

Abstract
Between April 1979 and August 1993, we treated 39 patients (49 knees) with knee flexion deformity after Poliomyelitis. All were subjected to fractional hamstring lengthening and supracondylar femoral extension osteotomy in the same surgical procedure. The goal was to correct the deformity and fit the lower extremities in long braces to improve or promote gait. Patients′ mean age was 19.5 (6.5–39) years and the mean knee flexion deformity was 65° (24–158°). The mean follow-up was 15.5 (11.5–25) years. Postoperatively, 22 knees had full extension, in 26 there was an extension lag between −1 and −10° and in one a lag greater than 10°. There were no neurovascular complications and all patients were fitted with long leg braces. Surgical planning is important, especially in severe deformities, where shortening of the femur is necessary to facilitate the osteotomy and relax the neurovascular structures.
Résumé
Entre avril 1979 et août 1993, nous avons traité 39 malades (49 genoux) avec flessum du genou après Poliomyélite. Tous ont été soumis à un allongement fractionné des tendons ischiojambiers et une ostéotomie d'extension supracondylienne du fémur dans le même temps opératoire. Le but était de corriger la déformation et d'adapter le membre inférieur à un appareillage pour permettre ou améliorer la marche. L'âge moyen des malades était 19,5 (6,5–39) années et le flessum moyen du genou était de 65° (24°–158°). La moyenne de suivi était 15,5 (11,5–25) années. Après l'opération 22 genoux avaient une extension complète, 26 avaient un défaut d'extension entre 1 et 10° et un genou avait un défaut de plus de 10°. Il n'y avait aucune complication neurovasculaire et tous les malades ont pu être appareillés avec des orthèses cruro-pédieuses. La planification chirurgicale est importante dans les déformations sévères où raccourcir le fémur est nécessaire pour faciliter l'ostéotomie et surtout pour détendre les structures neurovasculaires.
Introduction
Poliomyelitis is a rare disease in developed countries nowadays, but in many countries, including Brazil, there are still patients with late sequelae of this condition, the majority being adults.
The quadriceps paralysis seen in poliomyelitis causes a major handicap to the patient, who will need the hand as support on the thigh in order to walk. The muscle imbalance induced by the quadriceps paralysis, with normal or subnormal muscle power of the hamstrings, will lead to a knee flexion deformity. Depending on its severity this deformity will prevent the use of a long caliper that could otherwise stabilize the knee during gait. The knee will also develop morphological changes of the femoral and tibia condyles, which become flattened. The patella will assume the shape of a wedge as it does not move over the intercondylar groove during flexion and extension. As a consequence, patients are not able to extend their knees completely, but retain a reduced range of movement, which is unfavourable for walking [1–3, 6, 8, 9].
This retrospective study aims to show the long-term results of patients treated for knee flexion deformities as late sequelae of Poliomyelitis. The retrospective research protocol was reviewed and approved by The Ethics Medical Board of the Santa Casa Hospitals.
Material and methods
Between April 1979 and August 1993, 39 patients (49 knees) with knee flexion deformity following Poliomyelitis were subjected to a fractional hamstring lengthening and a supracondylar femoral extension osteotomy. In 29 patients the deformity was unilateral and in 10 bilateral. There were 24 right-sided and 25 left-sided deformities. There were 20 male and 19 female patients. The average age at surgery was 19.5 years (range 6.5–39 years). Functionally, 31 patients were able to walk with the hand on the thigh and eight were non-walkers.
Patients were evaluated clinically and radiographically. The radiographic preoperative mean knee flexion deformity was 65° (24–158°; Table 1).
Table 1.
Patients' distribution according to preoperative knee flexion deformity
| Preoperative knee flexion contracture | Number of knees (n) |
|---|---|
| 20–39° | 10 |
| 40–59° | 14 |
| 60–79° | 10 |
| 80–99° | 6 |
| 100–119° | 6 |
| 120–139° | 2 |
| 140–159° | 1 |
| Total | 49 |
Source: Medical Records of the Irmandade da Santa Casa de Misericórdia de São Paulo (M.R.I.S.C.M.S.P.)
