

Abstract
OBJECTIVE
To describe the American Academy on Communication in Healthcare’s (AACH) Faculty Development Course on Teaching the Medical Interview and report a single year’s outcomes.
DESIGN
We delivered a Faculty Development course on Teaching the Medical Interview whose theme was relationship-centered care to a national and international audience in 1999. Participants completed a retrospective pre-post assessment of their perceived confidence in performing interview, clinical, teaching, and self-awareness skills.
PARTICIPANTS AND SETTING
A total of 79 participants in the 17th annual AACH national faculty development course at the University of Massachusetts Medical School in June 1999.
INTERVENTION
A 5-day course utilized the principles of learner-centered learning to teach a national and international cohort of medical school faculty about teaching the medical interview.
MEASUREMENTS AND MAIN RESULTS
The course fostered individualized, self-directed learning for participants, under the guidance of AACH faculty. Teaching methods included a plenary session, small groups, workshops, and project groups all designed to aid in the achievement of individual learning goals. Course outcomes of retrospective self-assessed confidence in interview, clinical, teaching, self-awareness, and control variables were measured using a 7-point Likert scale. Participants reported improved confidence in interview, clinical, teaching, and self-awareness variables. After controlling for desirability bias as measured by control variables, only teaching and self-awareness mean change scores were statistically significant (p < .001).
CONCLUSIONS
The AACH Faculty Development course on Teaching the Medical Interview utilized learner-centered teaching methods important to insure learning with experienced course participants. Perceived teaching and self-awareness skills changed the most when compared to other skills.
KEY WORDS: medical interview, physician–patient relations, faculty development, educational methods
Research has indicated patient-centered practices improve patient health outcomes,1 satisfaction,2–4 adherence to therapy,5,6 and decrease malpractice claims.7 Whereas these studies did not directly evaluate interviewing practices, many agree that patient-centered interviewing will produce these outcomes. Recent data demonstrate that systematic patient-centered methods are effectively learned8 and that integrating this learning into patient care practices is associated with improved outcomes.9
Although the medical interview is commonly taught in most US and Canadian medical schools,10,11 and communication skills and provider–patient relationships are receiving increased attention from certifying bodies,12,13 the need for faculty development for teachers of these skills is critical.12,14–17 In this era when patients’ experiences of care are used as a marker of individual and organizational performance, it is likely that the need for skills in teaching the medical interview to a broad range of learners will increase.18–20 A recent Cochrane Review underscored the need for clear descriptions of teaching methods for those developing communication skills programs.21
To date, much of the published literature has focused on the teaching of skills pertaining to a single task of the interview, such as screening for domestic violence,22 and delivering bad news.23 One recent study implementing a broad curriculum in the third year at three US medical schools showed encouraging changes in medical students’ communication skills as a result of the implemented curriculum.24 Methods used to achieve these skills included lectures, workshops, demonstrations, role-play involving student–student, student-standardized patient, and student–patient interactions, as well as ward teaching rounds.25
The American Academy on Communication in Healthcare (AACH, formerly the American Academy on Physician and Patient or AAPP) is focused on teaching the medical interview. Whereas its courses have had great success as measured by participant satisfaction and personal testimony, there are no peer-reviewed publications focused on teaching methods. Outcomes of the courses have been published only in the early years of the AACH experience before communication skills were widely taught.26,27
Our aim is to provide a clear, practical, and systematic description of the AACH’s 17th annual Faculty Development course on Teaching the Medical Interview. We will describe in detail the novel methods used so that educators can use these principles in designing curricular interventions and faculty development activities for experienced participants. We also report this course’s learning outcomes.
METHODS
The Faculty Development Intervention
The course, titled Expanding the Center: Moving From Patient-Centered to Relationship-Centered Care, sought to describe the concepts of relationship-centered care (a concept that suggests the centrality of physician–patient, physician–physician, and physician–community relationships to health care)28 and explored its implications for how the medical interview is taught and practiced. We advertised to specialty societies involved in Primary Care education, through educational list serves, and to past course participants both nationally and internationally.
