.
Table 1.
Prevalence of non-vitamin, non-mineral supplements at four examination phases in the Beaver Dam Eye Study.
| 1988–1990
% (N=4,926) |
1993–1995
% (N=3,722) |
1998–2000
% (N=2,962) |
2003–2005
% (N=2,375) |
|
|---|---|---|---|---|
| Any NVNM supplement* | 5.3 | 6.3 | 20.5 | 30.3 |
| Lecithin | 1.6 | 1.6 | 1.8 | 1.7 |
| Garlic | 1.0 | 2.7 | 6.1 | 5.5 |
| Omega-3 fatty acid | 0.3 | 0.3 | 1.0 | 5.8 |
| Ginseng | 0.2 | 0.5 | 2.0 | 1.9 |
| Glucosamine | 0 | 0 | 5.4 | 13.2 |
| Ginkgo biloba | 0 | 0.2 | 4.3 | 2.9 |
| Saw Palmetto | 0 | 0.1 | 1.5 | 2.3 |
Abbreviations: N=number of participants at each examination phase; NVNM=non-vitamin, non-mineral
NVNM supplements included herbal preparations and other botanicals, amino acids, other dietary supplements not approved by the Food and Drug Administration, or any combination of the above with other supplements.
Cross-sectional associations
Unadjusted population characteristics at each examination by NVNM use are shown in Table 2. In this crude analysis, younger age was associated with NVNM use at the last two examinations. Women used NVNM supplements more frequently than men, but the association was only significantly different at the last two examinations. Persons with higher household income and more education were more likely to use NVNM supplements at the last two examinations, but not at earlier examinations. Vitamin and mineral use and taking more medications were associated with NVNM use at all examinations. A history of sedentary behavior, currently smoking, and hypertension were less likely to be associated with taking NVNM supplements at most examinations. Few other consistently significant patterns occurred for other characteristics (Table 2).
Table 2.
Crude (unadjusted) population characteristics by non-vitamin, non-mineral supplement use at all four examinations in the Beaver Dam Eye Study.
| Variable | 1988–1990 Examination | 1993–1995 Examination | 1998–2000 Examination | 2003–2005 Examination | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Not taking
(N=4,665) |
Taking
(N=261) |
p* | Not taking
(N=3,487) |
Taking
(N=235) |
p* | Not taking
(N=2,354) |
Taking
(N=608) |
p* | Not taking
(N=1,656) |
Taking
(N=719) |
p* | |
| Age, mean years | 62.0 | 62.5 | 0.48 | 65.2 | 65.8 | 0.41 | 69.3 | 67.8 | <0.01 | 72.6 | 70.4 | <0.01 |
| Gender, % men | 44.2 | 39.1 | 0.11 | 43.4 | 41.7 | 0.63 | 42.8 | 38.7 | 0.07 | 42.7 | 38.1 | 0.04 |
| Total Household Income | ||||||||||||
| <20 thousand, % | 44.1 | 44.3 | 0.83 | 34.6 | 40.1 | 0.60 | 28.7 | 23.7 | 0.02 | 27.0 | 21.9 | <0.01 |
| 20–44 thousand, % | 40.7 | 41.4 | 42.2 | 34.1 | 40.6 | 42.3 | 41.5 | 41.1 | ||||
| ≥ 45 thousand, % | 15.2 | 14.3 | 23.1 | 25.8 | 30.7 | 34.0 | 31.5 | 37.0 | ||||
| More than high school education, % | 27.4 | 27.3 | 0.99 | 30.3 | 29.5 | 0.83 | 31.6 | 38.1 | <0.01 | 34.6 | 38.9 | 0.05 |
| Married, % | 71.4 | 69.3 | 0.48 | 67.6 | 67.2 | 0.94 | 64.0 | 65.6 | 0.48 | 60.3 | 65.2 | 0.02 |
