

A 70-year-old woman receiving long-term corticosteroid therapy for sarcoidosis presented with hip pain. She underwent whole-body technetium 99m methylene diphosphonate bone scintigraphy to exclude avascular necrosis of the femoral head. Although there was no suggestion of avascular necrosis, multiple areas of increased activity were present in the axial and proximal appendicular skeleton (Figure 1). We were concerned that these findings suggested multiple skeletal metastases. A computed tomography scan of her chest showed bilateral pulmonary opacities and an infiltrating process involving the mediastinum and both hila (Figure 2). A computed tomography scan of her abdomen identified splenomegaly and lymphadenopathy. Our differential diagnosis included small-cell lung cancer, sarcoma, lymphoma and infection.
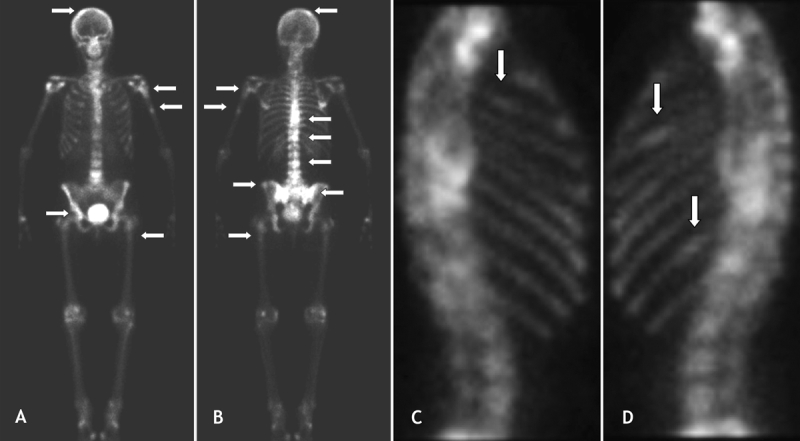
Figure 1: Technetium 99m methylene diphosphonate bone scintigraphy to exclude avascular necrosis of the femoral head in a 70-year-old woman who had hip pain and had been receiving long-term corticosteroid therapy. Whole-body (A, anterior, and B, posterior) and chest (C, right lateral, and D, left lateral) bone scintigraphy show focal areas of increased uptake (arrows) in the mid-to-lower thoracic spine, the lower lumbar spine, both sacroiliac joints, the right calvarium, the proximal and mid left humerus, bilateral ribs, the right acetabulum and the proximal shaft of the left femur.
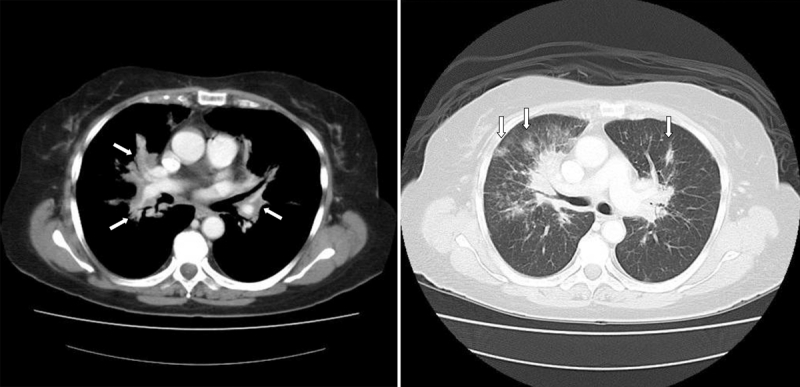
Figure 2: Computed tomography scan of the chest on mediastinal window (left) showing a diffuse infiltrative process involving the mediastinum and both pulmonary hila (arrows). Lung windows (right) demonstrate multiple pulmonary opacities in both lungs (arrows).
The patient had received a diagnosis of sarcoidosis 5 years earlier when she presented with lymphadenopathy and night sweats. The initial workup included a computed tomography scan that showed lymphadenopathy and an axillary lymph-node biopsy that revealed noncaseating granulomata (Appendix 1, available at www.cmaj.ca/cgi/content/full/178/2/153/DC1). The radiologist reviewing the current computed tomography scan did not receive this background information and suspected a malignant process. The patient's respirologist subsequently performed bone-marrow biopsies, which demonstrated noncaseating granulomata consistent with skeletal sarcoidosis. The patient's condition has been stable, and a repeat bone scan after 2 years of follow-up showed no change.
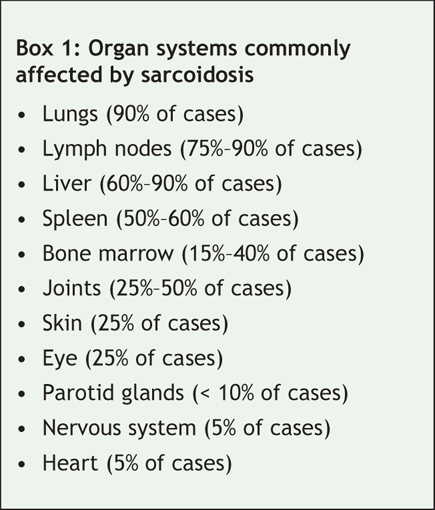
Sarcoidosis is a granulomatous disease of unknown cause that affects various organ systems (Box 1).1 The disease is diagnosed when typical clinical and radiographic manifestations are supported by histopathologic findings of noncaseating granulomata with no evidence of infection.2
Box 1.
Skeletal sarcoidosis most commonly affects the hands in the form of a coarsened trabecular pattern with cystic and marginal bone defects and sclerosis. Lesions may also develop in the skull, facial bones, spine, long tubular bones and joints; however, the imaging features are nonspecific and yield a broad differential diagnosis.3
Sundeep Singh Nijjar MD Section of Nuclear Medicine University of Manitoba William D. Leslie MD MSc Department of Internal Medicine St. Boniface General Hospital Winnipeg, Man.
@ See related article page 151
This case demonstrates a rare manifestation of sarcoidosis mimicking skeletal metastases on bone scintigraphy. It underscores the importance of providing complete clinical information to the imaging service to facilitate accurate diagnostic interpretation.
Supplementary Material
Footnotes
This article has been peer reviewed.
Competing interests: None declared.
REFERENCES
- 1.Kasper DL, Fauci AS, Longo DL, et al, editors. Harrison's principles of internal medicine. 16th ed. New York: McGraw-Hill; 2005.
- 2.Iannuzzi MC, Rybicki BA, Teirstein, AS. Sarcoidosis. N Engl J Med 2007;357:2153-65. [DOI] [PubMed]
- 3.Poyanli A, Poyanli O, Sencer S, et al. Vertebral sarcoidosis: imaging findings. Eur Radiol 2000;10:92-4. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.