

Abstract
BACKGROUND
Compared to those with depression alone, depressed patients with posttraumatic stress disorder (PTSD) experience more severe psychiatric symptomatology and factors that complicate treatment.
OBJECTIVE
To estimate PTSD prevalence among depressed military veteran primary care patients and compare demographic/illness characteristics of PTSD screen-positive depressed patients (MDD-PTSD+) to those with depression alone (MDD).
DESIGN
Cross-sectional comparison of MDD patients versus MDD-PTSD+ patients.
PARTICIPANTS
Six hundred seventy-seven randomly sampled depressed patients with at least 1 primary care visit in the previous 12 months. Participants composed the baseline sample of a group randomized trial of collaborative care for depression in 10 VA primary care practices in 5 states.
MEASUREMENTS
The Patient Health Questionnaire-9 assessed MDD. Probable PTSD was defined as a Primary Care PTSD Screen ≥ 3. Regression-based techniques compared MDD and MDD-PTSD+ patients on demographic/illness characteristics.
RESULTS
Thirty-six percent of depressed patients screened positive for PTSD. Adjusting for sociodemographic differences and physical illness comorbidity, MDD-PTSD+ patients reported more severe depression (P < .001), lower social support (P < .001), more frequent outpatient health care visits (P < .001), and were more likely to report suicidal ideation (P < .001) than MDD patients. No differences were observed in alcohol consumption, self-reported general health, and physical illness comorbidity.
CONCLUSIONS
PTSD is more common among depressed primary care patients than previously thought. Comorbid PTSD among depressed patients is associated with increased illness burden, poorer prognosis, and delayed response to depression treatment. Providers should consider recommending psychotherapeutic interventions for depressed patients with PTSD.
Key words: depression, PTSD, primary care, clinical practice guidelines
INTRODUCTION
Depressed patients present in general medical settings more frequently than in specialty mental health settings.1,2 Despite estimates suggesting that nearly 20% of primary care patients experience major depressive disorder (MDD) symptomatology,3,4 depression is detected in only 50% of cases.1,5 Furthermore, primary care–based depression treatment is often inadequate.2 The increasing proportion of patients treated in primary as opposed to specialty mental health care settings6 will increase demand among general medicine providers for interventions that support appropriate depression management.
To improve depression detection and care, multiple health care associations have authored depression clinical practice guidelines.7–9 Guideline-concordant treatment improves MDD detection and leads to improved process and outcomes including increased antidepressant treatment adherence and decreased symptomatology.10–12 Despite documented benefit, full MDD guideline implementation remains the exception to the norm,13 with impediments including health care system inertia and physicians’ depression-relevant attitudes and knowledge.13,14
Like MDD, posttraumatic stress disorder (PTSD) is common. Prevalence estimates among medical patients range from 7% to 36%.15–19 Although PTSD confers significant psychiatric disturbance, functional impairment, and morbidity as a singular diagnosis,18,20,21 depression and PTSD commonly co-occur. Research suggests, for example, that significant depressive symptomatology affects between 30% and 50% of persons diagnosed with PTSD.22–26
The Veterans Health Administration (VA) recently mandated nationwide primary care screening for depression and implemented a performance measure to gauge care quality vis-à-vis depression clinical practice guideline concordance.27 Aside from directing the practitioner to assess for comorbid psychiatric conditions, VA and other depression guidelines approach MDD and PTSD as separate entities with distinct pathogenesis and treatment indications. Given the frequency of MDD-PTSD co-occurrence, however, it is shortsighted to treat MDD without consideration of the possibility that PTSD might also be present. Indeed, the persistent course of PTSD and the fact that some PTSD symptoms appear to be treatment-resistant28 have the potential to increase complexity among depressed patients. At a minimum, it is important for general medicine providers to be aware of depressed primary care patients with PTSD.
We estimated the prevalence of probable PTSD among a sample of depressed VA primary care patients. Additionally, we compared demographic and illness-related characteristics of patients with depression alone (MDD) to those of depressed patients with positive PTSD screens (MDD-PTSD+). To our knowledge, this study is among the first to examine MDD-PTSD+ comorbidity in a sample recruited to resemble those who would be identified in clinical practices that employ routine depression screening. Indeed, to increase our findings’ clinical utility, we identified depressed participants using the Patient Health Questionnaire-9 (PHQ-9: 29), a self-report measure assessing frequency of depressive symptomatology that is recommended as the best available primary care–based depression screening tool.30 Relative to MDD-alone patients, we hypothesized that MDD-PTSD+ patients would evince worse depressive symptomatology, more frequent suicidal ideation, worse physical health, higher alcohol consumption, lower social support, increased mental and physical health care utilization, and lower care satisfaction.
METHODS
We present cross-sectional baseline analyses of participants from a site-randomized evaluation of a quality improvement depression intervention.
Setting
The parent study included participants from 10 VA primary care clinics located in rural/semi-rural settings or small cities in 5 states; 3 clinics were randomized to provide usual depression care, and 7 implemented a collaborative care intervention. Clinics served between 1,512 to and 11,506 patients annually. The present study examined participants from intervention and control clinics collectively.