| Taking vitamins, % | 31.7 | 82.8 | <0.01 | 46.3 | 85.5 | <0.01 | 61.9 | 88.3 | <0.01 | 67.3 | 90.5 | <0.01 |
| Taking minerals, % | 32.7 | 76.6 | <0.01 | 37.9 | 71.5 | <0.01 | 49.7 | 74.7 | <0.01 | 58.2 | 80.8 | <0.01 |
| Number of medications, mean | 3.9 | 6.1 | <0.01 | 4.4 | 6.8 | <0.01 | 5.9 | 7.5 | <0.01 | 7.6 | 8.9 | <0.01 |
| Sedentary lifestyle, % | 77.0 | 70.1 | 0.01 | 74.0 | 68.1 | 0.06 | 75.0 | 69.0 | <0.01 | 71.3 | 62.4 | <0.01 |
| Body mass index, mean kg/m2 | 28.8 | 28.3 | 0.21 | 29.5 | 29.5 | 0.97 | 29.8 | 30.1 | 0.16 | 30.1 | 30.7 | 0.04 |
| Ever heavy drinker, % | 17.4 | 11.9 | 0.02 | 17.1 | 16.2 | 0.79 | 15.3 | 13.1 | 0.20 | 12.5 | 14.2 | 0.26 |
| Current smoker, % | 20.1 | 13.0 | <0.01 | 15.0 | 11.5 | 0.15 | 10.6 | 6.6 | <0.01 | 10.0 | 5.6 | <0.01 |
| Hypertension, % | 50.9 | 45.0 | 0.06 | 51.2 | 50.6 | 0.89 | 61.0 | 55.1 | <0.01 | 66.9 | 62.4 | 0.04 |
| Serum cholesterol ≥ 240 mg/dL, % | 42.0 | 40.6 | 0.70 | 45.6 | 49.6 | 0.25 | 22.1 | 24.7 | 0.20 | N/A | ||
| History of arthritis, % | 38.3 | 43.6 | 0.10 | 42.6 | 42.7 | 0.99 | 43.9 | 52.3 | <0.01 | 47.6 | 60.0 | <0.01 |
| Other systemic disease†, % | 49.9 | 50.2 | 0.95 | 52.7 | 50.6 | 0.54 | 58.0 | 53.9 | 0.07 | 59.7 | 59.1 | 0.78 |
Abbreviations: N=number of participants at each examination phase; N/A = not available at the particular examination
t-test for continuous (mean) and chi-squared test for categorical (percent) variables
includes history of angina, stroke, myocardial infarction, cancer, diabetes, gout, thyroid disease, ulcer or emphysema
All variables in Table 2 were entered into logistic regression models and step-wise procedures were used to determine significant associations with NVNM supplement use. The final models include all variables that were significant (p<0.05) at any of the four examinations (Table 3). At the 1988–1990 (baseline) examination, NVNM use was significantly and directly associated with use of vitamins, minerals, number of other medications used and inversely associated with a history of cigarette smoking or having other chronic medical conditions (e.g., gout, cardiovascular disease). At the 1993–1995 (second) examination, NVNM use was directly associated with use of vitamins and number of other medications used and inversely associated with being a woman or having chronic medical conditions. At the 1998–2000 (third) examination, NVNM use was directly associated with use of vitamins, minerals, number of other medications used, history of arthritis and inversely with age, a history of currently smoking, hypertension, or having other chronic medical conditions. At the 2003–2005 (fourth) examination, NVNM use was directly associated with use of vitamins, minerals, number of other medications used, history of arthritis, history of heavy drinking and inversely associated with age, a history of sedentary behavior, currently smoking, or hypertension. Other variables listed in Table 2 were not significant in the multivariate models (data not shown).
Table 3.