Prior to the surgical treatment of the knee deformity, six patients underwent surgical release of the hip-flexors and/or hamstrings and two patients were treated conservatively for lengthening of the hamstrings.
All patients were subjected to a supracondylar femoral extension osteotomy and to fractional hamstring lengthening in the same surgical session. In four cases the osteotomy was performed to correct not only the flexion deformity but also any associated varus deformity, and in one case a femoral derotation was added to the procedure. Further associated surgical procedures were: hip flexor release in seven, psoas tenotomy in one, posterior tibial tendon tenotomy in one, tibial derotation osteotomy in one, Achilles tendon lengthening in seven, Steindler procedure in two, triple arthrodesis of the foot in two and a Jones procedure in one patient.
Surgical procedures that were performed later in order to correct other deformities are listed in Table 2.
Table 2.
Procedures done after the supracondylar femoral extension osteotomy
| Techniques | Number of procedures |
|---|---|
| Soutter procedure | 14 |
| Yount | 3 |
| Iliopsoas tenotomy | 3 |
| Posterior tibial tenotomy | 2 |
| Tendon transfers | |
| Peroneus brevis to the dorsum of the foot | 1 |
| Peroneus longus to the dorsum of the foot | 1 |
| Posterior tibial tendon and peroneus brevis to the dorsum of the foot | 1 |
| Anterior tibial tendon to the dorsum of the foot | 1 |
| Tibia derotation osteotomy | 3 |
| Tibia varus osteotomy | 1 |
| Achilles tendon lengthening | 19 |
| Ankle and posterior subtalar capsulotomy | 2 |
| Plantar fascia release | 4 |
| Triple arthrodesis of the foot | 10 |
| Jones procedure | 1 |
| Total | 66 |
Source: M.R.I.S.C.M.S.P.
Surgical technique
With the patient in a supine position, fractional hamstring lengthening was performed using the technique of Green and McDermott (as described in Bleck [3]). The average gain in knee extension was 10 to 15°.
The skin incision started on the lateral side of the distal third of the thigh and exposed the supracondylar area of the femur. The inferior osteotomy line was done at the supracondylar level, being extra-articular and parallel to the physis (Figs. 1, 2). The femoral shortening was on average 1.5 (0.5–2.5) cm. Two crossed Steimann pins were used to fix the osteotomy, introduced anteriorly with the knee in full extension. A long leg cast with the knee in full extension was applied and maintained until bone union was confirmed. This the patient was then fitted with a long leg brace and trained to walk.
Fig. 1.

Osteotomy in triangle form, for flexion deformities <30°
Fig. 2.

Osteotomy in trapezoid form, for major flexion deformities
Results
The mean follow-up was 15.5 (11.5–24) years. The results were analysed according to the correction of deformity and function. A result was considered satisfactory if the knee deformity was corrected and the patient experienced improvement in gait or the ability to walk. A result was considered unsatisfactory when there was a residual flexion deformity greater than 20°, with valgus or varus deviation of the knee greater than 5°, with union or nonunion of the osteotomy.
At the final follow-up a lateral radiograph of the extended knee showed 22 knees to be in neutral position, 26 knees with a deformity between −1 to 10° (Figs. 3, 4, 5, 6) and one knee with a deformity of greater than 10°.
Fig. 3.