Participants and Recruitment
A contracted firm conducted computer-assisted telephone interviewing (CATI) to determine eligibility and collect baseline data. Parent study eligibility required participants to have an upcoming appointment and to have attended a study clinic within the previous 12 months. Administrative databases identified potential eligible participants who were sent letters describing the study and providing refusal opportunities. Approximately 2 weeks later, data collection personnel began CATI. New contacts continued until each clinic met parent study enrollment targets, which were determined by power analyses. Study protocols were approved by participating clinics’ Institutional Review Boards (IRBs) and the project’s administrative sites.
Major depressive symptomatology (PHQ-9 ≥ 10)29 was required for enrollment. Exclusion criteria included acute suicidality and problems that precluded CATI participation. Because we were interested in the potential for PTSD to complicate provision of clinical practice guideline treatment for unipolar depression, we also excluded patients with probable bipolar disorder. Results of screening and enrollment are described below.
Measures
The 50-minute baseline interview included the following measures employed in the present analyses:
Demographic characteristics Demographics included participant gender, age, ethnicity (White vs. non-White), relationship status (married/living as married vs. single), education (high school or less vs. some college or more), and current employment (employed full or part-time, unemployed, on disability, retired, or other).
Depressive symptomatology The PHQ-9 assessed depressive symptom severity. Using a 4-point scale (“0 = not at all” to “3 = every day/nearly every day”), participants indicated a 2-week frequency of DSM-IV31 major depressive episode symptoms. Higher scores indicated worse symptomatology.
Suicidal ideation We dichotomized the PHQ-9 suicide/self-harm item to indicate presence/absence of suicidal ideation, with “0 = Not at all” coded as negative suicidal ideation and “1 = Several days” or greater coded as positive.
PTSD The Primary Care PTSD Screen (PC-PTSD)32 assessed presence of probable PTSD. Participants received a single point for the previous month’s presence of each of 4 PTSD symptoms (i.e., reexperiencing, avoidance, hypervigilance, and emotional numbing related to past trauma). Summing the points generated scores ranging from 0 to 4. Previous work32 suggested that scores of 3 and greater identify PTSD with reasonable sensitivity (0.78) and specificity (0.89). Scores of 3 and 4 represented positive PTSD screens.
Anxiety and panic Two questions assessed general anxiety and panic attacks over the past 6 months. Participants indicated whether they had felt “anxious much of the time (yes/no)” and/or experienced “a panic attack when [they] suddenly felt intense fear and discomfort (yes/no).” An additional question assessed whether a panic attack had occurred during the past month.
Probable bipolar disorder Positive responses to both of the following questions identified patients with probable bipolar disorder: “Did a doctor ever say you had a manic-depressive or bipolar illness?” and “Have you ever taken the medications Lithium, Depakote, or Tegretol for a depressive illness?”
Alcohol consumption The Alcohol Use Disorders Identification Test consumption questions (AUDIT-C)33 evaluated alcohol consumption. Participants who denied past-year consumption received a score of “0.” For those with more recent use, summed AUDIT-C responses resulted in an index where higher scores reflected higher consumption. The AUDIT-C predicts poor alcohol-related outcomes; scores greater than 8 demonstrate an association with mortality.34
General health The following Health Status Questionnaire35 item provided an indicator of general health: “In general would you say your health is...” Response options ranged from “1 = excellent” to “5 = poor.”
Medical comorbidity The Seattle Index of Comorbidity (SIC)36 assessed medical comorbidity. The SIC includes presence/absence of 7 chronic illness conditions, cigarette smoking status, and participant age. The SIC summary score predicts hospitalization and mortality.36
Social support Eight items from the Medical Outcomes Study Social Support Scale37 assessed emotional and tangible social support. Higher mean scores reflected higher social support.
Self-reported care utilization Participants reported the frequency of medical care received in the previous 6 months. Frequencies of outpatient, inpatient, and emergency department care were assessed separately. Participants reported frequency of care for physical and emotional problems in each treatment venue separately.
Care satisfaction Two questions adapted from the Partners in Care study38 assessed participants’ satisfaction with available health care services over the previous 6 months. We assessed care satisfaction for physical health and emotional problems separately on a scale ranging from “1 = very satisfied” to “6 = very dissatisfied.”
Analysis
Survey data were adjusted for population weights (age and gender) derived to reflect the sampling frame and probability of participant enrollment (procedures available upon request). Bivariate and multivariate analyses examined differences between MDD and MDD-PTSD+ patients. In bivariate analyses, t tests detected differences between groups on continuous measures, and chi-square statistics tested proportional differences on categorical measures. Multivariate regression analyses tested a priori hypotheses that PTSD would evidence relationships with several clinically relevant variables with potential to complicate primary care–based depression treatment. Separate models were fit for each variable; PC-PTSD screen status (dummy-coded: 0 = negative, 1 = positive) and demographic covariates were entered simultaneously in each model.