Multivariate logistic regression model for cross-sectional associations with non-vitamin, non-mineral supplement use at each examination in the Beaver Dam Eye Study.
| Variable | 1988–1990 | 1993–1995 | 1998–2000 | 2003–2005 | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
|
| ||||||||
| Age at 1988–1990 exam | ||||||||
| 75–86 vs 43–54 years | 0.94 | 0.62, 1.43 | 0.72 | 0.41, 1.25 | 0.49 | 0.30, 0.79† | 0.19 | 0.09, 0.42† |
| 65–74 vs 43–54 years | 0.71 | 0.48, 1.04 | 1.13 | 0.77, 1.66 | 0.73 | 0.56, 0.96† | 0.43 | 0.32, 0.57† |
| 55–64 vs 43–54 years | 1.01 | 0.71, 1.43 | 1.10 | 0.77, 1.58 | 1.11 | 0.88, 1.39 | 0.87 | 0.70, 1.07 |
| Women vs Men | 0.75 | 0.56, 1.02 | 0.73 | 0.53, 1.00† | 0.96 | 0.77, 1.19 | 1.03 | 0.84, 1.28 |
| Taking vitamins | 5.32 | 3.53, 8.01† | 4.31 | 2.64, 7.04† | 2.88 | 2.12, 3.93† | 3.05 | 2.21, 4.20† |
| Taking minerals | 1.94 | 1.33, 2.83† | 1.18 | 0.80, 1.74 | 1.54 | 1.21, 1.97† | 1.61 | 1.25, 2.09† |
| Number of medications | 1.09 | 1.04, 1.14† | 1.16 | 1.11, 1.21† | 1.06 | 1.03, 1.10† | 1.03 | 1.00, 1.06† |
| Sedentary lifestyle | 0.84 | 0.63, 1.12 | 0.82 | 0.60, 1.11 | 0.87 | 0.71, 1.08 | 0.81 | 0.66, 0.99† |
| Ever heavy drinker | 0.69 | 0.45, 1.05 | 1.04 | 0.69, 1.57 | 0.96 | 0.71, 1.29 | 1.38 | 1.02, 1.85† |
| Smoking history | ||||||||
| current vs never | 0.70 | 0.46, 1.06 | 0.75 | 0.46, 1.20 | 0.64 | 0.44, 0.95† | 0.52 | 0.35, 0.77† |
| past vs never | 0.87 | 0.64, 1.18 | 0.86 | 0.62, 1.18 | 1.07 | 0.86, 1.31 | 0.92 | 0.75, 1.13 |
| Hypertension | 0.78 | 0.59, 1.02 | 0.87 | 0.65, 1.16 | 0.74 | 0.60, 0.90† | 0.77 | 0.62, 0.94† |
| History of arthritis | 1.01 | 0.76, 1.34 | 0.78 | 0.58, 1.05 | 1.36 | 1.11, 1.66† | 1.68 | 1.38, 2.05† |
| Other systemic disease* | 0.73 | 0.54, 0.97† | 0.60 | 0.45, 0.82† | 0.70 | 0.57, 0.86† | 0.96 | 0.78, 1.18 |
Abbreviations: OR=odds ratio; CI=confidence interval
includes history of angina, stroke, myocardial infarction, cancer, diabetes, gout, thyroid disease, ulcer or emphysema
p<0.05
Associations with Survival
About 32% (n=1,576) of the baseline population had died prior to December 31, 2002. Within each 5-year interval, after controlling for age and sex, the hazard for dying was lower for users of NVNM supplements than non-users but was only statistically significant from the 5 to 10-year interval (Figure 1). Combining these intervals into a single model, NVNM use was associated with a significant reduction in mortality, after controlling for age and sex (hazard ratio [HR]=0.73, 95 percent confidence interval [CI]: 0.58, 0.91). The magnitude of the relationship was similar after multivariate adjustment for other lifestyle and medical factors (HR=0.74, 95 percent CI: 0.57, 0.95).
Figure 1.