The course focused on development of discrete interviewing, clinical, teaching, and self-awareness skills. We developed this course based on principles of learner-centered learning, which suggests that learning is most effective when learners are able to formulate learning goals, describe clear, measurable, behavioral objectives, choose learning methods to achieve these objectives, and evaluate whether objectives have been met through formative (feedback) and summative evaluation measures.29 We contacted course participants before the course, and asked them to formulate learning goals for the course in writing. These were submitted to the course director, and distributed to participants’ small group faculty who worked with learners most closely during the 5-day experience.
A course schedule is seen in Table 1.
Table 1.
Course Schedule
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | |
|---|---|---|---|---|---|
| 8:00 | Announcements | ||||
| 8:30 | Workshops | Plenary | Workshops | Workshops | Learning Groups |
| 9:00 | |||||
| 9:30 | Learning Groups | ||||
| 10:00 | Project Group Presentations | ||||
| 10:30 | Learning Groups | Learning Groups | |||
| 11:00 | Learning Groups | ||||
| 11:30 | |||||
| 12:00 | |||||
| 12:30 | |||||
| 1:00 | Course Reflection/Evaluation | ||||
| 1:30 | |||||
| 2:00 | |||||
| 2:30 | |||||
| 2:45 | Break | ||||
| 3:00 | Break | Break | |||
| 3:15 | Project Brainstorming | ||||
| 3:30 | Project Group | Project Group | |||
| 4:00 | Project Group | ||||
| 4:30 | |||||
Course time over 5 days was 35.5 hours, with slightly more than 60% in small groups (22 hours) divided between skills work and personal awareness work (in proportions negotiated with groups but approximately a 50–50 split). The remaining hours were devoted to lecture (1.5 hours), workshops (4.5 hours), project groups (6 hours), and course logistics/announcements (1.5 hours).
We utilized multiple teaching methods to achieve learning objectives. A Plenary lecture by a national figure to highlight the relationship-centered care course theme (Jon Kabat Zin, PhD, lectured on Embodying the Hippocratic Calling: The Healing Power of Remembering to be Present).
Workshops were offered and participants attended up to 3 workshops selecting from a menu of workshops including several on: 1) teaching methods, techniques, and models, 2) challenging interactions, and 3) theme-related workshops. Table 2 has a full list of workshops.
Table 2.
Workshop Selections
| Day 1 Workshops | Day 3 Workshops | Day 4 Workshops |
|---|---|---|
| Teaching Methods | Teaching Methods | Teaching Methods |
| Learner-centered Learning | Learner-centered Learning | Learner-centered Learning |
| Feedback | Feedback | Feedback |
| Patient-centered Interviewing | Patient-centered Interviewing | Patient-centered Interviewing |
| Competency-based Interview Curriculum | Three-function Model of Interviewing | Three-function Model of Interviewing |
| Standardizing Standardized Patients | ||
| Challenging Interactions | Challenging Interactions | Challenging Interactions |
| Motivational interviewing | Somatization | Working with the Addicted Patient |
| Breaking Bad News | Alliance and Adherence in Health Behavior counseling | Working with Members of the Addicted Family |
| Family Interviewing | Somatization | |
| Theme-Related | Theme-Related | Theme-Related |
| Clinician–Clinician Communication | Building Relationship-centered Departments | Mutual learning between Doctor and Patient |
| Curricular Approaches to Personal Awareness | Medical Marriages | Meditation/Mindfulness in the Interview |
| Meditation/Mindfulness in the Interview | Narratives of Relationship | |
| Mutual learning between Doctor and Patient | ||
| Meditation/Mindfulness in the Interview |
Workshops had an introduction of concepts, experiential skill-building activities, and reflection to reinforce learning, allowing participants to work on a focused skill over a short period of time. Although not all workshops dealt directly with patient communication skills, they did address applying the principles and skills of relationship-centered care to work (Building a Relationship-Centered Academic Department, Clinician to Clinician communication) and home (Medical Marriages).