RESULTS
Participants
Figure 1 presents our screening and sampling strategy. The entire sampling frame included 28,474 patients. We screened 10,929 patients (38% of total) for depression; 9,615 screened negative or refused the full screen, and 30 were acutely suicidal. Finally, 523 of the 1,313 eligible depressed patients refused enrollment. Eighty-four patients met the present study’s bipolar disorder exclusion criterion. The final sample included 677 depressed patients.
Figure 1.
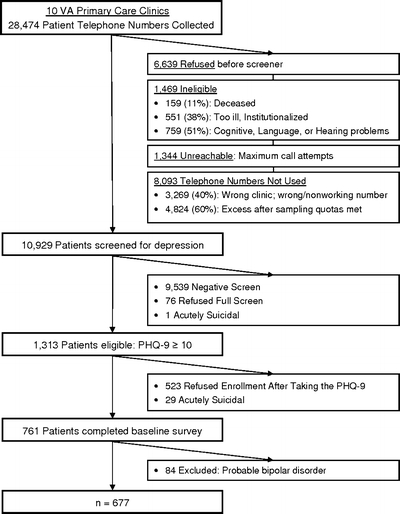
Participant enrollment.
Table 1 presents demographic, psychosocial, and illness-related characteristics for the entire sample and separately for MDD and MDD-PTSD+ patients. Overall PHQ-9 scores indicated moderately severe depression.29
Table 1.
Bivariate Comparisons: Demographic Characteristics, Health Care Satisfaction, and Illness Characteristics for PTSD Screen Negative and Screen Positive Participants*
| Characteristic | Overall (n = 677) | PTSD screen negative (n = 433) | PTSD screen positive (n = 244) | p† |
|---|---|---|---|---|
| Mean Age (SD) | 65 (13) | 68 (15) | 59 (22) | <.001 |
| Gender (% Male) | 96.1 | 96.8 | 94.7 | .14 |
| Ethnicity (% White) | 87.6 | 90.5 | 81.1 | <.001 |
| Education (% < High School) | 53.9 | 58.0 | 44.8 | .002 |
| Relationship status (% Married/living as married) | 63.4 | 65.0 | 59.9 | .21 |
| Employment (%) | <.001 | |||
| Full-time or part-time | 13.8 | 13.0 | 15.8 | |
| Unemployed | 9.4 | 7.9 | 12.8 | |
| On disability | 34.7 | 27.1 | 51.7 | |
| Retired | 42.0 | 52.1 | 19.7 | |
| Satisfied/very satisfied with care (%) | ||||
| Physical | 73.2 | 74.9 | 69.3 | .13 |
| Emotional | 64.8 | 66.7 | 60.7 | .15 |
| Self-reported general health (%) | .90 | |||
| Excellent or very good | 5.0 | 4.9 | 5.3 | |
| Good | 14.4 | 15.1 | 12.8 | |
| Fair | 34.0 | 33.6 | 34.9 | |
| Poor | 46.6 | 46.4 | 47.0 | |
| Mean physical comorbidity: SIC (SD) | 7.9 (3.5) | 8.4 (4.1) | 6.8 (6.4) | <.001 |
| Alcohol use: AUDIT-C (%) | .18 | |||
| 0 | 55.8 | 57.5 | 50.0 | |
| 1–3 | 23.1 | 21.9 | 27.6 | |
| 4–7 | 13.7 | 14.4 | 14.4 | |
| 8–12 | 7.4 | 6.2 | 8.4 | |
| Mean social support‡ (sd) | 3.7 (1.2) | 3.9 (1.1) | 3.5 (1.2) | <.001 |
| General anxiety (% yes) | 59.7 | 49.5 | 82.5 | <.001 |
| Panic attack—1 month (% yes) | 20.6 | 9.7 | 45.1 | <.001 |
| Mean depressive severity: PHQ-9 (SD) | 15.5 (4.4) | 14.7 (7.6) | 17.4 (5.0) | <.001 |
| Suicidal ideation (% yes) | 28.7 | 22.3 | 43.3 | <.001 |
*Data are adjusted for population weights and probability of enrollment.
†Significance tests included X2analyses for categorical data and t tests for continuous data.
‡Higher value indicates more social support.
Bivariate Analyses
As indicated in Table 1, 36% of patients screened positive on the PC-PTSD, suggesting a high likelihood of MDD-PTSD comorbidity. Relative to MDD patients, MDD-PTSD+ patients were younger (P < .001), more likely to be non-White (P < .001), and were better educated (P = .002). In addition, more MDD-PTSD+ patients reported being disabled (52% v. 27%, P < .001).
Whereas self-reported general health did not differ, the SIC indicated more severe physical illness comorbidity among the older, MDD patients (P < .001). Moreover, patient groups reported similar physical and emotional care satisfaction (P = .13 and P = .15, respectively) and alcohol consumption (AUDIT-C) (P = .18). MDD-PTSD+ patients reported lower social support than MDD patients (P < .001).