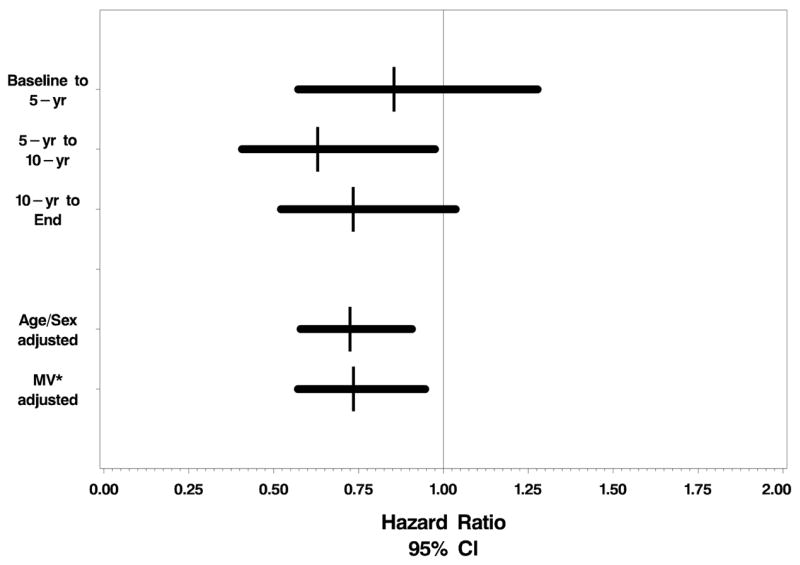
Associations of non-vitamin, non-mineral (NVNM) supplement use with all cause-mortality. Age and sex adjusted hazard ratios and 95 percent confidence intervals are plotted for each interval between examinations and then combined together using a time-varying covariate approach (see statistical methods section for complete details). A final multivariate model is presented in the bottom row.
* MV: multivariate adjusted for age (continuous), sex, vitamin and mineral use, history of arthritis, cardiovascular disease, emphysema, smoking, cancer, diabetes, level of educational attainment, body mass index (<25, 25–29.9, 30+ kg/m2), systolic blood pressure, sedentary lifestyle behavior, and total to high density lipoprotein serum cholesterol.
We investigated the most common specific NVNM supplements and their associations with survival using a similar modeling approach. There were no significant relationships with any of the specific NVNM supplements (Figure 2). However the hazard ratios were less than 1 for all supplements except for ginseng and omega-3 fatty acids.
Figure 2.
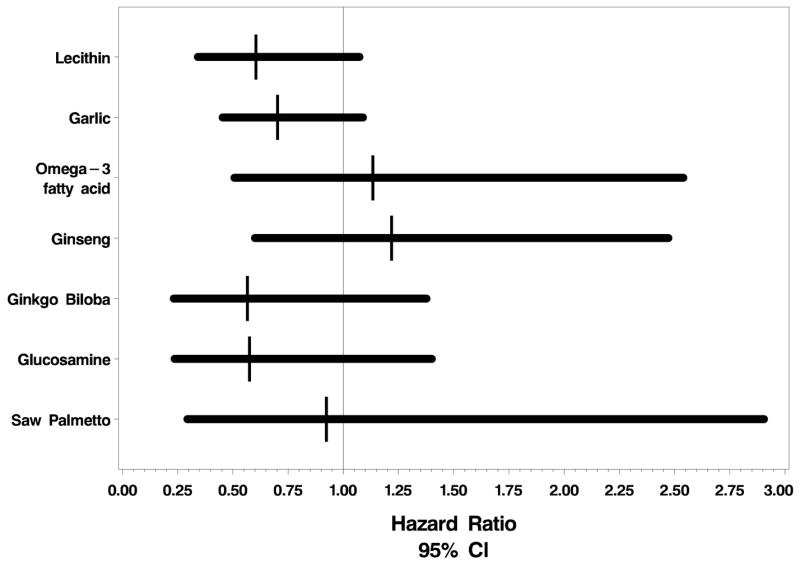
Associations of the most common reported non-vitamin, non-mineral (NVNM) supplements with all cause-mortality. Multivariate adjusted hazard ratios and 95 percent confidence intervals combining the hazards from each 5-year interval (see statistical methods) are plotted. The models adjusted for age (continuous), sex, vitamin and mineral use, history of arthritis, cardiovascular disease, emphysema, smoking, cancer, diabetes, level of educational attainment, body mass index (<25, 25–29.9, 30+ kg/m2), systolic blood pressure, sedentary lifestyle behavior, and total to high density lipoprotein serum cholesterol.
