

Abstract
The authors prospectively investigated the association between dairy intake and risk of Parkinson’s disease among 57,689 men and 73,175 women from the Cancer Prevention Study II Nutrition Cohort from the American Cancer Society. A total of 250 men and 138 women with Parkinson’s disease were identified during the follow-up (1992–2001). Dairy consumption was positively associated with the risk of Parkinson’s disease: compared with the lowest intake quintile, the corresponding relative risks (RRs) for quintiles 2–5 were 1.4, 1.4, 1.4, and 1.6 (95 percent confidence interval (CI): 1.1–2.2; p for trend=0.05). A higher risk among dairy consumers was found in both men and women, although the association in women appeared non-linear. The meta-analysis of all prospective studies confirmed a moderately elevated risk of Parkinson’s disease among individuals with high dairy consumption: the RRs between extreme intake categories were 1.6 (95 percent CI: 1.3–2.0) for men and women combined, 1.8 for men (95 percent CI: 1.4–2.4), and 1.3 for women (95 percent CI: 0.8–2.1). These data suggest that dairy consumption may increase the risk of Parkinson’s disease, particularly in men. More studies are needed to further examine these findings and to explore the underlying mechanisms.
Keywords: dairy, diet, milk, Parkinson’s disease
Diet may play an important role in the etiology of Parkinson’s disease, either by altering the oxidative balance in the brain or by serving as a vehicle for environmental neurotoxins. Few epidemiological studies have been able to examine potential associations between diet and Parkinson’s disease because of its relatively low incidence and insidious onset. Most of the published investigations were case-control studies (1–4) that may not be well-suited for investigating associations between diet and neurodegenerative diseases, due to the potential for recall and selection bias (5, 6). With prospective data from the Health Professionals Follow-up Study and the Nurses’ Health Study, we initially reported an unexpected positive association between dairy consumption and risk of Parkinson’s disease in men, but not in women (5). A recent analysis of the prospective Honolulu Asian Aging Study, a cohort comprising only men, reported that higher mid-life consumption of milk, but not of other dairy items, was related to a greater risk of Parkinson’s disease in later life (7). Here, by taking advantage of the well-established American Cancer Society’s Cancer Prevention Study II-Nutrition cohort, we were able to further prospectively investigate the associations between dairy, individual dairy items, and nutrients from dairy products and risk of Parkinson’s disease and to examine the potential gender difference.
MATERIALS AND METHODS
Study population
Participants in this study were drawn from the Cancer Prevention Study II-Nutrition cohort, a prospective study of 86,404 men and 97,786 women that was initiated in 1992 by the American Cancer Society to investigate risk factors for cancer incidence (8). This Nutrition cohort is a subgroup of the 1.2 million US men and women originally recruited in 1982 in the Cancer Prevention Study II for research on cancer mortality. Participants were 50–74 years of age at enrollment in 1992 or 1993, when they completed a mailed questionnaire that included questions on demographic, medical, environmental, lifestyle and dietary habits. Follow-up surveys were conducted in 1997, 1999 and 2001 to update exposure information and to ascertain whether major chronic diseases have occurred. A specific question on the lifetime occurrence of Parkinson’s disease was asked in the 2001 survey. The current analyses were limited to participants in the 2001 survey who did not have Parkinson’s disease before they answered the baseline 1992 questionnaire. We also excluded men and women who reported extreme values of daily energy intake (<550 or >3500 kcal/day for women and <650 or >4000 kcal/day for men) and those who left 10 or more items blank or did not complete the beverage section of the questionnaire. The follow-up of eligible participants (n= 130,864) started on the date of return of the 1992 questionnaire and ended on the date when the first symptoms of Parkinson’s disease were noticed for Parkinson’s disease cases, or August 31, 2001 for participants without Parkinson’s disease. The study was approved by the Human Subject Committee at Harvard School of Public Health and the Institutional Review Board at Emory University.
