An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
Treatment of oesophageal high-grade dysplasia is one of the great conundrums facing oesophageal surgeons. Both authors allude to the uncertainty of the natural history of high-grade dysplasia, especially the rate of progression to invasive cancer and furthermore to the variation in reported incidence of carcinoma in post oesophagectomy resections for high-grade dysplasia.
Professor Barr adopts the minimalist approach – favouring local ablative therapy (such as photodynamic therapy or endoscopic mucosal resection [EMR]) and endoscopic surveillance – postulating these inconveniences are better than death or life-long morbidity following oesophagectomy for a pathologically variable disease.
Mr Maynard quotes very impressive mortality following transhiatal oesophagectomy and rightly alludes to the fact that increasing depth of mucosal neoplasia equates to higher nodal disease with consequent reduction in survival from higher tumour stage.
What is the correct approach? Probably the answer will lie in increased use of EMR: this will enable better pretreatment staging and identification of patients with multifocal disease. Those whom are fit, have multifocal long-segment disease and with extending depths of neoplasia on EMR histology might fare best with surgical resection. The unfit with short-segment, superficial disease may suffice with endoscopic therapy/surveillance.
1Cranfield Health, Gloucestershire Royal Hospital, Gloucester, UK
✉
Correspondence to Prof. Hugh Barr, Cranfield Health, Gloucestershire Royal Hospital, Great Western Road, Gloucester GL1 3NN, UK T: +44 (0)8454 226679; F: +44 (0)8454 224813; E: hugh.barr@glos.nhs.uk
In the UK, the annual death rate from oesophageal carcinoma is now over 7000. The incidence in men has dramatically risen over the past three decades from 8.8 to 14.1 per 100,000 population, with the corresponding female rates rising from 4.8 to 5.7 per 100,000. The predominant cancer is a junctional adenocarcinoma related to columnar lined Barrett's oesophagus.1 There is intense scientific scrutiny of this most intriguing premaligant phenotype with a search for the molecular mechanisms, and high-risk groups. The management of Barrett's oesophagus and its dysplastic degeneration is the most controversial topic facing oesophagogastric surgeons and gastro-enterologists. The debate is intense as to the value of screening patients suffering from chronic reflux disease, since this will identify approximately 12% who will have Barrett's metaplasia. The divergence between the American College of Gastroenterology and the British Society of Gastroenterology is stark with the former recommending screening and latter unconvinced by the current evidence base.2 There is also controversy as to whether patients with Barrett's oesophagus should receive regular endoscopic surveillance and biopsy to detect dysplasia and early cancer. The NHS Technology Review concluded that there was insufficient evidence to assess the effectiveness of a surveillance programme.3 This has resulted in the HTA commissioning a large randomised clinical trial (Barrett's Oesophagus Surveillance Study-BOSS) and Cancer Research UK supporting a randomised chemoprevention trial (AspECT). The evidence from these trials will be vital to future treatment strategies.
Resection: the dilemmas
A management strategy of oesophageal resection, following the detection and confirmation of high-grade dysplasia is problematical to both surgeon and patient. Many surgeons feel ‘the existentialist guilt of the spectator’, being anxious to intervene, following the detection of a degenerating phenotype. This being justified since dysplasia may be a marker of co-existent cancer, and the best marker for its subsequent development. However, oesophagectomy is associated with a worrying mortality in these asymptomatic patients of 5–11%.4 Resection for high-grade dysplasia has an early and late morbidity of over 50% and 26%, respectively, with an overall 5-year survival of 79%,5 with profound deterioration in quality of life. The important question – is there an acceptable and safer alternative strategy?