DISCUSSION
In this study of adults aged 43–86 years at baseline, we found an increase from 5% at baseline to 6% at the second to 21% at the third to 30% at the fourth examination in use of NVNM supplements. We found the greatest increase in NVNM use occurred at the examination following the adoption of the Dietary Supplement Health and Education Act of 1994 which permitted herbal products, vitamins, and minerals to be regulated as foods and not be subject to criteria for drug or food additive approval.21,24 Low prevalence of use of these supplements prior to this Act has also been shown by Eisenberg.4 We are unaware of studies with data collected after 2002 to compare with the prevalence of 30% that we found at the 2003–2005 examination in this study. Nevertheless, it seems likely from this and other studies1,3,4 that use of NVNM supplements is continuing to rise. Since relative risks and benefits of use of these preparations are not well defined, further study of persons using these preparations is warranted.
At the first two examinations, there were relatively few users. That, in part, may account for the relatively few significant associations we found compared to the findings for the last two examinations. However, there were similar odds ratios among the four visits for many of the factors correlated with NVNM use (e.g., more frequent use of vitamins, minerals, and other medications and less frequent use in those with a history of currently smoking and those with hypertension and chronic medical conditions other than a history of arthritis). We did not find a consistent association of higher NVNM use in women compared to men, while others have reported such an association.5,9,13 Also, while self-reported income and higher educational attainment have been associated with use in other studies,3,9,12,13 neither was significant in multivariable analyses in our study. It is possible that persons of other ethnicities or cultures or socio-economic status are more (or less) likely to use NVNM supplements than in the Beaver Dam population.
Similar to findings of use of Complementary and Alternative Medicines (CAM),1,3,25 a broader class of therapies that includes NVNM supplements, younger age was associated with use. We did not obtain information on reasons for use, so we can only speculate as to the reasons behind the age effect. There may have been greater exposure to advertising of NVNM supplements to younger persons. Persons with systemic chronic conditions were less likely to be NVNM users, and these persons were likely to be older. In a recent study, Wheaton reported that the majority of persons using these supplements were using them to maintain health rather than to treat or prevent illness.13 This may suggest that persons with systemic conditions may not be using NVNM supplements because of the lack of efficacy of such treatment for their medical conditions.
There are likely to be different reasons for use of the specific NVNM supplements. For example, persons with joint or skeletal complaints due to arthritis may be taking glucosamine for their symptoms,26 while those who take omega-3 fatty acids may take these preparations to prevent cardiovascular disease.27 The (inferred) reasons may be a combination of these as, for example, garlic has been touted as a prevention and a treatment for hypertension and atherosclerotic heart disease.28
We found that users of vitamins and minerals were more likely to use NVNM supplements suggesting that these persons may be more health conscious than non-users. The finding of better survival among NVNM users is consistent with this notion. It is also possible that the anti-oxidant, anti-inflammatory, and anti-platelet properties in some of the NVNM supplements may be causally related to survival. No single NVNM supplement was significantly associated with survival after multivariate adjustment, although the hazards were suggestive for some. That use of any NVNM was significantly protective may be related to additive effects of some of these preparations. An alternative explanation is that unmeasured lifestyle exposures rather than biological actions of the supplements may be the important protective exposures. Great caution should be taken as this finding should not be interpreted as causal.
Strengths of this study include a high participation rate (>80% at all examinations), large sample size, longitudinal follow-up, and unbiased data collection methods. A possible limitation is that the population under study is from a Midwestern community of mostly Caucasian Americans, and this may have influenced our findings, although we cannot be sure that the frequency of use of NVNM and the relationships we found are associated with living in a rural community or with a specific ethnicity. Other limitations are that information on dose and duration of NVNM use and reasons for use were not obtained and these may influence the results we report.