Small group sessions focused on interview, clinical, teaching, and self-awareness skills. In these small groups, participants engaged in skills practice and reflected on their skills through self-assessment, peer and faculty assessment, and feedback. Reflection on skills was broadened to include discussing personal responses to patients, patient care, and teaching, and the possible effects these reactions have on encounters. The faculty-to-participant ratio of 1:4 for these small groups allowed for knowledge and skills acquisition tailored to established needs of small-group members. Small group sessions are described in greater detail below.
Project groups took place in which the entire cohort of course participants brainstormed ideas for projects, then formed 13 project groups utilizing a modified Delphi technique, a common technique used to build consensus and prioritize group interests.30 Project group criteria included that more than 1 individual was interested in the topic, individuals committed to working on the project during the course, and each group committed to a presentation of their work at the end of the course. Three meetings of project groups took place. Project groups embody the concepts of learner-centered learning in action: learners organized according to their own interests, and by the end of the week produced an outcome in the form of a presentation to all course participants that met agreed-upon learning goals articulated by group members during their meetings.
Small Group Sessions
In the first small group session, learners articulated and refined their learning goals and objectives, facilitated by course faculty. Throughout the course, faculty worked closely with their small groups to ensure that focused learning objectives were met. For example, 1 small group session consisted of having a participant work on the interviewing skill of talking with patients at the end-of-life in a role play with 1 of the other group members taking on the patient role. Another course participant worked on delivering feedback, whereas the final member also worked on end-of-life skills through focused observation of the role play. Once the interaction took place, the interviewer provided a self-assessment of his interview followed by feedback from the “patient”-participant, other group members (with special attention to the group member who was working on end-of-life skills in the observer role), and faculty. The post-interview feedback facilitated by the group member focused on improving her feedback skills. Faculty then facilitated a portion of the session to ensure that the group member working on delivering feedback received input on her skills of facilitating a feedback session. These activities underscored the importance of experience and reflection to reinforce learning.31
Whereas a typical session described above took approximately 2 hours (20 minutes set up of task and group participant roles, 30 minutes interview with self-assessment from interviewer, 20 minutes of other group feedback and reactions from interviewer with lessons learned, 20 minutes of feedback to the participant facilitating the feedback session, followed by 15 minutes of final lessons, and 15 minutes of planning for the next session), the course schedule allowed for large portions of the day to be designated as learning groups so that if tasks took shorter or longer times, there was flexibility built into the schedule. In subsequent sessions, faculty worked with other group members on their learning needs, thus ensuring that all individuals had an opportunity to work on their own learning needs during the week.
In some small group sessions, termed Personal Awareness groups, participants discussed challenges they faced in teaching and patient care encounters (and sometimes their personal life) to examine how these issues affected their communication with patients, colleagues, or teaching performance. For example, 1 course participant reflected on his challenges with a dying patient, and through gentle probing, came to realize that his own discomfort with death was a contributor to this difficulty. Methods utilized to facilitate personal awareness groups included challenging case discussions, based on methods or Balint groups,32 discussing family of origin33 and its effect on communication, as well as more open-ended discussion based on methods advocated by Carl Rogers.34
Program Evaluation and Analysis
We used a retrospective pre-post design for course evaluation. Participants completed a 29-item evaluation immediately after the course that assessed their skill level at two points: before (retrospective pretest) and after (posttest) the course.35–37 The questionnaire assessed participant confidence in using interview (10 items), clinical (3 items), teaching (7 items), and self-awareness skills (3 items). Six items, designated control variables, were not formally or systematically taught during the course and were included to provide a measure of desirability bias.35,38 Questionnaire responses were on a Likert scale of 1 to 7, with anchors of 1 = not at all confident and 7 = completely confident. The evaluation instrument outlining all four subscales and the control variables is included as Appendix.
Demographic variables were gathered including gender, age, years teaching in a medical school, years teaching the medical interview, and the number of prior AACH courses attended. Descriptive statistics were computed for demographic variables. Paired-samples t tests were used to assess if mean change scores were different across skill category. Additional t tests were performed to assess pre/post mean differences in confidence in utilizing skills before and after adjusting for desirability bias as measured by the control variables. The adjustment was calculated by subtracting the average of the pre/post mean difference of the control variables from each skill category post measure. Reliability analysis was conducted on all questionnaire items (excluding the control variables) and the four subscales using Cronbach’s alpha as the measure. Linear regression was used to determine whether participant demographic variables predicted post-course skills assessment.