Resection: the rationale for avoidance
A major problem remains that of establishing a definitive diagnosis and the natural history in that individual patient. The histopathological recognition of high-grade dysplasia remains worryingly subjective, with kappa values for intra-observer and interobserver of 0.64 and 0.43, respectively.6 It is also apparent that the natural history of dysplasia in a patient is highly variable. Some investigators report 60% developing cancer within 8 months. Others report a cumulative cancer incidence of 9% (at 5 years), with only 16% of patients developing cancer during 13.9 years of surveillance.7 Also, the diagnosis of invasive cancer presents a challenge. Even following detailed examination of oesophagectomy specimens to establish invasion into the lamina propria, the intra-observer and interobserver kappa values are 0.56 and 0.42, respectively.8 The argument that many patients with dysplasia have an occult cancer is being challenged. Overall, the prevalence following surgical resection is between 11–73%. This has resulted in the valid questioning of decisions taken following the diagnosis of high-grade dysplasia. It is possible that an intensive endoscopic search for occult cancer with endoscopic mucosal resection/biopsy is unlikely if one is already committed to oesophagectomy. The important question is, what level of uncertainty is acceptable for patients and surgeons?
Resection: realistic alternatives
Anecdotal time-line analysis of several of our patients reveals that many with high-grade dysplasia and even early cancer can be controlled with ablation techniques and careful endoscopic follow-up for 5–10 years. These types of highly observational, purely anecdotal data from many centres were the major driver for a large multicentre trial to gain the evidence base. This partially (histopathological) blinded, randomised trial used photodynamic therapy to eradicate high-grade dysplasia. Patients (208) were randomised 2:1 to endoscopic photodynamic therapy with omeprazole or received omeprazole (control) only. There was a significant difference (P < 0.0001) for photodynamic therapy (106/138; 77%) compared with control (27/70; 39%) in complete ablation of high-grade dysplasia. The occurrence of adenocarcinoma in the photodynamic group was significantly lower (P < 0.006). The response remains robust at 5-year follow-up. Although endoscopic ablation with life-long follow-up is more expensive, it is the most cost-effective solution when compared with surveillance and radical surgery at the detection of dysplasia. Oesophagectomy results in 11.82 quality-adjusted life years (QUALYs), compared with photodynamic therapy and life-long follow-up results in 12.31 QUALYs.9,10
Comparisons of 5-amino-laevulinic acid photodynamic therapy with argon plasma coagulation suggest that the thermal eradication may also be very effective.11
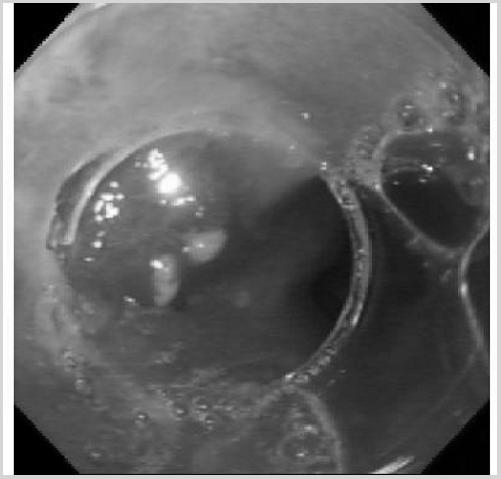
The development of endoscopic mucosal resection (Fig. 1) allows complete eradication with accurate staging of mucosal cancer. It is clear that these techniques are highly effective with a complete remission rate of 82.5% of 350 patients with Barrett's carcinoma and high-grade dysplasia (mean follow-up 12 months). The best results occurred in patients with high-grade dysplasia and small (< 20 mm) well or moderately differentiated cancers (97%).12 The major concern is that metachronous tumours can occur in up to 50% of patients in the residual Barrett's segment. Patients must, therefore, continue with careful endoscopic surveillance and have complete ablation of the metaplastic segment with photodynamic therapy or repeat endoscopic mucosal resection. Currently, optical spectroscopy techniques are being developed that will allow detection of molecular degeneration and microscopic dysplastic change in real-time. This will allow detection and destruction at one endoscopic session. These are novel and developing techniques and need further long-term assessment. Conceptually, it must be correct to eradicate local disease with minimal trauma. It is not a surgical triumph to eradicate a microscopic molecular change with the total trauma of a radical oesophagectomy.