Case ascertainment
The case ascertainment procedures were similar to those in our previous studies of Parkinson’s disease (9). Briefly, we wrote to all participants who reported a diagnosis of Parkinson’s disease on the 2001 questionnaire and asked for their permission to contact their treating neurologists. We then asked their treating neurologists (or internists if the neurologists did not respond) to complete a diagnostic questionnaire or to send a copy of the medical record. The questionnaire asked physicians to report the presence or absence of cardinal signs of Parkinson’s disease (rest tremor, rigidity, bradykinesia, and postural instability), response to levodopa treatment, and other clinical features that may corroborate a Parkinson’s disease diagnosis or suggest an alternative diagnosis. A case was confirmed if the diagnosis was considered clinically definite or probable by the treating neurologist or internist, or if the medical record included either a final diagnosis of Parkinson’s disease made by a neurologist, or evidence at a neurological examination of at least two of the four cardinal signs with one being rest tremor or bradykinesia, a progressive course, and the absence of unresponsiveness to levodopa or other features suggesting an alternative diagnosis. The review of medical records was conducted by our movement disorder specialist (MAS), blind to the exposure status.
A total of 840 participants reported a Parkinson diagnosis at any time in the past and 677 (81%) provided informed consents for contacting their treating neurologists. A completed diagnostic questionnaire or medical record was obtained from 648 (96%) patients and 588 (91%) diagnoses were thus confirmed. After further excluding 175 cases with onset before 1992 and 25 with missing information on dietary intake, we finally included 388 confirmed incident PD cases in the analysis. With the exception of age and education level, these 388 cases were not significantly different from those that were not included in the analyses. Overall, 67.6 percent of the cases in the cohort were confirmed by the treating neurologists (55.0 percent) or movement disorder specialists (12.6 percent), 21.1 percent by review of the medical records, and 11.4 percent by the treating internists or family physicians.
Dietary Assessment
Diet was assessed at baseline using a 68-item semi-quantitative food frequency questionnaire that was modified from the brief “Health Habits and History Questionnaire” developed by Block et al (10). This questionnaire asked about portion size (small, medium, and large) and frequency of consumption of individual food items with 9 possible categories, ranging from “never or less than once/month” to “2+ times/day” for foods and to “6+ times/day” for beverages. Dietary intakes of nutrients were calculated using the Diet Analysis System Version 3.8a. The questionnaire also asked for the frequency and doses of common vitamin supplement uses during the past year, including multiple vitamins and calcium. Individual vitamin D supplement use was rare and thus was not included in the questionnaire. Total intake of calcium was calculated from intakes of foods, multivitamins, and calcium supplements, while that of vitamin D from foods and multivitamins.
Individual dairy items listed on the questionnaire included whole milk, low fat milk, skim milk, cheese, low fat yogurt, regular yogurt, and ice cream. In addition, we estimated additional cheese intake from pizza, assuming 16 percent of the weight of pizza. Intakes of grams of individual dairy items were summed up as the total intake of dairy products. The food frequency questionnaire used in the current study was validated among a subgroup of 441 participants against four random 24-hour dietary recalls collected over a 1-year period (11). After controlling for day-to-day variation in 24 hour recalls, the energy-adjusted correlations between foods/nutrients assessed by these two methods were 0.72/0.63 (men/women) for dairy products, 0.57/0.66 for calcium, 0.58/0.66 for fat, and 0.29/0.33 for protein (11). Intakes of dairy products and associated nutrients assessed in this cohort has been linked to risk of colorectal (12) and prostate cancers (13) in directions that were consistent with their biological hypotheses.
Statistical analyses
Intakes of calcium and vitamin D were adjusted for energy intake, using the residual method (14). Protein and fat intakes were expressed as percent of energy. Nutrient intakes were further classified according to their sources: dairy products, other foods, or supplements. For most foods and nutrients, we categorized intakes into quintiles according to the intake distribution of the overall cohort. For yogurts and ice cream, individuals who never ate those foods were grouped as the lowest intake category and the rest were categorized into quartiles. We categorized supplement intakes according to their distributions, calcium into 4 categories (mg/day: 0, 1–130, 131–620, and >620) and vitamin D into 3 categories (IU/day: 0, 1–399, ≥400). In each analysis, the lowest intake category was used as the reference group.
Relative risks (RR) and 95 percent confidence intervals (CI) were calculated from the Cox proportional hazards models, adjusting for baseline age, sex, smoking status (never, past, current (cigarette/day: 1–14, 15–24, and 25+)) and energy intake (quintiles), vigorous physical activity (quintiles), education level (below high school, high school, post-high school education, college graduate, and graduate school) and pesticide exposure (yes/no) that was reported in the 1982 Cancer Prevention Study II survey. The statistical significance of a linear trend was tested by including the median of each category as a continuous variable in the Cox models. Stratified analyses were further conducted according to sex, baseline age (<65 years and ≥65 years), and smoking status (never smokers and ever smokers). To reduce the potential bias attributable to dietary changes caused by early and unrecognized symptoms of Parkinson’s disease, we performed lag analyses by excluding the first 2 years of follow-up.