RESULTS
Seventy-nine participants took part in the course. Approximately one-half of the sample (52%) was 45 or younger, 54% were male. Forty-six percent were first-time course participants, 28% attended 1 prior course, and 26% attended 2 or more prior AACH courses (see Table 3).
Table 3.
Descriptive Characteristics of Course Participants
| Demographic Characteristic | N | % |
|---|---|---|
| Gender | ||
| Male | 31 | 54 |
| Female | 26 | 46 |
| Age | ||
| 29–35 | 14 | 23 |
| 36–40 | 8 | 13 |
| 41–45 | 10 | 16 |
| 46–50 | 16 | 26 |
| 51 or greater | 14 | 23 |
| AAPP Experience | ||
| No prior course | 28 | 46 |
| One course | 17 | 28 |
| Two or more courses | 16 | 26 |
Participants had been practicing medicine an average of 14 years, with a mean of 8 years teaching medical school, and 6 years teaching the medical interview (data not shown). Participants were from the United States and 4 additional countries, were predominantly physicians, although 15 (20%) were educators trained in social work, psychology, and education.
Sixty-five participants (82%) completed course evaluations. Initial analysis indicated statistically significant changes in mean scores of participants’ confidence in interview (mean pre = 5.0, Standard deviation or SD 0.8, post = 5.6, SD 0.6; p < .001), clinical (pre = 4.1, SD 0.9 post = 4.8, SD 0.9; p < .001), teaching (pre = 4.1, SD 0.9 post = 5.2, SD 0.8; p < .001), self-awareness (pre = 4.3, SD 1.1 post = 5.5, SD 0.8; p < .001) skills and control variables (mean pre = 4.4, SD 1.1, post = 5.0, SD 0.9; p < .001). Scores in interview skills demonstrated the smallest change, although the participants rated their interview skills highest of all categories before the intervention.
Further analysis using a paired t test after adjusting for the average of the control variables’ pre/post difference demonstrated that only teaching and self-awareness mean change scores were statistically significant (p < .001). Figure 1 reflects the mean change scores with their respective confidence intervals, after accounting for desirability bias.
Figure 1.
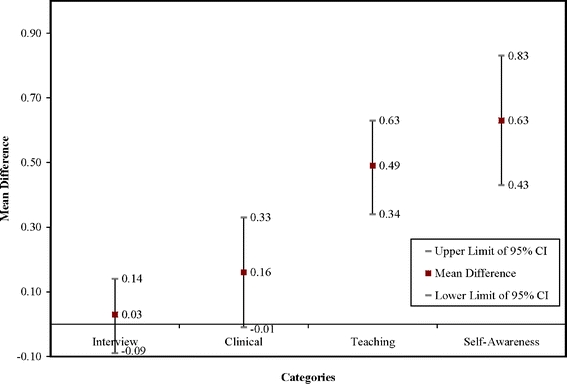
Change in pre/post skill categories after accounting for desirability bias
There was no significant effect of years of practice, gender, or age on the 4 skill variables, except the personal awareness variable where the training increased personal awareness most in older female participants (51 years and older; p < .01).
Results for the reliability analysis showed a high alpha for the overall scale (pre = 0.93, post = 0.93) and 3 of the 4 subscales: interview (pre = 0.88, post = 0.86), teaching (pre = 0.88, post = 0.90), and self-awareness (pre = 0.84, post = 0.82). Clinical skills pre and post were lower (pre = 0.58, post = 0.61). These alpha levels suggest that evaluation responses measured participants’ confidence and changes were not because of different interpretations of the questionnaire content.