Endoscopic picture of an area of high-grade dysplasia with an endoscopic mucosal resection cap prior to mucosectomy to eradicate disease.
Concluding comments
Many patients with high-grade dysplasia and mucosal cancer cannot tolerate radical resection and clearly can be managed with endoscopic ablation followed by surveillance. The more challenging patients are those fit for resection but with a degenerating segment of Barrett's oesophagus with multifocal dysplastic disease. I strongly suggest to the oesophagogastric surgical community that resection should now be reserved for patients with evidence of cancer. If there is high-grade dysplasia, the patient should be managed using endoscopic eradication and the entire Barrett's segment destroyed followed by life-long surveillance. The concept of minimally invasive endoscopic surgery for localised disease is appropriate, but further data are needed to ensure that the response to therapy is robust over time.
3.Garside R. Surveillance of Barrett's oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling. Health Technol Assess. 2006;10:1–158. doi: 10.3310/hta10080. [DOI] [PubMed] [Google Scholar]
4.Bachmann MO, Alderson D, Edwards D, Wotton S, Bedford C, Peters TJ, et al. Cohort study in South and West England of the influence of specialization on the management and outcome of patients with oesophageal and gastric cancers. Br J Surg. 2002;89:914–22. doi: 10.1046/j.1365-2168.2002.02135.x. [DOI] [PubMed] [Google Scholar]
5.Zaninotto P, Parenti AR, Ruol A, Costantini M, Merigliano S, Ancona E. Oesophageal resection for high-grade dysplasia in Barrett's oesophagus. Br J Surg. 2000;97:1102–5. doi: 10.1046/j.1365-2168.2000.01470.x. [DOI] [PubMed] [Google Scholar]
6.Montgomery E, Bronner MP, Goldblum JR, Greenson JK, Haber MM, Hart J, et al. Reproducibility of the diagnosis of dysplasia in Barrett's oesophagus: a reaffirmation. Hum Pathol. 2001;32:368–78. doi: 10.1053/hupa.2001.23510. [DOI] [PubMed] [Google Scholar]
7.Schnell TG, Sontag SJ, Chejfec G, Aranha G, Metz AD, Connell S, et al. Long term non-surgical management of Barrett's esophagus with high-grade dysplasia. Gastroenterology. 2001;120:1607–19. doi: 10.1053/gast.2001.25065. [DOI] [PubMed] [Google Scholar]
8.Ormsby AH, Petras RE, Henricks WH, Rice TW, Rybicki LA, Richter JE, et al. Observer variation in the diagnosis of superficial oesophageal adenocarcinoma. Gut. 2002;51:671–6. doi: 10.1136/gut.51.5.671. [DOI] [PMC free article] [PubMed] [Google Scholar]
9.Overholt BF, Lightdale CJ, Wang KK, Canto MI, Burdick S, Haggitt RC, et al. on behalf of the International Photodynamic group for High-grade dysplasia in Barrett's esophagus Gastrointest Endosc. 2005;62:488–98. doi: 10.1016/j.gie.2005.06.047. [DOI] [PubMed] [Google Scholar]
10.Vij R, Triadafilopoulos G, Owens DK, Kunz P, Sanders GD. Cost-effectiveness of photodynamic therapy for high-grade dysplasia in Barrett's esophagus. Gastrointest Endosc. 2004;60:739–56. doi: 10.1016/s0016-5107(04)02167-4. [DOI] [PubMed] [Google Scholar]
11.Kelty CJ, Ackroyd R, Brown NJ, Stephenson TJ, Stoddard CJ, Reed MWR. Endoscopic ablation of Barrett's oesophagus: a randomised controlled trial of photodynamic therapy vs argon plasma coagulation. Br J Surg. 2004;91:142. doi: 10.1111/j.1365-2036.2004.02277.x. [DOI] [PubMed] [Google Scholar]
12.Pech O, May A, Gossner L, Ell C. Barrett's esophagus: endoscopic resection. Gastrointest Endosc Clin North Am. 2003;13:505–12. doi: 10.1016/s1052-5157(03)00047-3. [DOI] [PubMed] [Google Scholar]