In summary, NVNM supplement use has drastically increased in prevalence from 5% in 1988–2000 to 30% in 2003–2005, and in general, users of NVNM supplements had a healthier profile and were more likely to survive than non-users.
Acknowledgments
Supported by National Institutes of Health grant EY06594 (R. Klein, B.E.K. Klein).
Abbreviations
- NVNM
non-vitamin, non-mineral
- HDL
high density lipoprotein
- HR
hazard ratio
- CI
confidence interval
- CAM
complementary and alternative medicines
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Kessler RC, Davis RB, Foster DF, Van Rompay MI, Walters EE, Wilkey SA, et al. Long-term trends in the use of complementary and alternative medical therapies in the United States. Ann Intern Med. 2001;135:262–268. doi: 10.7326/0003-4819-135-4-200108210-00011. [DOI] [PubMed] [Google Scholar]
- 2.Ervin RB, Wright JD, Reed-Gillette D. Prevalence of leading types of dietary supplements used in the Third National Health and Nutrition Examination Survey, 1988--94. Adv Data. 2004:1–7. [PubMed] [Google Scholar]
- 3.Tindle HA, Davis RB, Phillips RS, Eisenberg DM. Trends in use of complementary and alternative medicine by US adults: 1997–2002. Altern Ther Health Med. 2005;11:42–49. [PubMed] [Google Scholar]
- 4.Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, et al. Trends in alternative medicine use in the United States, 1990–1997: results of a follow-up national survey. JAMA. 1998;280:1569–1575. doi: 10.1001/jama.280.18.1569. [DOI] [PubMed] [Google Scholar]
- 5.Radimer KL, Subar AF, Thompson FE. Nonvitamin, nonmineral dietary supplements: issues and findings from NHANES III. J Am Diet Assoc. 2000;100:447–454. doi: 10.1016/S0002-8223(00)00137-1. [DOI] [PubMed] [Google Scholar]
- 6.Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medication use in the ambulatory adult population of the United States: the Slone survey. JAMA. 2002;287:337–344. doi: 10.1001/jama.287.3.337. [DOI] [PubMed] [Google Scholar]
- 7.Ni H, Simile C, Hardy AM. Utilization of complementary and alternative medicine by United States adults: results from the 1999 national health interview survey. Med Care. 2002;40:353–358. doi: 10.1097/00005650-200204000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Rafferty AP, McGee HB, Miller CE, Reyes M. Prevalence of complementary and alternative medicine use: state-specific estimates from the 2001 Behavioral Risk Factor Surveillance System. Am J Public Health. 2002;92:1598–1600. doi: 10.2105/ajph.92.10.1598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Schaffer DM, Gordon NP, Jensen CD, Avins AL. Nonvitamin, nonmineral supplement use over a 12-month period by adult members of a large health maintenance organization. J Am Diet Assoc. 2003;103:1500–1505. doi: 10.1016/j.jada.2003.08.026. [DOI] [PubMed] [Google Scholar]
- 10.Bent S, Ko R. Commonly used herbal medicines in the United States: a review. Am J Med. 2004;116:478–485. doi: 10.1016/j.amjmed.2003.10.036. [DOI] [PubMed] [Google Scholar]
- 11.Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004:1–19. [PubMed] [Google Scholar]
- 12.Yu SM, Ghandour RM, Huang ZJ. Herbal supplement use among US women, 2000. J Am Med Womens Assoc. 2004;59:17–24. [PubMed] [Google Scholar]
