

Abstract
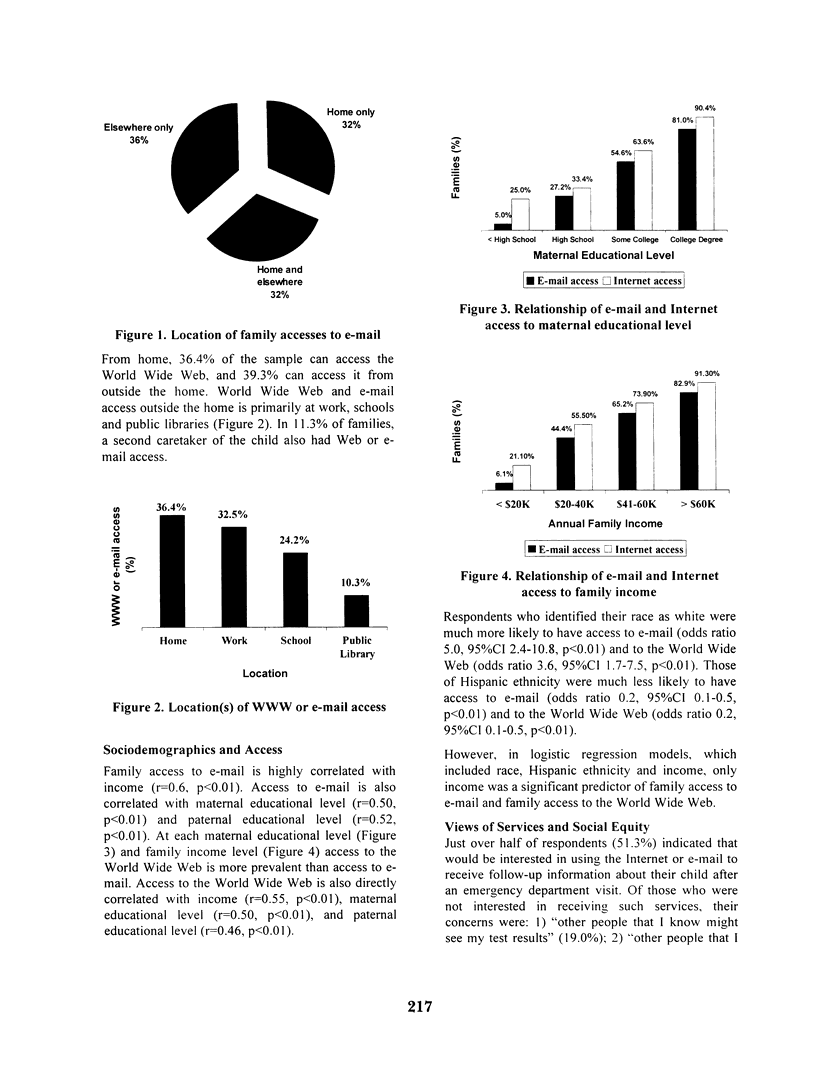
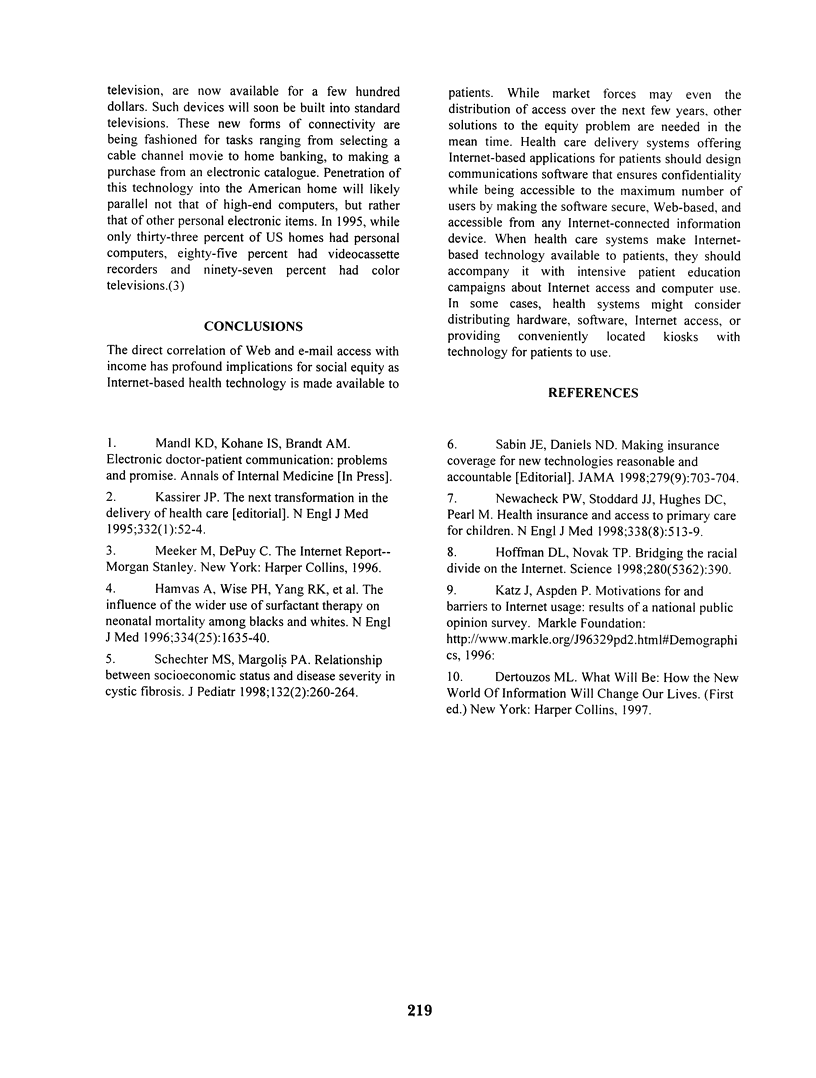
INTRODUCTION: The distribution and types of Internet connectivity will determine the equity of access by patient populations to emerging health technologies. We sought to measure the rates, types, and predictors of access in a patient population targeted for Web-based medical services. METHODS: Design. Cross sectional in-person interview. Setting. Emergency department of a large urban pediatric teaching hospital. Subjects. Primary caretakers of patients or patients at least 16 years old. Procedure and measures. Subjects were asked about access to e-mail and the Internet as well as about willingness to use and concerns about Web-based services. Views of equity and access and sociodemographic data were also elicited. RESULTS: 132 subjects were enrolled in the study. Of respondents, 67.2% use a computer and 36.4% can access the Internet or e-mail from home. Including Internet connections and/or e-mail accounts at work, school and public libraries, 50.7% of the sample has access. Forty percent of families have e-mail accounts. The rate at which families have connectivity is primarily correlated with income (r = 0.6, p < 0.01). At all income levels, rates of access to the World Wide Web are higher than to e-mail. White patients are much more likely to have e-mail (OR 5.0, 95% CI 2.4-10.8) and Web access (OR 3.6, 95% CI 1.7-7.5). CONCLUSIONS: Connectivity is directly