One additional outcome is that some project groups continued to work after the course, and this led to the publication of scholarly work.39,40
DISCUSSION
The AACH’s 17th annual Faculty Development course demonstrated that, guided by needs assessment of learners’ goals, a faculty development intervention can be designed to meet diverse needs of a national and international group of participants with a broad range of experience teaching the medical interview. We used teaching methods that allowed participants to form specific goals and objectives and take concrete steps to achieve them during the course. In contrast to a self-study process, our program emphasized the importance of small group learning and the teacher–learner relationship to ensure learning. The importance of goal-setting, observation, guided reflection, and feedback based on participant goals in the learning process has been described as critical in teaching communication skills41 and in developing expertise with complex learning tasks.42 More than half of the participants in this faculty development program had previously attended a similar AACH course. The extent to which these experienced learners influenced the learning of others is unknown, but may have been significant given our emphasis on small-group learning and shared experiences.
There are other medical interview teaching interventions that have demonstrated success, but these are typically with a single skill set22,23 with undergraduate medical students25,43 or at single institutions.8,9 Our teaching that utilizes learner-centered teaching methods requires a faculty well versed in teaching communication skills, but also adept at modifying his or her teaching to specific participant learning needs. This results in a course that ultimately has no “standard” curriculum, but whose process embodies the learner-centered principles it seeks to teach.29
Our teaching intervention produced clear outcomes in perceived skills for a faculty development program, while overcoming common sources of bias. We observed improvement in two broad skill areas: teaching skills and self-awareness skills, consistent with our focus on teaching and skills unique to the AACH model, self-awareness. Smaller changes in interviewing and clinical skills were not statistically significant.
The presence of feelings related to encounters have been demonstrated to potentially affect performance in the medical interview,44,45 providing a rationale for including content related to self-awareness in this faculty development intervention. In addition, reflection promoting self-assessment, self-awareness, and learning is felt by many to be integral to professional training,46 teacher development,46–49 and for learners to effectively learn patient-centered interviewing skills.45,50 A recent article stems from AACH work and describes how personal awareness can be taught by teachers without specific psychological training.51
Whereas a recent review points out the limited correlation of physician self-assessment compared to observed measures of competence,52 three studies directly related to our subject matter and evaluation methods show a positive correlation. Smith8 demonstrated that improvement in resident attitudes of self-efficacy in interviewing skills was accompanied by improved skills performance with both real and simulated patients. Williams and Deci53 demonstrated that the use of learner-centered teaching methods for interviewing skills led to increased self-assessed perception of learner competence and improvement in interview skills at 6 months as assessed by standardized patient interviews. Hewson’s faculty development interventions demonstrated positive correlations between participant’s self-assessed retrospective pre-post teaching skills evaluations, and improved teaching evaluations by learners.54,55 This suggests that the improved self-efficacy we observed could be similarly paralleled by improved skills.
Several faculty development programs have used experiential teaching methods like our course and demonstrated that faculty development in teaching skills related to the medical interview were improved as assessed by videotape analysis of teaching,56 and that interview skills of students improved after being instructed by teachers trained to teach the medical interview.57
This paper has broader implications for educational programs with experienced national and international audiences. Whereas prior curricular interventions have stressed the importance of insuring buy-in and fitting curricular interventions into an already existing context,25,26 our intervention assessed and met learners’ needs over a relatively short period of time. The process by which faculty rapidly and repeatedly assessed learning needs and took steps to meet them is important in allowing learners to meet their learning goals and objectives.29 This approach requires significant investment in small group sessions and skilled faculty who can teach the material pertinent to the medical interview, while being flexible enough to meet individual learner’s needs. This framework parallels the one derived empirically by Fryer-Edwards who broke down this teaching process into the following steps: 1) identifying a learning edge (setting goals), 2) proposing and testing hypotheses (trying new skills), and 3) calibrating learner’s self-assessments (feedback and evaluation).41 Educators running faculty development programs should consider adapting their methodology to allow individual learners to establish their own learning goals and objectives and choose methods that allow for their achievement during their programs.
This course, with its emphasis on and commitment to learner-centered learning, skills practice, and reflection for skills improvement provides a unique approach to faculty development and could serve as a model for other faculty development efforts, especially those with the goal of disseminating the practice of health care relationships and communication that integrates best medical practices with patients’ and clinicians’ values, needs, and choices, the mission of the AACH.