- 13.Wheaton AG, Blanck HM, Gizlice Z, Reyes M. Medicinal herb use in a population-based survey of adults: prevalence and frequency of use, reasons for use, and use among their children. Ann Epidemiol. 2005;15:678–685. doi: 10.1016/j.annepidem.2004.09.002. [DOI] [PubMed] [Google Scholar]
- 14.Kronenberg F, Cushman LF, Wade CM, Kalmuss D, Chao MT. Race/ethnicity and women’s use of complementary and alternative medicine in the United States: results of a national survey. Am J Public Health. 2006;96:1236–1242. doi: 10.2105/AJPH.2004.047688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Druss BG, Rosenheck RA. Association between use of unconventional therapies and conventional medical services. JAMA. 1999;282:651–656. doi: 10.1001/jama.282.7.651. [DOI] [PubMed] [Google Scholar]
- 16.Klein R, Klein BE, Linton KL, De Mets DL. The Beaver Dam Eye Study: visual acuity. Ophthalmology. 1991;98:1310–1315. doi: 10.1016/s0161-6420(91)32137-7. [DOI] [PubMed] [Google Scholar]
- 17.Klein R, Klein BE, Lee KE. Changes in visual acuity in a population. The Beaver Dam Eye Study Ophthalmology. 1996;103:1169–1178. doi: 10.1016/s0161-6420(96)30526-5. [DOI] [PubMed] [Google Scholar]
- 18.Klein R, Klein BE, Lee KE, Cruickshanks KJ, Chappell RJ. Changes in visual acuity in a population over a 10-year period: The Beaver Dam Eye Study. Ophthalmology. 2001;108:1757–1766. doi: 10.1016/s0161-6420(01)00769-2. [DOI] [PubMed] [Google Scholar]
- 19.Klein R, Klein BE, Lee KE, Cruickshanks KJ, Gangnon RE. Changes in visual acuity in a population over a 15-year period: The Beaver Dam Eye Study. Am J Ophthalmol. 2006;142:539–549. doi: 10.1016/j.ajo.2006.06.015. [DOI] [PubMed] [Google Scholar]
- 20.Klein R, Klein BE. The Beaver Dam Eye Study. Manual of Operations. US Department of Commerce; Springfield, VA: 1991. NTIS Accession No. PB91–149823; [Google Scholar]
- 21.Dietary supplement health and education act of 1994. Pub L No. 103–417, 108 Stat. 4325 (October 25, 1994).
- 22.Allison PD. Survival analysis using the SAS® system: a practical guide. Cary, NC: SAS Institute Inc.; 1995. pp. 138–161. [Google Scholar]
- 23.SAS Institute Inc. SAS/STAT User’s Guide, Version 9. Cary, NC: SAS Institute Inc; 2004. [Google Scholar]
- 24.Taylor DA. Botanical supplements: weeding out the health risks. Environ Health Perspect. 2004;112:A750–A753. doi: 10.1289/ehp.112-a750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Graham RE, Ahn AC, Davis RB, O’Connor BB, Eisenberg DM, Phillips RS. Use of complementary and alternative medical therapies among racial and ethnic minority adults: results from the 2002 National Health Interview Survey. J Natl Med Assoc. 2005;97:535–545. [PMC free article] [PubMed] [Google Scholar]
- 26.McAlindon TE, LaValley MP, Gulin JP, Felson DT. Glucosamine and chondroitin for treatment of osteoarthritis: a systematic quality assessment and meta-analysis. JAMA. 2000;283:1469–1475. doi: 10.1001/jama.283.11.1469. [DOI] [PubMed] [Google Scholar]
- 27.Thies F, Garry JM, Yaqoob P, Rerkasem K, Williams J, Shearman CP, et al. Association of n-3 polyunsaturated fatty acids with stability of atherosclerotic plaques: a randomised controlled trial. Lancet. 2003;361:477–485. doi: 10.1016/S0140-6736(03)12468-3. [DOI] [PubMed] [Google Scholar]
- 28.Rahman K. Garlic and aging: new insights into an old remedy. Ageing Res Rev. 2003;2:39–56. doi: 10.1016/s1568-1637(02)00049-1. [DOI] [PubMed] [Google Scholar]