

Abstract
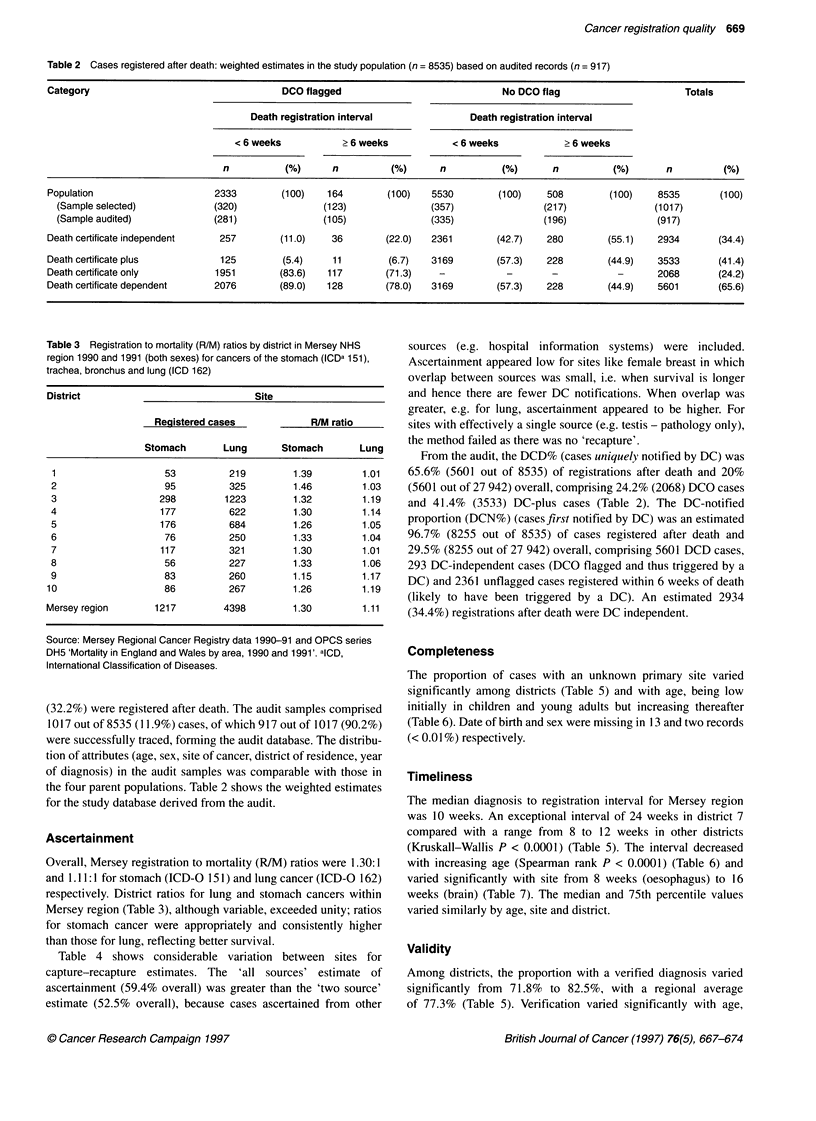
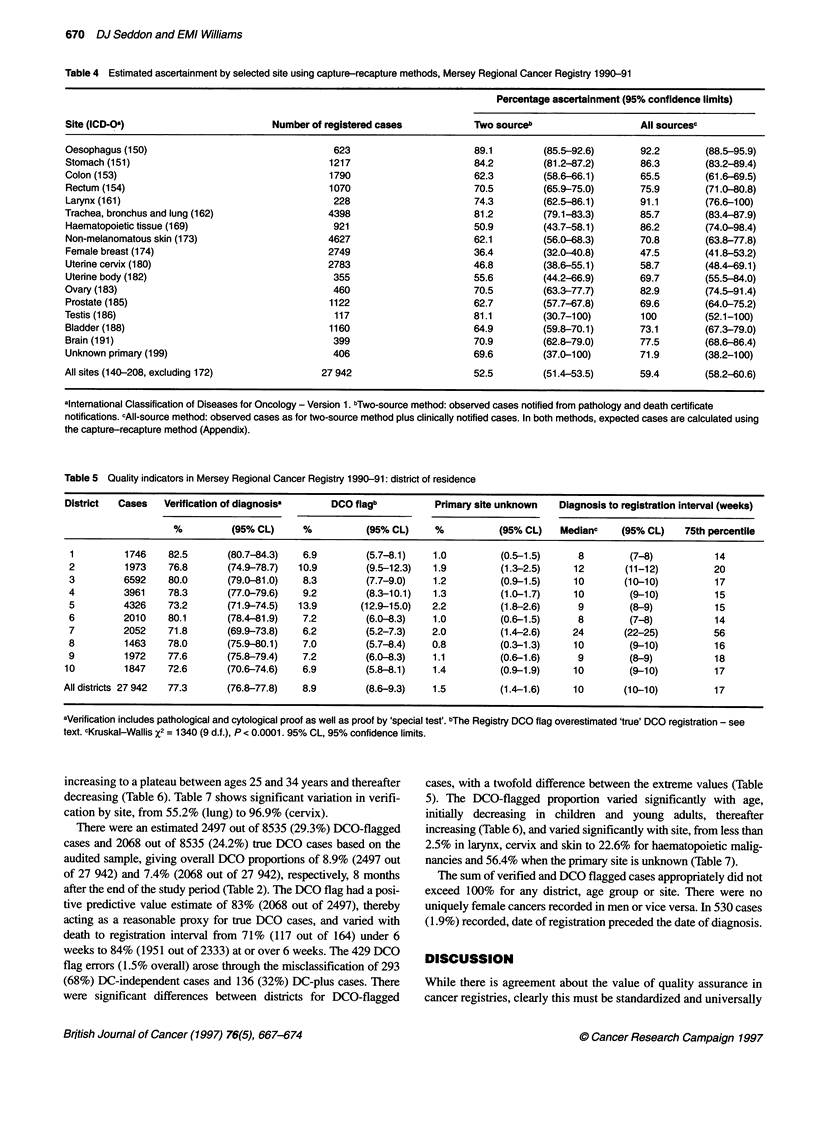
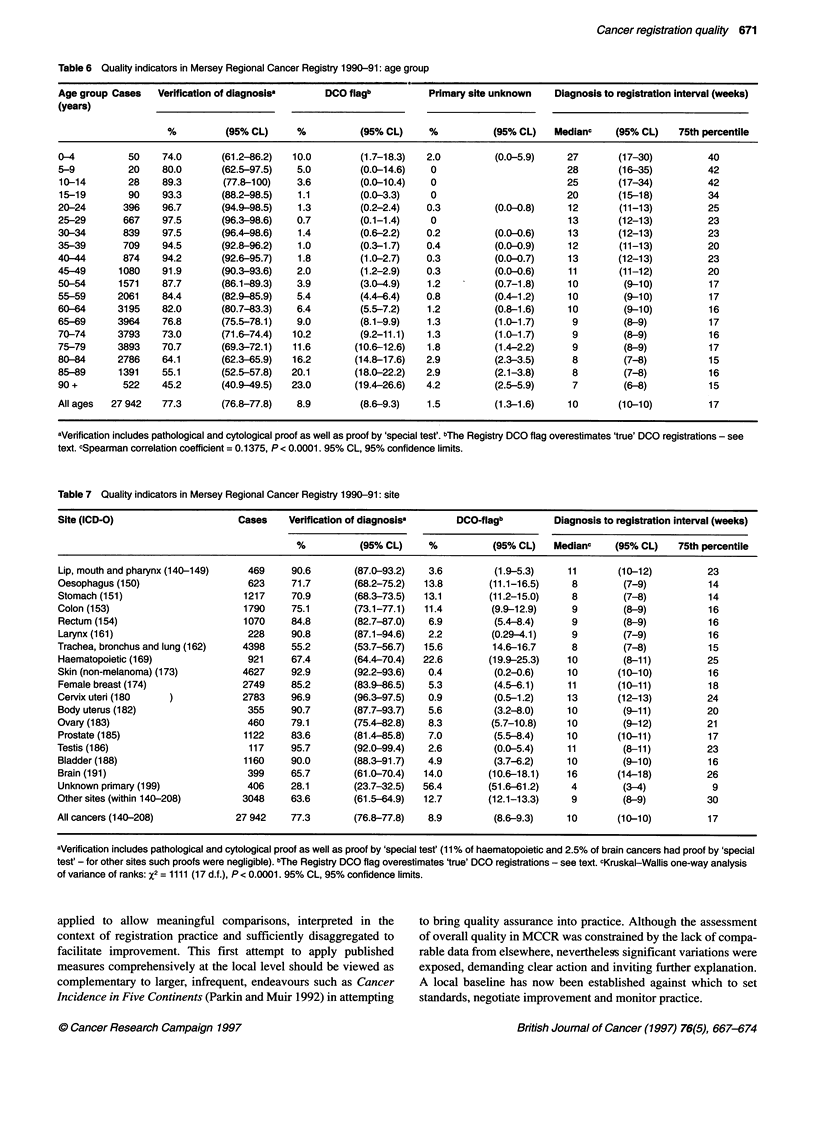
Merseyside and Cheshire Cancer Registry (MCCR) data quality was assessed by applying literature-based measures to 27,942 cases diagnosed in 1990 and 1991. Registrations after death (n = 8535) were also audited (n = 917) to estimate death certificate only (DCO) case accuracy and the proportion of registrations notified by death certificate (DC). Ascertainment appeared to be high from the registration/mortality ratio for lung [1.01:1] and to be low from capture-recapture estimates (59.4%), varying significantly with site from oesophagus [92.2% (95% CI 88.5-95.9)] to breast [47.5 (95% CI 41.8-53.2)]. The estimated DC-dependent proportion was 20% (5601 out of 27 942) with successful traceback in 3533 out of 5601 (63.1%) cases. DCO flagging (2497 out of 27,942, 8.9%) overestimated true DCO cases (2068 out of 27,942, 7.4%). The proportion of cases of unknown primary site was low (1.5%), varying significantly with age [0-4.2%, (95% CI 2.5-5.9)] and district [0.8% (95% CI 0.3-1.3) to 2.2% (95% CI 1.8-2.6)]. The median diagnosis to registration interval appeared to be good (10 weeks), varying significantly with site (P < 0.0001), age (P < 0.0001) and district (P < 0.0001). The proportion with a verified diagnosis was 77.3%, varying significantly with site [lung 55.2% (95% CI 53.7-56.7) to cervix 96.9% (95% CI 96.3-97.5)], age [45.2% (95% CI 40.9-49.5) to 97.5% (95% CI 96.4-98.6)] and district [71.8% (95% CI 69.9-73.8) to 82.5% (95% CI 80.7-84.3)]. The DCO percentages varied similarly by site [non-melanoma skin 0.4% (95% CI 0.2-0.6) to lung 22.6% CI (95% 19.9-25.3)], age [0.7(95% CI 0.1-1.4) to 23.0 (95% CI 19.4-26.6)] and district [6.9% (95% CI 5.7-8.1) to 13.9% (95% CI 12.9-15.0)]. MCCR data quality varied with age, site and district - inviting action - and apparently compares favourably with elsewhere, although deficiencies in published data hampered definitive assessment. Putting quality assurance into practice identified shortcomings in the scope, definition and application of existing measures, and absent standards impeded interpretation. Cancer registry quality assurance should henceforward be within an explicit framework of agreed and standardized measures.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Balarajan R., Scott A. National cancer registration: an appraisal. Community Med. 1983 Feb;5(1):31–37. doi: 10.1007/BF02548581. [DOI] [PubMed] [Google Scholar]
- Benn R. T., Leck I., Nwene U. P. Estimation of completeness of cancer registration. Int J Epidemiol. 1982 Dec;11(4):362–367. doi: 10.1093/ije/11.4.362. [DOI] [PubMed] [Google Scholar]
- Day N. E., Davies T. W. Cancer registration: integrate or disintegrate? BMJ. 1996 Oct 12;313(7062):896–896. doi: 10.1136/bmj.313.7062.896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman L. S. Variations in the level of reporting by hospitals to a regional cancer registry. Br J Cancer. 1978 May;37(5):861–865. doi: 10.1038/bjc.1978.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkins M. M., Swerdlow A. J. Completeness of cancer and death follow-up obtained through the National Health Service Central Register for England and Wales. Br J Cancer. 1992 Aug;66(2):408–413. doi: 10.1038/bjc.1992.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robles S. C., Marrett L. D., Clarke E. A., Risch H. A. An application of capture-recapture methods to the estimation of completeness of cancer registration. J Clin Epidemiol. 1988;41(5):495–501. doi: 10.1016/0895-4356(88)90052-2. [DOI] [PubMed] [Google Scholar]