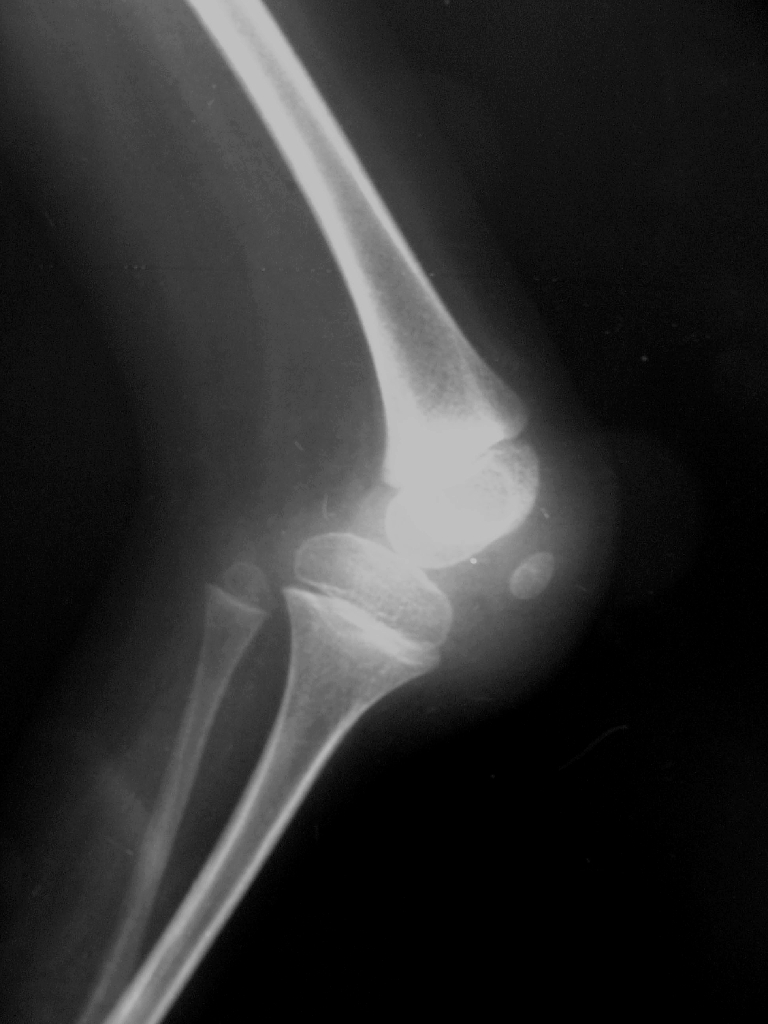
Preoperative lateral radiograph of the knee at maximum extension
Fig. 4.
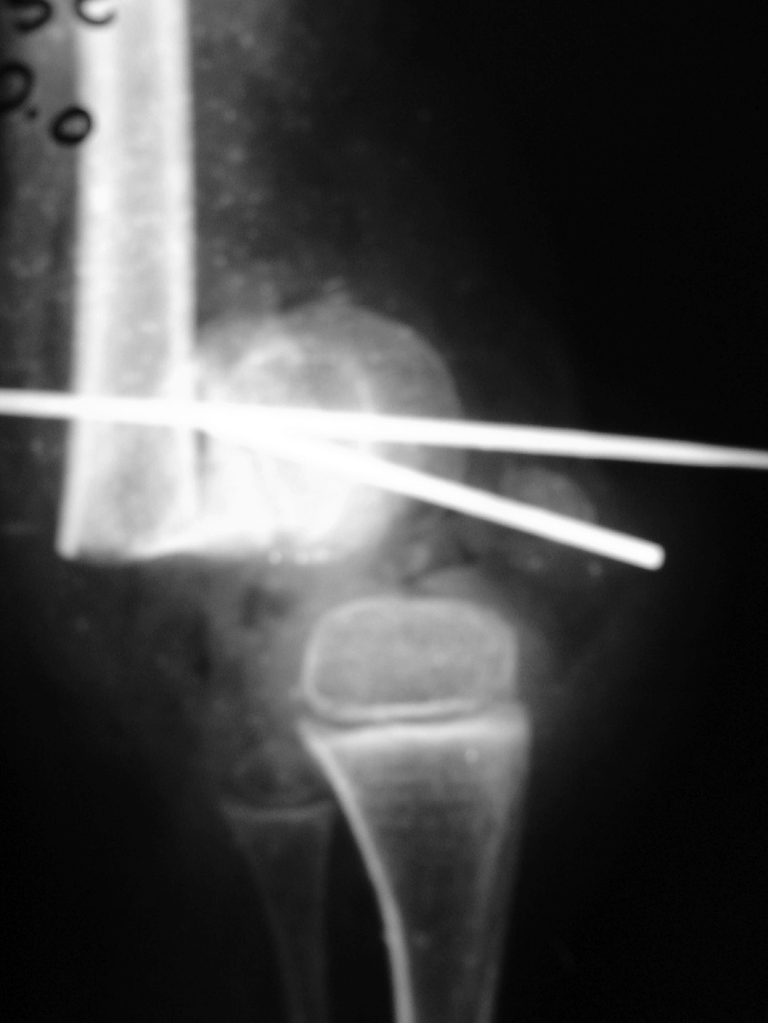
Postoperative lateral radiograph of the knee
Fig. 5.