correlated with income and distributed unevenly across racial and ethnic groups. World Wide Web access is more prevalent than e-mail accounts, and both are often obtained outside the home. Design of health applications should account for these attributes of patient access.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hamvas A., Wise P. H., Yang R. K., Wampler N. S., Noguchi A., Maurer M. M., Walentik C. A., Schramm W. F., Cole F. S. The influence of the wider use of surfactant therapy on neonatal mortality among blacks and whites. N Engl J Med. 1996 Jun 20;334(25):1635–1640. doi: 10.1056/NEJM199606203342504. [DOI] [PubMed] [Google Scholar]
- Kassirer J. P. The next transformation in the delivery of health care. N Engl J Med. 1995 Jan 5;332(1):52–54. doi: 10.1056/NEJM199501053320110. [DOI] [PubMed] [Google Scholar]
- Newacheck P. W., Stoddard J. J., Hughes D. C., Pearl M. Health insurance and access to primary care for children. N Engl J Med. 1998 Feb 19;338(8):513–519. doi: 10.1056/NEJM199802193380806. [DOI] [PubMed] [Google Scholar]
- Sabin J. E., Daniels N. Making insurance coverage for new technologies reasonable and accountable. JAMA. 1998 Mar 4;279(9):703–704. doi: 10.1001/jama.279.9.703. [DOI] [PubMed] [Google Scholar]
- Schechter M. S., Margolis P. A. Relationship between socioeconomic status and disease severity in cystic fibrosis. J Pediatr. 1998 Feb;132(2):260–264. doi: 10.1016/s0022-3476(98)70442-1. [DOI] [PubMed] [Google Scholar]