Acknowledgments
Conflict of Interest None disclosed.
Appendix
Table 4.
Items from Assessment Instrument
| Interview | 1. Can make patients comfortable and set stage for medical visit |
| 2. Efficiently negotiate the patient’s agenda for the visit | |
| 3. Elicit patient’s explanatory model for their illness | |
| 4. Can elicit patient’s personal story in an open-ended manner | |
| 5. Elicit the patent’s emotional reactions in an open ended manner | |
| 6. Effectively inform the patient about necessary information | |
| 7. Effectively motivate patient to change unhealthy behaviors | |
| 8. Manage the patient’s expressed emotion | |
| 9. Conduct the open ended, patient centered aspect of the medical interview efficiently | |
| 10. Obtain patient’s description of physical symptoms in open-ended manner | |
| Clinical | 1. Effectively manage patients with substance abuse problems |
| 2. Effectively manage patients with many somatic symptoms without a disease explanation | |
| 3. Effectively manage patients with anger/hostility | |
| Teaching | 1. Provide effective feedback on communication skills |
| 2. Facilitate small groups | |
| 3. Teach in a learner-centered way | |
| 4. Work effectively with a resistant learner | |
| 5. Work effectively with a learner who dominates group | |
| 6. Use role play or simulations to teach medical interviewing | |
| 7. Recognize specific interviewing behaviors that promote or impede effective encounters | |
| Personal Awareness | 1. Promote personal growth in myself and others |
| 2. Recognize personal responses to patients and how they affect the interaction | |
| 3. Recognize personal responses to learners and how they affect the interaction | |
| Control Variables | 1. Effectively manage patients with different socioeconomic needs |
| 2. Effectively manage patients with depression | |
| 3. Effectively manage patients with anxiety | |
| 4. Effectively work with patients from different cultural backgrounds | |
| 5. Develop an interviewing skills curriculum for my institution | |
| 6. Use videotape reviews to teach the medical interview |
Footnotes
This study was presented in part at the 23rd annual meeting of the Society of General Internal Medicine, Boston, MA, May, 2000.
References
- 1.Greenfield S, Kaplan S, Ware JE Jr. Expanding patient involvement in care. Effects on patient outcomes. Ann Int Med. 1985;102:520–8. [DOI] [PubMed]
- 2.O’Keefe M, Sawyer M, Roberton D. Medical student interviewing skills and mother reported satisfaction and recall. Med Educ. 2001;35:637–44. [DOI] [PubMed]
- 3.Mangione-Smith R, McGlynn EA, Elliott MN, McDonald L, Franz CE, Kravitz RL. Parent expectations for antibiotics, physician-parent communication, and satisfaction. Arch Pediatr Adolesc Med. 2001;155:800–6. [DOI] [PubMed]
- 4.Jackson JL, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52:609–20. [DOI] [PubMed]
- 5.Hausman A. Taking your medicine: relational steps to improving patient compliance. Health Market Quart. 2001;19:49–71. [DOI] [PubMed]
- 6.Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. J Clin Pharm Ther. 2001;26:331–42. [DOI] [PubMed]
- 7.Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM. Physician–patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553–9. [DOI] [PubMed]
- 8.Smith RC, Lyles, JS, Mettler MA, Stoffelmayr BE, et al. The effectiveness of intensive training for residents in interviewing: A randomized controlled study. Ann Int Med. 1998;128:118-126. [DOI] [PubMed]
- 9.Smith RC, Lyles JS, Gardiner JC, et al. Primary care clinicians treat patients with medically unexplained symptoms—a randomized controlled trial. J Gen Intern Med. 2006;21:671–7. [DOI] [PMC free article] [PubMed]
- 10.Novack DH, Volk G, Drossman DA, Lipkin M Jr. Medical interviewing and interpersonal skills teaching in US medical schools. Progress, problems, and promise. JAMA. 1993;269:2101–5. [DOI] [PubMed]
- 11.Anonymous. Consensus statement from the workshop on the teaching and assessment of communication skills in Canadian medical schools. Can Med Assoc J. 1992;147:1145–9. [PMC free article] [PubMed]
- 12.ACGME Outcome Project. Faculty Development. Available at: http://www.acgme.org/Outcome. Accessed September 5, 2007.