Considering psychiatric symptomatology, nearly 60% of participants reported feeling anxious, and 20% reported a panic attack in the previous month. When compared to MDD patients, significantly greater proportions of MDD-PTSD+ patients sanctioned the anxiety item (50% vs. 83%, P < .001) and past month panic (10% vs. 45%, P < .001). As hypothesized, MDD-PTSD+ patients evinced significantly worse depression (P < .001) and a greater percentage of these patients reported suicidal ideation (43% vs. 23%, P < .001).
We examined self-reported health care utilization intensity in the 6 months preceding baseline in 2 ways; we compared the proportions of patients who reported any health care visits, and we examined their number of visits (Table 2). Compared to MDD patients, MDD-PTSD+ patients were more likely to report any outpatient care (78% vs. 67%, P = .006), and they reported more visits (6.8 vs. 3.6, P < .001). A similar pattern of difference in outpatient visits was observed for emotional and physical problems, as higher proportions of MDD-PTSD+ patients reported any visit for problems in both areas (emotional: 15% vs. 48%, P < .001; physical: 65% vs. 74%, P = .02). Whereas MDD-PTSD+ patients reported more visits for emotional problems (2.5 vs. 0.4, P < .001), numbers of physical problem visits did not differ significantly.
Table 2.
Bivariate Comparisons: Self-reported Healthcare Utilization for PTSD Screen Negative and Screen Positive Participants*
| PTSD screen negative (n = 433) | PTSD screen positive (n = 244) | p† | |
|---|---|---|---|
| Outpatient visits | |||
| Any visit (%) | 67.3 | 78.0 | .006 |
| Visit for emotional problem (%) | 15.4 | 47.5 | <.001 |
| Visit for physical problem (%) | 65.2 | 74.3 | .02 |
| Mean number of visits (SD) | 3.6 (6.6) | 6.8 (10.2) | <.001 |
| Mean number of visits: emotional problem (SD) | 0.4 (1.6) | 2.5 (5.0) | <.001 |
| Mean number of visits: physical problem (SD) | 3.2 (6.3) | 4.3 (7.5) | .04 |
| Inpatient admissions | |||
| Any admission (%) | 24.4 | 18.5 | .10 |
| Any admission: emotional problem (%) | 3.0 | 3.9 | .60 |
| Any admission: physical problem (%) | 23.8 | 17.4 | .07 |
| Emergency room visits | |||
| Any emergency department visit (%) | 27.4 | 25.3 | .56 |
| Emergency room visit: emotional problem (%) | 2.2 | 6.2 | .01 |
| Emergency room visit: physical problem (%) | 26.3 | 24.0 | .52 |
*Data are adjusted for population weights and probability of enrollment.
†Significance testing included X2analyses for categorical data and t tests for continuous data.
Similar proportions of patients in both groups reported inpatient hospital care. Although overall percentages of self-reported emergency department visits were similar, a significantly greater proportion of MDD-PTSD+ patients (6.2% vs. 2.2%, P = .01) reported emergency department visits for an emotional problem.
Multivariate Analyses
In multivariate analyses (Table 3), the relations between PTSD screen status and each variable of interest were modeled separately. After controlling for sociodemographic differences between patient groups, physical illness comorbidity was no longer significant. In contrast, a positive PTSD screen was associated with significantly worse depressive symptomatology (P < .001), and after controlling for depressive severity, MDD-PTSD+ patients were twice as likely to report current suicidal thinking than MDD patients (OR = 2.00, P = .001). MDD-PTSD+ patients reported significantly lower levels of social support (P = .012). Finally, analyses (data not shown) failed to observe a significant difference between patient groups with regard to satisfaction with care for emotional and physical problems.
Table 3.
Multivariate Comparisons: PTSD Screen Regressed on Illness Characteristics and Social Support *
| Model | PTSD screen (0 = negative, 1 = positive) | |||
|---|---|---|---|---|
| Ordinary least squares regression | Coefficient | SE | 95% CI | p |
| Physical comorbidity (SIC) | −0.23 | 0.25 | −0.72–0.26 | .36 |
| Social support (MOS SSS)† | −0.26 | 0.10 | −0.47 to −0.06 | .012 |
| Depressive severity (PHQ-9) | 2.65 | 0.37 | 1.93–3.37 | <.001 |
| Logistic regression | OR | SE | 95% CI | p |
| Suicidal ideation‡ (0 = no, 1 = yes) | 2.00 | 0.43 | 1.31–3.05 | .001 |
*Analyses adjusted for age, gender, ethnicity, marital status, level of education, and work status and population weights.
†Lower values denote less social support.
‡Analyses also adjusted for physical comorbidity (i.e., SIC) and depressive severity (i.e., PHQ-8).
To evaluate the specificity of the relationship between comorbid PTSD and depressive severity, we examined the simultaneous contributions of PTSD, past month panic, and a multiplicative PTSD × panic interaction. PTSD (coefficient = 1.88, 95% CI = 1.04–2.72, P < .001) and panic (coefficient = 1.95, 95% CI = 0.53–3.37, P < .01) evidenced independent relations with depression. The interaction was not significant, suggesting that panic among MDD-PTSD+ patients did not represent a particularly problematic depressogenic combination.