Three years postoperatively, lateral radiograph in extension
Fig. 6.
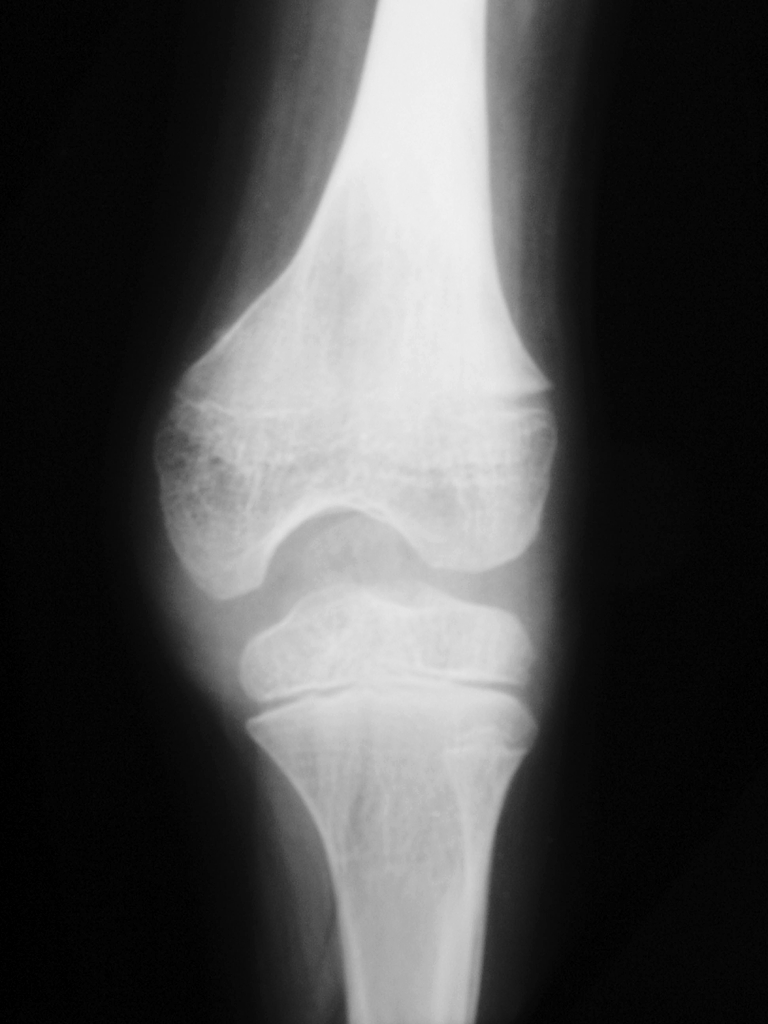
Three years postoperatively, antero-posterior radiograph
In all patients the osteotomy united in a mean time of 4 (2–10) months. One patient with bilateral osteotomies showed a delayed union on one side, which led to a second grafting procedure with union after 10 months.
Postoperatively, all patients were fitted with long leg braces for walking and became community walkers, even the two patients with residual knee flexion deformity. All patients considered the overall result to be satisfactory.
There were no vascular complications, although some of the patients had flexion deformities greater than 90°. One patient had neuropraxia of the external popliteal nerve, due to excessive manipulation during the hamstring lengthening. It resolved totally after 4 months. Two patients had superficial pin site infections, which were treated with topical care.
Discussion
The presence of a major handicap such as quadriceps paralysis following Poliomyelitis should be treated to promote or improve gait [1, 4, 6–9].
The knee flexion deformity can be treated in different ways, depending on severity and the age of the patient. Progressive correction of the knee flexion deformity by skeletal traction requires a long time in hospital. It is associated with high morbidity, such as pain, pin site infection, and posterior subluxation of the knee, and usually does not correct the deformity entirely, necessitating further surgery at a later date. Serial casting was avoided in cases of flexion deformity greater than 20°, because of its poor outcome and complications such as pressure sores, pain and subluxation of the knee.