- 13.American Board of Internal Medicine. Maintenance of Certification. Available at http://www.abim.org/moc/sempbpi.shtm. Accessed September 5, 2007.
- 14.Simpson M, Buckman, Stewart M, et al. Doctor–patient communication: the Toronto consensus statement. BMJ. 1991;303:1385–7. [DOI] [PMC free article] [PubMed]
- 15.Association of American Medical Colleges. Contemporary Issues in Medicine: Communication in Medicine. Washington, DC: Association of American Medical Colleges; 1999.
- 16.Evans CH. Faculty development in a changing academic environment. Acad Med. 1995;70:14–20. [DOI] [PubMed]
- 17.Lang F, Everett K, McGowen R, Bernard B. Faculty development in communication skills instruction: insights from a longitudinal program with “real time feedback.” Acad Med. 2000;75:1222–8. [DOI] [PubMed]
- 18.Bertakis KD. The communication of information from physician to patient: a method of increasing patient retention and satisfaction. J Fam Pract. 1977;5:217–22. [PubMed]
- 19.Safran D, Montgomery J, Chang H, et al. Switching doctors: predictors of voluntary disenrollment from a primary physician’s practice. J Fam Pract. 2001;50:130–6. [PubMed]
- 20.Federman AD, Cook EF, Phillips RS, et al. Intention to discontinue care among primary care patients: influence of physician behavior and process of care. J Gen Intern Med. 2001;16:668–74. [DOI] [PMC free article] [PubMed]
- 21.Fellowes D, Wilkinson S, Moore P. Communication skills training for health care professionals working with cancer patients, their families and/or carers. Cochrane Database of Systematic Reviews 2004, Issue 2. Art. No.: CD03751. DOI 10.1002/14651858.CD002751.pub2. [DOI] [PubMed]
- 22.Jonassen JA, Pugnaire MP, Mazor K, et al. The effect of a domestic violence interclerkship on the knowledge, attitudes, and skills of third-year medical students. Acad Med. 1999;74:821–8. [DOI] [PubMed]
- 23.Rosenbaum ME, Kreiter C. Teaching delivery of bad news using experiential sessions with standardized patients. Teaching and Learning in Medicine. 2002;14:144–9. [DOI] [PubMed]
- 24.Yedidia MJ, Gillepsie CC, Kachur E, et al. Effect of communications training on medical student performance. JAMA. 2003;290:1157–65. [DOI] [PubMed]
- 25.Kalet A, Pugnaire MP, Cole-Kelley K, et al. Teaching communication in clinical clerkships: models from the Macy initiative in health communication. Acad Med. 2004;79:511–20. [DOI] [PubMed]
- 26.Rost K, Gordon GH. The teacher simulation exercise: changes in physician teaching emphasis and strategy. J Gen Intern Med. 1989;4:121–6. [DOI] [PubMed]
- 27.Gordon GH, Levinson W. Attitudes toward learner-centered learning at a faculty development course. Teaching and Learning in Medicine. 1990;2:106–9.
- 28.Tresolini CP, Pew-Fetzer Task Force. Health Professions Education and Relationship-centered Care. San Francisco: Pew Health Professions Commission; 1994.
- 29.Kaplan C. Learner centered learning. Medical Encounter. 1992;8:2–4.
- 30.Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32:1008–15. [DOI] [PubMed]
- 31.Smith CS, Irby DM. The roles of experience and reflection in ambulatory education. Acad Med. 1997;72:32–5. [PubMed]
- 32.Samuel O. How doctors learn in a Balint group. Fam Pract. 1989;6:108–13. [DOI] [PubMed]
- 33.Mengel MB. Physician ineffectiveness due to family-of-origin issues. Fam Syst Med. 1987;5:176–90.