High-grade dysplasia is a histological diagnosis of neoplasia confined to the epithelium. It is the last step in the neoplastic sequence before invasion and rarely, if ever, regresses. One can only determine the optimum treatment of high-grade dysplasia arising in Barrett's oesophagus with accurate data about the risks and benefits of all management options. That this controversy exists reflects significant difficulties in the diagnosis of high-grade dysplasia, a poor understanding of its natural history, and a lack of definitive data regarding such risks and benefits. Nevertheless, it is indisputable that Barrett's oesophagus is a major risk factor for adenocarcinoma of the oesophagus, the incidence of which has increased dramatically over the past 30 years. The chance of cure following oesophagectomy for invasive carcinoma remains low, and it remains likely that the best chance of improving outcome will depend on intervening at a much earlier, pre-invasive stage. The progression from intestinal metaplasia to low-grade dysplasia to high-grade dysplasia and, finally, to invasive carcinoma has been well described.1 Indeed, it forms the basis for the wide-spread use of routine surveillance of patients with Barrett's oesophagus in an attempt to identify those who might benefit from treatment at a pre-invasive stage of the disease.
The rationale for proceeding to oesophagectomy when high-grade dysplasia is diagnosed is predicated by the knowledge that many patients with high-grade dysplasia picked up on surveillance endoscopy will either already have a focus of carcinoma or will shortly develop invasive disease.2–4 There are, however, wide variations both in the reported incidence of carcinoma in oesophagectomy specimens from patients undergoing surgery for high-grade dysplasia (0–73%),2–4 and in the rate of progression of high-grade dysplasia to invasive cancer in patients who are intensively surveyed (16–60%).2,4–7
Diagnosis of high-grade dysplasia
The subjectivity of histopathological interpretation of biopsy specimens from Barrett's oesophagus cannot be underestimated.2,3,7 Agreement between non-specialist pathologists and pathologists who specialise in oesophageal pathology as to what constitutes high-grade dysplasia is only about 50%,7 the diagnoses of high-grade dysplasia by non-specialist pathologists being frequently downgraded to low-grade dysplasia, indefinite for dysplasia or no dysplasia, and even occasionally to normal squamous epithelium! Amongst specialist pathologists, intra-observer and inter-observer agreements for the diagnosis of high-grade dysplasia are 94% and 88%, respectively. When it comes to distinguishing between high-grade dysplasia and intramucosal carcinoma, the agreements are significantly poorer. It is now widely accepted (at least in the UK) that, before any treatment decisions are made based on a diagnosis of high-grade dysplasia, diagnosis is confirmed by two expert independent pathologists on two occasions. Indeed, this is a core requirement in the British Society of Gastroenterology Guidelines for the diagnosis and management of Barrett's oesophagus.8
Natural history of high-grade dysplasia
The wide variation in reported natural history of Barrett's dysplasia can largely be explained by variations in histological interpretation of what constitutes low-grade dysplasia, high-grade dysplasia and indeed intramucosal carcinoma, as well as the intensity of the search for foci of invasive tumour in oesophagectomy specimens.3 In many of the papers reporting a low risk of incidental carcinomas or low rate of progression to carcinoma in patients with high-grade dysplasia, the diagnosis of high-grade dysplasia was made by one pathologist only, thus introducing the risk of overdiagnosis of high-grade dysplasia. In centres using a more rigorous definition of high-grade dysplasia, with independent confirmation by two specialist pathologists together with detailed and aggressive analysis of the surgical specimen, the incidence of invasive carcinoma in oesophagectomy specimens is much higher.4 That microscopic foci of invasive carcinoma are missed on endoscopic biopsy in such patients is hardly surprising. Cameron et al.3 histologically mapped oesophagectomy specimens from patients undergoing oesophagectomy for either high-grade dysplasia or early adenocarcinoma. They demonstrated that areas of microscopic carcinoma are often extremely small and can easily be missed – the median surface area of adenocarcinoma was only 3% of the total Barrett's oesophagus surface area. Furthermore, with standard protocols for the taking and microsectioning of biopsies, only 1–2.5% of the biopsied area and 0.03% of the surveillance area are actually examined under the microscope.7