After controlling for demographic characteristics and physical illness comorbidity, MDD-PTSD+ patients reported significantly more frequent outpatient health care visits (IRR = 1.62, P < .001) (Table 4). There was no apparent difference in frequency of visits for physical health, but MDD-PTSD+ patients reported significantly more frequent outpatient care for emotional problems (IRR = 4.01, P < .001). Results of logistic regression did not observe a statistically significant association between likelihood of inpatient admission and PTSD screen status.
Table 4.
Multivariate Analyses: PTSD Screen Regressed on Health Care Utilization Variables*
| Model | PTSD screen (0 = negative, 1 = positive) | |||
|---|---|---|---|---|
| Poisson regression | IRR | SE | 95% CI | p |
| Total outpatient visits† | 1.62 | 0.19 | 1.28–2.04 | <.001 |
| Outpatient visits: physical health | 1.24 | 0.10 | 0.96–1.61 | .101 |
| Outpatient visits: emotional health | 4.01 | 0.94 | 2.53–6.36 | <.001 |
| Logistic regression | OR | SE | 95% CI | p |
| Any inpatient admission | 0.90 | 0.22 | 0.56–1.44 | .675 |
IRR = incidence rate ratio.
*Analyses adjusted for age, gender, ethnicity, marital status, level of education and work status, clinic site clustering, and population weights.
†Also adjusted for physical comorbidity (SIC).
DISCUSSION
Depression clinical practice guidelines like the VA/DOD’s9 focus on patients with depression alone and recommend specialty mental health referral when comorbid psychiatric disorders (e.g., PTSD or other anxiety disorders) appear likely. Although some occasions might warrant specialty care, the fact that 36% of our depressed primary care sample had probable concurrent PTSD suggests that general medicine practitioners will regularly encounter these comorbid patients. As a result, practitioners should understand that comorbid patients might present differently from those with depression alone and how these differences might impact treatment planning and outcome.
Considering sociodemographic characteristics, patients with positive PTSD screens were younger, better educated, and more likely to be disabled than patients with depression alone. PTSD screen positive patients were more severely depressed, and consistent with previous work,39,40 they were significantly more likely to report current thoughts about suicide—even after controlling for other depressive symptoms.
The apparent fact that MDD-PTSD+ patients are numerous raises important issues for depression management in general medical settings. First, unlike MDD, which is characterized by a cyclical course, PTSD is more persistent and unremitting. Because many patients treated for PTSD demonstrate lingering psychiatric symptomatology,28 MDD-PTSD comorbid patients treated using depression clinical practice guidelines might be less likely than those with depression alone to experience full remission. As illustrated in a recently published report,41 relative to patients with depression alone, depressed patients with PTSD experienced a delayed response to an effective primary care–based depression intervention. Similarly, PTSD comorbidity predicted worse short-term outcomes in an investigation of hospitalized depressed patients.42
Positive PTSD screens were associated with increased prevalence of suicidal ideation. Lower social support and higher disability prevalence among MDD-PTSD+ patients represented additional suicide risk factors that have been cited by others.43–45 MDD-PTSD+ patients reported more frequent outpatient health care for emotional problems. It appears that these patients either presented more frequently to primary care for emotional problems or received additional specialty mental health care. Collectively, these results suggest that close monitoring of MDD-PTSD+ patients is advisable to ensure patient safety.
A recent metaanalysis46 documented the short-term benefit of several structured psychotherapeutic interventions for PTSD. For example, 1 study47 supported the effectiveness of cognitive processing therapy as a treatment for MDD-PTSD comorbid female sexual assault victims. Empirical support plus PTSD’s relatively poor prognosis suggest that psychotherapeutic interventions for comorbid primary care patients might have considerable utility.
Many in the present sample reported panic attacks and feeling anxious. When considering our results’ specificity to PTSD, our participants with panic evidenced higher depressive severity than those without. Coupled with previous work,48 this finding suggests that comorbid panic might also complicate primary care–based depression treatment. Notwithstanding this possibility, MDD-PTSD+ patients who reported panic did not experience worse depression than those who did not. When interpreting this finding, it is important to note that our panic and general anxiety indicators had unknown sensitivity and specificity.
Our results confirmed the expectation that comorbid PTSD would be associated with worse depression and increased health care utilization. We believe, therefore, that this work adds to the literature49,50 regarding the effects of comorbid anxiety disorders on depression and care utilization among primary care patients. Ultimately, additional research should clarify relationships between depression and PTSD/other anxiety disorders among primary care patients.
The present study has several limitations. First, our sample included male VA patients who averaged 65 years old. Given the combat exposure likelihood among VA patients, our PTSD prevalence estimate might differ from that observed in non-VA clinics. Similarly, PTSD trauma precipitants might differ across health care venues and gender. Whereas combat-related precipitants are common among VA PTSD patients, sexual assault and rape are modal precipitants among women.51 Despite the possibility that different precipitants might evince different degrees of stress severity,51 we maintain that any comorbid PTSD might complicate depression care. Future research in primary care should clarify the function and impact of MDD-PTSD comorbidity across gender, age, and traumatic precipitants.