When an osteotomy is performed, a new deformity is created in the distal femur depending on the flexion deformity. Thus, in a patient with a 90° flexion contracture, the distal fragment lies at 90° to the femoral shaft. The new relationship of the distal femur with time undergoes a process of bone remodelling, as observed in the postoperative follow-up.
In cases of flexion deformity greater than 30°, bone resection of a trapezoidal segment of the distal femur had to be made to allow the balance between soft tissue and bone fragments. In cases of more than 90° of flexion angle, the resection could be up to 2.5 cm along the short base of the trapezium, leading to shortening of the extremity, which must be compensated for by the brace.
Care should be taken that the amount of shortening is sufficient to relax the neurovascular bundle to avoid major complications.
This osteotomy allows simultaneous correction not only of the flexion deformity, but also of any associated varus, valgus or torsional deformities [5]. Care should be taken to measure the preoperative angular deviations remembering that, due to the knee flexion deformity, they can could be misinterpreted on the antero-posterior radiograph.
One concern about the long-term survival of these knee joints is the degenerative changes that could occur later. From our group of patients only two patients (three knees) presented with pain with radiographic signs of arthritis. In one patient the pain started 11 and the other 12 years years postoperatively, this latter patient complained of bilateral pain, although only the right side had been operated upon. Both patients are now being treated conservatively. Therefore, the incidence of degenerative arthritis following extension osteotomy was low despite the severity of the initial deformity.
In our series, subsequent growth did not cause any recurrence of the deformity, showing that the new range of movement is not lost over time.
The radiographic evaluation showed that we obtained a good final alignment after the supracondylar femoral extension osteotomy, even in knees that had moderate to severe contracture angles.
After the surgery, the majority of the knees obtained a final extension angle between 0° and 12°. No correlation was found between the initial deformity angle and the final outcome so that despite the initial deformity all patients ended up with full or alomost full extension. There was no direct correlation between the age at the operation and the final degree of knee extension. The same was true of gender, side affected, unilateral or bilateral deformity, or correction obtained.
In conclusion, patients with moderate to severe knee flexion deformity following Poliomyelitis are best treated by supracondylar femoral extension osteotomy with simultaneous fractional hamstring lengthening.
The need for bone resection to prevent neurovascular complications should be stressed. The procedure is technically easy and safe with good functional results, as it allows these handicapped patients to walk or improve their gait pattern. The final knee extension did not depend on age, sex, side, unilateral or bilateral and is maintained over time.
References
- 1.Abraham E, Sharrard WJW (1977) The treatment of flexion contracture of the knee in myelomeningocele. J Bone Joint Surg Br 59:433–438 [DOI] [PubMed]
- 2.Banta JV, Nichols O (1969) Sacral agenesis. J Bone Joint Surg Am 51:693–703 [PubMed]
- 3.Bleck EE (1987) Orthopaedic management in cerebral palsy, 2nd edn. MacKeith, London, p 497
- 4.Cravener EK (1930) Device for overcoming non-bony flexion contracture of the knee. J Bone Joint Surg 12:437–439
- 5.Delbello DA, Watts HG (1996) Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 16:122–126 [DOI] [PubMed]
- 6.Men H, Bian C, Yang C, Zhamg Z, Wu C, Pang B (1991) Surgical treatment of flail knee after poliomyelitis. J Bone Joint Surg Br 73:195–199 [DOI] [PubMed]
- 7.Merle d'Aubignè R, Scholder-Dumur C (1956) Traitement du flexum du genou et de la hanche chez les poliomyélitiques. Rev Chir Orthop Repar Appar Mot 42:591–620 [PubMed]
- 8.Zimmerman MH, Smith CF, Oppenheim WL (1982) Supracondylar femoral extension osteotomies in the treatment of fixed flexion deformity of the knee. Clin Orthop 171:87–93 [PubMed]
- 9.Zouari O, Gargouri A, Jenzri M, Hadinane R, Slimana N (2001) Supracondylar femoral extension osteotomy for knee flexion contracture correction in poliomyelitic conditions. Rev Chir Orthop Repar Appar Mot 87:361–636 [PubMed]