Oesophagectomy for high-grade dysplasia
It is clear, therefore, that when diagnosed appropriately, high-grade dysplasia is both a precursor of and a marker for invasive cancer. Such patients should be considered for oesophagectomy, a procedure which offers a high chance of long-term cure. The increasing risk of nodal metastases with increasing depth of tumour invasion, and the low chance of cure with N1 disease, provide strong support for the radical treatment of such pre-invasive disease. Oesophagectomy has been traditionally considered to be a procedure associated with high morbidity and significant mortality. Those who argue that oesophagectomy should be reserved only for patients with invasive carcinoma quote high mortality rates for oesophagectomy which are largely historical and not only cover a heterogeneous group of cases including patients with advanced locoregional disease undergoing radical surgery, but also are often from ‘low-volume’ units. With microscopic mucosal disease, neither thoracotomy nor nodal dissection is required, and a ‘non-radical’ transhiatal oesophagectomy can be carried out with minimal morbidity and mortality. The volume–outcome relationship for oesophagectomy is well established, and in-hospital mortality rates of less than 5% can easily be achieved in high-volume centres.9 In the Oxford Oesophago-Gastric Centre, the in-hospital mortality rate for all transhiatal oesophagectomies (including radical transhiatal resections for invasive malignancy) is 1.5%, and the in-hospital mortality rate for transhiatal oesophagectomies for high-grade dysplasia is zero.4Figure 2 shows the Kaplan-Meier survival graph for 17 patients with a pre-operative diagnosis of high-grade dysplasia who underwent oesophagectomy. In six of the surgical specimens there was high-grade dysplasia alone, whereas in eleven (65%) surgical specimens there were foci of invasive malignancy – all patients with high-grade dysplasia alone remain alive and well. Furthermore, although quality of life is undoubtedly impaired in the early postoperative period following oesophagectomy, studies suggest that it returns to pre-operative levels after about 9 months.10 Vagal-sparing oesophagectomy11 and more limited resections12 may reduce morbidity and improve quality of life yet further.
Continued surveillance might be suitable for patients who do not actually have high-grade dysplasia. However, if high-grade dysplasia has been clearly diagnosed according to the stringent criteria outlined above and elsewhere, the risk of missing invasive malignancy is unacceptably high. Furthermore, such a policy runs the risk of patients being ‘lost to follow-up’ and returning some time later with inoperable disease. Endoscopic ablative techniques, particularly photodynamic therapy (PDT), are increasingly popular,2 but clearly do not provide any specimen for histology. Together with short follow-up times, it is difficult, therefore, to verify claims that dysplasia and cancer are eliminated by PDT. Furthermore, residual foci of dysplastic cells may persist deep to the regenerated squamous epithelium. Endoscopic mucosal resection (EMR) does, of course, provide a histological specimen, and may have a role in the treatment of visible lesions or short-segment high-grade dysplasia. High-grade dysplasia is often multifocal, however, and early reports with EMR suggest an unacceptably high rate of positive margins. Most studies on endoscopic therapy for high-grade dysplasia are not randomised or controlled, involve relatively few patients, and have short durations of follow-up – the conclusions that can be drawn from such reports are, as yet, limited.