Second, a symptom measure and a screening tool provided our MDD and probable PTSD definitions, respectively. Moreover, our design prohibited determination of the temporal relation between PTSD and MDD symptomatology. Some MDD and PTSD patients might have been misidentified, and for comorbid cases, it was unclear which illness was primary. Our results remain informative despite these ambiguities. Specifically, our patients resembled those that general medicine providers will encounter in practice. Because even minor depression and subthreshold PTSD lead to functional impairment,52–54 it is likely that our participants experienced clinically significant symptoms that warranted treatment.
In summary, depressed patients with positive PTSD screens present differently from those with depression alone. Relative to what is known about effective primary care–based depression treatment,55,56 less is known about primary care treatment of PTSD and MDD-PTSD comorbidity. Whereas some comorbid patients will respond to depression-specific treatments, others might require a “stepped-care” approach that incorporates psychotherapy57 or referral. In an effort to streamline care and maximize outcomes, future research should examine which patients will respond to standard depression treatment and which will require a stepped approach combining depression treatment and PTSD-specialized care. At a minimum, however, general medicine practitioners should examine the possibility of comorbid PTSD among their depressed patients.
In closing, we would like to highlight the present results’ relevance to non-VA care providers. First, as noted above, noncombat PTSD has the potential to complicate depression care. Second, because 45% of the present sample received non-VA medical care, many non-VA practitioners will encounter depressed patients with combat-related PTSD. This becomes increasingly likely given that psychiatric morbidity prevalence estimates among veterans of present US military conflicts range between 17% and 19%.58,59 As soldiers from Iraq and Afghanistan become war veterans and health care consumers, the presentation of traumatized and depressed patients in non-VA medical practices has the potential to increase.
Acknowledgments
The results reported here were from the Well-Being Among Veterans Enhancement Study (WAVES). WAVES received financial support from a grant (MHI 99-375: Chaney EF & Rubenstein LV, Co-PIs) from the Department of Veterans Affairs, Health Services Research and Development (HSR& D). An HSR& D Postdoctoral Traineeship (Campbell) provided additional support. The views expressed here are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs, the University of Montana, the University of Washington, the University of California Los Angeles, or the RAND Health Program. Portions of this project were presented at the Department of Veterans Affairs HSR& D National Annual Meeting (2005, February), Baltimore, MD. The authors wish to acknowledge the contributions of Robert Petzel, MD; Kathy Henderson, MD; Scott Ober, MD; Maurilio Garcia-Maldinado, MD; Laura M. Bonner, PhD; Barbara Simon, MA; Carol Simons; and the WAVES research group.
Potential Financial Conflicts of Interest Dr. Felkier reported receiving honoraria from Pfizer for speaking. Dr. Chaney reported receiving honorarium from The RAND Corporation for article review. The other authors reported no conflicts of interest.
References
- 1.Rost K, Zhang M, Fortney J, Smith J, Coyne J, Smith GR. Persistently poor outcomes of undetected major depression in primary care. Gen Hosp Psych. 1998;20:12–20. [DOI] [PubMed]
- 2.Simon GE, Von Korff M, Wagner EH, Barlow W. Patterns of antidepressant use in community practice. Gen Hosp Psych. 1993;15:399–408. [DOI] [PubMed]
- 3.Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psych. 1992;14:237–47. [DOI] [PubMed]
- 4.Olfson M, Shea S, Feder A, et al. Prevalence of anxiety, depression, and substance use disorders in an urban general medicine practice. Arch Fam Med. 2000;9:876–83. [DOI] [PubMed]
- 5.Wells KB, Hays RD, Burnam A, et al. Detection of depressive disorder for patients receiving prepaid or fee-for-service care: results from the medical outcomes study. JAMA. 1989;262:3298–303. [DOI] [PubMed]
- 6.Olfson M, Marcus SC, Druss B, Elinson L, Tanielian T, Pincus H. National trends in the outpatient treatment of depression. JAMA. 2002;287:203–9. [DOI] [PubMed]
- 7.Depression Guideline Panel. Clinical practice guideline number 5: depression in primary care, volumes 1 & 2. Rockville, MD: US Department of Health and Human Services, Agency for Health Care Policy and Research; 1993. AHCPR Publications 93-0550-51.
- 8.American Psychiatric Association Workgroup on Major Depressive Disorder. Practice guideline for the treatment of patients with major depressive disorder, 2nd edition. Washington: 2000; American Psychiatric Publishing, Inc. Website: http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- 9.The Management of Major Depressive Disorder Working Group. Veterans Health Administration/Department of Defense clinical practice guideline for the management of major depressive disorder in adults. Version 2.0, February 2000, Washington DC.