- 34.Rogers C. On Becoming a Person. Boston: Houghton Mifflin Co.; 1961.
- 35.Aiken LS, West SG. Invalidity of true experiments: self-report pretest biases. Eval Rev. 1990;14:374–90. [DOI]
- 36.Howard GS, Dailey PR. Response-shift bias: a source of contamination of self-report measures. J Appl Psychol. 1979;64:144–50. [DOI]
- 37.Sprinagers M, Hoogstraten J. On delay and reassessment of retrospective preratings. J Exp Educ. 1988;56:148–53.
- 38.Hebert J, Clemow L, Pbert L, et al. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int J Epidemiol. 1995;24:389-98. [DOI] [PubMed]
- 39.Branch WT Jr, Kern D, Haidet P, et al. The patient–physician relationship. Teaching the human dimensions of care in clinical settings. JAMA. 2001;286:1067–74. [DOI] [PubMed]
- 40.Gracey CF, Haidet P, Branch WT, et al. Precepting humanism: strategies for fostering the human dimensions of care in ambulatory settings. Acad Med. 2005;80:21–8. [DOI] [PubMed]
- 41.Fryer-Edwards K, Arnold R, Baile W, et al. Reflective teaching practices: an approach to teaching communication skills in a small group setting. Acad Med. 2006;81:638–44. [DOI] [PubMed]
- 42.Quirk ME. Intuition and Metacognition in Medical Education: Keys to Developing Expertise. New York: Springer Publishing; 2006.
- 43.Makoul G. The SEGUE framework for teaching and assessing communication skills. Patient Educ Couns. 2001;45:23–34. [DOI] [PubMed]
- 44.Marshall AA, Smith RC. Physicians’ emotional reactions to patients: recognizing and managing counter transference. Am J Gastroenterol. 1995;90:4–8. [PubMed]
- 45.Novack DH, Suchman AL, Clark W, et al. Calibrating the physician. Personal awareness and effective patient care. JAMA. 1997;278:502–9. [DOI] [PubMed]
- 46.Epstein R. Mindful practice. JAMA. 1999;282:833–8. [DOI] [PubMed]
- 47.Palmer P. The Courage to Teach. San Francisco: Josey-Bass; 1998.
- 48.Brookfield S. Becoming a Critically Reflective Teacher. San Francisco: Josey-Bass; 1995.
- 49.Cole KA, Barker LR, Kolodner K, et al. Faculty development in teaching skills: an intensive longitudinal model. Acad Med. 2004;79:469–80. [DOI] [PubMed]
- 50.Smith RC, Marshall AA, Lyles JS, Frankel RM. Teaching self-awareness enhances learning about interviewing. Acad Med. 1999;74:1242–8. [DOI] [PubMed]
- 51.Smith RC, Dwamena FC, Fortin VI, AF. Teaching personal awareness. JGIM. 2005;20:201–7. [DOI] [PMC free article] [PubMed]
- 52.Davis DA, Mazmanian PE, Fordis M, et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296:1094–102. [DOI] [PubMed]
- 53.Williams GC, Deci EL. Internalization of biopsychosocial values by medical students: a test of self-determination theory. J Pers Soc Psychol. 1996;70:115–26. [DOI] [PubMed]
- 54.Hewson MG, Copeland HL. Outcomes assessment of a faculty development program in medicine and pediatrics. Acad Med. 1999;74:S68–S71. [DOI] [PubMed]
- 55.Hewson MG, Copeland HL, Fishleder AJ. What’s the use of faculty development? Evaluation using retrospective self-assessments and independent performance ratings. Teaching and Learning in Med. 2001;13:153–60. [DOI] [PubMed]
- 56.Naji SA, Maguire GP, Fairbairn SA, Goldberg DP, Faragher EB. Training clinical teachers in psychiatry to teach interviewing skills to medical students. Med Educ. 1986;20:140–7. [DOI] [PubMed]
- 57.Gask L, Goldberg JB, Craig T, et al. Training general practitioners to teach psychiatric interviewing skills: an evaluation of group training. Med Educ. 1991;25:444–51. [DOI] [PubMed]