Conclusions
High-grade dysplasia is the last step in the neoplastic sequence before invasive carcinoma. Its natural history remains unclear, but its strong association with invasive carcinoma requires that it be treated aggressively. Oesophagectomy is the only treatment that reliably removes all the neoplastic epithelium. In healthy patients with reasonable life expectancy, transhiatal oesophagectomy should be the treatment of choice for high-grade dysplasia arising in Barrett's oesophagus. Such surgery should be carried out in high-volume specialist centres with in-hospital mortality rates of well under 5%.
References
1.O'Connor JB, Falk GW, Richter JE. The incidence of adenocarcinoma and dysplasia in Barrett's esophagus. Am J Gastroenterol. 1999;94:2037–42. doi: 10.1111/j.1572-0241.1999.01275.x. [DOI] [PubMed] [Google Scholar]
2.Spechler SJ. Dysplasia in Barrett's oesophagus: limitations of current management strategies. Am J Gastroenterol. 2005;100:927–35. doi: 10.1111/j.1572-0241.2005.41201.x. [DOI] [PubMed] [Google Scholar]
3.Cameron AJ, Carpenter HA. Barrett's esophagus, high-grade dysplasia, and early adenocarcinoma: a pathological study. Am J Gastroenterol. 1997;92:586–91. [PubMed] [Google Scholar]
4.Sujendran V, Sica G, Warren B, Maynard N. Oesophagectomy remains the gold standard for treatment of high-grade dysplasia in Barrett's oesophagus. Eur J Cardiothorac Surg. 2005;28:763–6. doi: 10.1016/j.ejcts.2005.08.018. [DOI] [PubMed] [Google Scholar]
5.Reid BJ, Blount PL, Feng Z, Levine DS. Optimizing endoscopic biopsy detection of early cancers in Barrett's high-grade dysplasia. Am J Gastroenterol. 2000;95:3089–96. doi: 10.1111/j.1572-0241.2000.03182.x. [DOI] [PubMed] [Google Scholar]
6.Schnell TG, Sontag SJ, Chejfec G, Aranha G, Metz AD, Connell S, et al. Long term non-surgical management of Barrett's esophagus with high-grade dysplasia. Gastroenterology. 2001;120:1607–19. doi: 10.1053/gast.2001.25065. [DOI] [PubMed] [Google Scholar]
7.Rice TW. PRO: oesophagectomy is indicated for high grade dysplasia in Barrett's oesophagus. Am J Gastroenterol. 2006;101:2177–9. doi: 10.1111/j.1572-0241.2006.00864_1.x. [DOI] [PubMed] [Google Scholar]
8.British Society of Gastroenterology. Guidelines for the diagnosis management of Barrett's columnar-lined oesophagus. A report of the Working Party of the British Society of Gastroenterology < http://www.bsg.org.uk>.
9.Metzger R, Bollschweiler E, Vallböhmer D, Maish M, DeMeester TR, Hölscher AH. High volume centers for esophagectomy: what is the number needed to achieve low postoperative mortality? Dis Oesoph. 2004;17:310–4. doi: 10.1111/j.1442-2050.2004.00431.x. [DOI] [PubMed] [Google Scholar]
10.Blazeby JM, Farndon JR, Donovan J, Alderson D. A prospective longitudinal study examining the quality of life of patients with oesophageal carcinoma. Cancer. 2000;88:1781–7. [PubMed] [Google Scholar]
11.DeMeester SR. Endoscopic mucosal resection and vagal-sparing oesophagectomy for high-grade dysplasia and adenocarcinoma of the oesophagus. Semin Thorac Cardiovasc Surg. 2005;17:320–5. doi: 10.1053/j.semtcvs.2005.09.001. [DOI] [PubMed] [Google Scholar]
12.Stein HJ, Feith M, Mueller J, Werner M, Siewert JR. Limited resection for early adenocarcinoma in Barrett's oesophagus. Ann Surg. 2000;12:733–42. doi: 10.1097/00000658-200012000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]