- 10.Bruce ML, Ten Have TR, Reynolds III CF, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291:1081–91. [DOI] [PubMed]
- 11.Katon W, Rutter C, Ludman EJ, et al. A randomized trial of relapse prevention of depression in primary care. Arch Gen Psychiatry. 2001;58:241–7. [DOI] [PubMed]
- 12.Whooley MA, Simon GE. Managing depression in medical outpatients. NEJM. 2000;343:1942–50. [DOI] [PubMed]
- 13.Rollman BL, Weinreb L, Korsen N, Schulberg HC. Implementation of guideline-based care for depression in primary care. Adm Policy Ment Health. 2006;33:43–53. [DOI] [PubMed]
- 14.Cabana MD, Rushton JL, Rush AJ. Implementing practice guidelines for depression: Applying a new framework to an old problem. Gen Hosp Psych. 2002;24:35–42. [DOI] [PubMed]
- 15.Magruder KM, Frueh BC, Knapp RG, et al. Prevalence of posttraumatic stress disorder in Veterans Affairs primary care clinics. Gen Hosp Psych. 2005;27:169–79. [DOI] [PubMed]
- 16.Dobie DJ, Kivlahan DR, Maynard C, et al. Screening for post-traumatic stress disorder in female Veterans Affairs patients. Gen Hosp Psych. 2002;24:367–74. [DOI] [PubMed]
- 17.Hankin CS, Spiro III A, Miller DR, Kazis L. Mental disorders and mental health treatment among US Department of Veterans Affairs outpatients: the Veterans Health Study. Am J Psychiatry. 1999;156:1924–30. [DOI] [PubMed]
- 18.Stein MB, McQuaid JR, Pedrelli P, Lenox R, McCahill ME. Posttraumatic stress disorder in the primary care medical setting. Gen Hosp Psych. 2000;22:261–9. [DOI] [PubMed]
- 19.Taubman-Ben-Ari O, Rabinowitz J, Feldman D, Vaturi R. Post-traumatic stress disorder in primary-care settings: prevalence and physician’s detection. Psychol Med. 2001;31:555–60. [DOI] [PubMed]
- 20.Davidson JRT, Hughes D, Blazer DG, George LK. Post-traumatic stress disorder in the community: an epidemiological study. Psychol Med. 1991;21:713–21. [DOI] [PubMed]
- 21.Magruder KM, Frueh BC, Knapp RG, et al. PTSD symptoms, demographic characteristics, and functional status among veterans treated in VA primary care clinics. J Trauma Stress. 2004;17:293–301. [DOI] [PubMed]
- 22.Nixon RDV, Resick PA, Nishith P. An exploration of comorbid depression among female victims of intimate partner violence with posttraumatic stress disorder. J Affect Disord. 2004;82:315–20. [DOI] [PMC free article] [PubMed]
- 23.Blanchard EB, Buckley TC, Hickling EJ, Taylor AE. Posttraumatic stress disorder and comorbid major depression: Is the correlation an illusion? J Anxiety Disord. 1998;12:21–37. [DOI] [PubMed]
- 24.Boudreaux E, Kilpatrick DG, Resnick HS, Best CL, Saunders BE. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665–78. [DOI] [PubMed]
- 25.Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52:1048–60. [DOI] [PubMed]
- 26.Hankin CS, Spiro III A, Miller DR, Kazis L. Mental disorders and mental health treatment among US Department of Veterans Affairs outpatients: the Veterans Health Study. Am J Psychiatry. 1999;156:1924–30. [DOI] [PubMed]
- 27.Office of Quality and Performance. FY2005 VA Performance Measurement System Technical Manual. Washington, DC: Department of Veterans Affairs, Veterans Health Administration; 2005.
- 28.Zlotnick C, Rodriquez BF, Wiesberg RB, et al. Chronicity in posttraumatic stress disorder and predictors of the course of posttraumatic stress disorder among primary care patients. J Nerv Ment Dis. 2004;192:153–9. [DOI] [PubMed]
- 29.Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. JGIM. 2001;16:606–13. [DOI] [PMC free article] [PubMed]
- 30.Nease Jr DE, Malouin JM. Depression screening: a practical strategy. J Fam Pract. 2003;52:118–26. [PubMed]
- 31.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed.). Washington, DC: American Psychiatric Association; 1994:327.
