

A 49-year-old man with a medical history of hypertension was admitted within one hour after the onset of an acute anterior myocardial infarction with ST elevation for primary coronary intervention (PCI).
He was pretreated with a bolus of aspirin (325 mg) and clopidogrel (600 mg). Before angioplasty, technetium-99m sestamibi was injected to assess the size of the myocardial area at risk (AAR),1 expressed as percentage of the total myocardium with singlephoton emission computed tomography (SPECT) (figure 1). Immediately after injection of technetium, catheterisation was performed demonstrating an occluded left anterior descending coronary artery (LAD). The circumflex artery and right coronary artery showed no lesions of haemodynamic significance. Subsequently, a balloon angioplasty was performed in the LAD with implantation of a bare metal stent (Driver 4.0x12 mm) resulting in TIMI flow 3 without rest stenosis. Two hours later myocardial SPECT was performed using an ambulant gamma camera system (Cardio MD, Philips Medical Systems), which is situated on the coronary care unit. The heart enzymes became maximally elevated six hours after admission (CK 3421 U/l, CK-MB 283 U/l, troponin T 9.0 μg/l). Five days after PCI, a control SPECT was performed using technetium-99m sestamibi and the same camera system to assess the final infarction size (FIS), expressed as percentage of the total myocardium. Myocardial salvage index (MSI) was calculated as AAR minus FIS, divided by the AAR.1 In this patient the calculated salvage index was 0.96 (AAR 48%; FIS 2%) (figure 2). Gated SPECT five days after PCI demonstrated a decrease in left ventricular dimensions compared with gated SPECT early after PCI (end-diastolic volume from 133 to 121 ml and end-systolic volume from 84 to 48 ml, respectively). Before angioplasty, the gated SPECT showed anteroseptal and apical dyskinesia with severely abnormal anterior wall thickening resulting in a left ventricular ejection fraction (LVEF) of 37%. After angioplasty, the wall motion abnormalities had almost normalised (LVEF 60%). Myocardial SPECT is able to demonstrate the extent of irreversible myocardial tissue injury, which is a strong predictor of functional recovery and prognosis in the post-myocardial infarction period.2,3 Moreover, myocardial SPECT is able to calculate the myocardial salvage index, demonstrating the efficacy of any possible intervention, whether it is drug-related or percutaneous.
Figure 1.
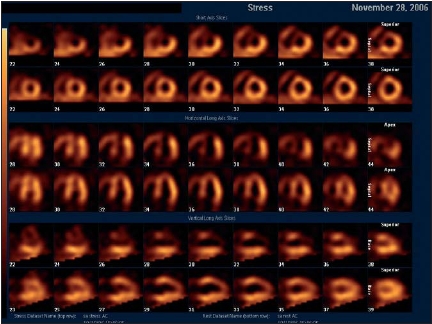
Myocardial SPECT with short axis slices (rows 1 and 2), horizontal axis slices (rows 3 and 4) and vertical axis slices (rows 5 and 6). Before primary coronary intervention (PCI) (rows 1, 3 and 5), severe lack of myocardial count distribution is shown in anteroseptal, anterior and apical walls. After PCI, only a small distal anteroseptal and apical defect can be demonstrated suggesting a small and subendocardial infarction.
Figure 2.
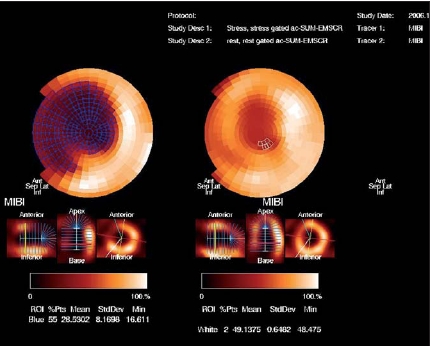
Myocardial SPECT bull’s-eye images summarise three-dimensional data in two dimensions. The blue hatched area in the left plot represents the area at risk before primary coronary intervention (PCI) (48% of the total myocardium). The white hatched area in the right plot demonstrates the final infarction size as percentage of the total myocardium (2%) five days after PCI. Thus, myocardial salvage index can be calculated as area at risk minus final infarction size, divided by the area at risk.
In this section a remarkable ‘image’ is presented and a short comment is given.
We invite you to send in images (in triplicate) with a short comment (one page at the most) to Bohn Stafleu van Loghum, PO Box 246, 3990 GA Houten, E-mail: l.jagers@bsl.nl.
‘Moving images’ are also welcomed and (after acceptance) will be published as aWeb Site Feature and shown on our website: www.cardiologie.nl
This section is edited by M.J.M. Cramer and J.J. Bax.
References
- 1.Ndrepepa G, Mehilli J, Schwaiger M, et al. Prognostic value of myocardial salvage achieved by reperfusion therapy in patients with acute myocardial infarction. J Nucl Med 2004;45:725-9. [PubMed] [Google Scholar]
- 2.Miller T, Christian T, Hopfenspirger M, Hodge D, Gersh B, Gibbons R. Infarct size after acute myocardial infarction measured by quantitative tomographic 99mTc sestamibi imaging predicts subsequent mortality. Circulation 1995;92:334-41. [DOI] [PubMed] [Google Scholar]
- 3.Ibrahim T, Bulow H, Hackl T, Hornke M, Nekolla S, Breuer M, et al. Diagnostic value of contrast-enhanced magnetic resonance imaging and single-photon emission computed tomography for detection of myocardial necrosis early after acute myocardial infarction. J Am Coll Card;2007;49:208-16. [DOI] [PubMed] [Google Scholar]