- 32.Prins A, Ouimette P, Kimmerling R, et al. The primary care PTSD screen (PC-PTSD): development and operating characteristics. Prim Care Psychiatry. 2003;9:9–14. [DOI]
- 33.Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT Alcohol Consumption Questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med. 1998;158:1789–95. [DOI] [PubMed]
- 34.Bradley KA, Maynard C, Kivlahan DR, et al. The relationship between alcohol screening questionnaires and mortality among male VA outpatients. J Stud Alcohol. 2001;62:826–33. [DOI] [PubMed]
- 35.Kazis LE, Ren XS, Lee A, et al. Health status in VA patients: results from the Veterans Health Study. Am J Med Qual. 1999;14:28–38. [DOI] [PubMed]
- 36.Fan VS, Au D, Heagerty P, Deyo RA, McDonnell MB, Fihn SD. Validation of case-mix measures derived from self-reports of diagnoses and health. J Clin Epidemiol. 2002;55:371–80. [DOI] [PubMed]
- 37.Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32:705–14. [DOI] [PubMed]
- 38.Meredith LS, Orland M, Humphrey N, Camp P, Sherbourne CD. Are better ratings of the patient–provider relationship associated with higher quality care for depression? Med Care. 2001;39:349–60. [DOI] [PubMed]
- 39.Oquendo MA, Friend JM, Halberstam B, et al. Association of comorbid posttraumatic stress disorder and major depression with greater risk for suicidal behavior. Am J Psychiatry. 2003;160:580–2. [DOI] [PubMed]
- 40.Oquendo M, Brent DA, Birmaher B, et al. Posttraumatic stress disorder comorbid with major depression: factors mediating the association with suicidal behavior. Am J Psychiatry. 2005;162:560–6. [DOI] [PubMed]
- 41.Hegel MT, Unutzer J, Tang L, et al. Impact of comorbid panic and posttraumatic stress disorder on outcomes of collarborative care for late-life depression in primary care. Am J Geriatr Psychiatry. 2005;13:48–58. [DOI] [PubMed]
- 42.Holtzheimer PE, Russo J, Zatzick D, Bundy C, Roy-Byrne PP. The impact of comorbid posttraumatic stress disorder on short-term outcome in hospitalized patients with depression. Am J Psychiatry. 2005;162:970–6. [DOI] [PubMed]
- 43.Lara ME, Leader J, Klein DN. The association between social support and course of depression: is it confounded with personality? J Abnorm Psychology. 1997;106:478–82. [DOI] [PubMed]
- 44.Oslin DW, Datto CJ, Kallan MJ, Katz IR, Edell WS, TenHave T. Association between medical comorbidity and treatment outcomes in late-life depression. J Am Geriatr Soc. 2002;50:823–8. [DOI] [PubMed]
- 45.Turvey CL, Conwell Y, Jones MP, et al. Risk factors for late-life suicide: a prospective, community-based study. Am J Geriatr Psychiatry. 2002;10:398–406. [DOI] [PubMed]
- 46.Bradley R, Greene J, Russ E, Dutra L, Westen D. A multidimensional meta-analysis of psychotherapy for PTSD. Am J Psychiatry. 2005;162:214–27. [DOI] [PubMed]
- 47.Nishith P, Nixon RDV, Resick PA. Resolution of trauma-related guilt following treatment of PTSD in female rape victims: a result of cognitive processing therapy targeting comorbid depression. J Affect Disord. 2005;86:259–65. [DOI] [PMC free article] [PubMed]
- 48.Felker BL, Hedrick SC, Chaney EF, et al. Identifying depressed patients with a high risk of comorbid anxiety in primary care. Prim Care Companion J Clin Psychiat. 2003;5:104–10. [DOI] [PMC free article] [PubMed]
- 49.Gaynes BN, Magruder KM, Burns BJ, Wagner HR, Yarnall KSH, Broadhead WE. Does a coexisting anxiety disorder predict persistence of depressive illness in primary care patients with major depression? Gen Hosp Psych. 1999;21:158–67. [DOI] [PubMed]
- 50.Sherbourne CD, Wells KB. Course of depression in patients with comorbid anxiety disorders. J Affect Disord. 1997;43:245–50. [DOI] [PubMed]
- 51.Norris FH. Epidemiology of trauma: frequency and impact of different potentially traumatic events of different demographic groups. J Consult Clin Psychol. 1992;60:409–18. [DOI] [PubMed]
- 52.Grubaugh AL, Magruder KM, Waldrop AE, Elhai JD, Knapp RG, Frueh BC. Subthreshold PTSD in primary care: prevalence, psychiatric disorders, healthcare use, and functional status. J Nerv Ment Dis. 2005;193:658–64. [DOI] [PubMed]
- 53.Backenstrass M, Frank A, Joest K, Hingmann S, Mundt C, Kronmüller K. A comparative study of nonspecific depressive symptoms and minor depression regarding functional impairment and associated characteristics in primary care. Compr Psychiatry. 2006;47:35–41. [DOI] [PubMed]
- 54.Stein MB, Walker JR, Hazen AL, et al. Full and partial posttraumatic stress disorder: findings from a community survey. Am J Psychiatry. 1997;154:1114–9. [DOI] [PubMed]
- 55.Herbeck Belnap B, Kuebler J, Upshur C, et al. Challenges of implementing depression care management in the primary care setting. Administration and Policy in Mental Health and Mental Health Services Research. 2006;33:65–75. [DOI] [PubMed]
- 56.Kilbourne AM, Rollman BL, Schulberg HC, Herbeck Belnap B, Pincus HA. A clinical framework for depression treatment in primary care. Psychiatr Ann. 2002;32:545–53.
- 57.Davidson JRT, Connor KM. Management of posttraumatic stress disorder: diagnostic and therapeutic issues. J Clin Psychiatry. 1999;60:33–8. [PubMed]
- 58.Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems and barriers to care. NEJM. 2004;351:13–22. [DOI] [PubMed]
- 59.Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA. 2006;295:1023–32. [DOI] [PubMed]