Finally, we conducted a meta-analysis by pooling the results of all three prospective cohort studies (Health Professionals and Nurses cohorts, Honolulu cohort, and the current Cohort). Statistical testing showed no heterogeneity among the risk estimates from different cohorts. Both overall and gender specific summary RRs comparing the highest versus the lowest dairy consumption categories were calculated with a fixed-effects model by averaging the natural logarithms of the RRs from individual studies, weighted by the inverses of their variances. The meta-analysis was performed using STATA software version 7.0 (STATA Corp, College Station, Texas). All other analyses were conducted with the SAS software version 8.2 (SAS Institute, Cary, North Carolina).
RESULTS
Age adjusted baseline population characteristics according to dairy consumption quintiles are provided in Table 1. Compared with individuals of low dairy consumption, those with higher intakes had proportionally more men and fewer smokers. They were also more likely to report higher education, higher energy intakes, more vigorous physical activities and ibuprofen use at baseline and pesticide exposure in 1982.
Table 1.
Population characteristics by dairy consumption at baseline*
| Diary intake quintiles | |||||
|---|---|---|---|---|---|
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | |
| Means (range, g/day) | 78.1 | 178.6 | 285.5 | 415.3 | 815.0 |
| (0–133.6) | (133.6–228.5) | (228.5–345.9) | (345.9–502.0) | (502.1–3488.6) | |
| Age (years) | 62.1 | 62.6 | 62.5 | 62.8 | 62.9 |
| Men (%) | 41.0 | 43.6 | 44.8 | 45.8 | 45.0 |
| Past smokers (%) | 47.3 | 46.9 | 47.2 | 45.9 | 43.8 |
| Current smokers (%) | 10.0 | 7.4 | 7.1 | 6.7 | 6.6 |
| High school or post-high school (%) | 57.6 | 55.3 | 53.6 | 52.3 | 51.1 |
| College or higher (%) | 36.3 | 39.5 | 41.3 | 43.1 | 44.3 |
| Pesticide exposure in 1982 (%) | 4.9 | 5.0 | 5.2 | 5.4 | 6.6 |
| Energy intake (kcal/day) | 1297 | 1421 | 1516 | 1642 | 1909 |
| Vigorous physical activity (MET/week)† | 3.9 | 4.3 | 4.6 | 4.9 | 5.0 |
| Ibuprofen users (%) | 18.2 | 19.1 | 19.5 | 19.7 | 20.0 |
Except for age, all other covariates were standardized to the age distribution of the entire cohort.
Metabolic equivalent tasks (MET) were calculated by multiplying the hours spent per week on each activity by its typical energy expenditure requirements
During 1,107,406 person years of follow-up, we identified 250 incident Parkinson’s disease cases in men and 138 in women. Among men and women combined, total consumption of dairy products was positively associated with Parkinson’s disease risk (Table 2). A linear trend was evident in men, whereas in women, the risk increased between the first and second quintiles but the linear trend was not statistically significant. Of the four individual dairy items, only milk intake was significantly associated with a higher risk of Parkinson’s disease (Table 2). Similar findings were observed in analyses excluding the first 2 years of follow-up (71 cases were excluded): the RR comparing the highest versus the lowest intake categories was 1.5 (95 percent CI: 1.0–2.3, p for trend=0.07) for total dairy and 1.7 (95 percent CI: 1.2–2.5, p for trend=0.03) for milk. No significant differences across subgroups were found in analyses stratified by baseline age and smoking status. For overall dairy products, the RR between extreme quintiles were 1.6 (95 percent CI: 0.9–2.7) for participants younger than age 65 and 1.5 (95 percent CI: 0.9–2.5) for those older, and were 1.6 for never smokers (95 percent CI: 0.9–2.6) and 1.4 (95 percent CI: 0.9–2.4) for ever smokers; the corresponding RRs for milk consumption were 2.0 (95 percent CI: 1.2–3.3) for younger participants, 1.5 (95 percent CI: 0.9–2.4) for older participants, 1.6 (95 percent CI: 1.0–2.7) for never smokers, and 1.7 (95 percent CI: 1.0–2.8) for ever smokers.
Table 2.
Relative risks (RR)* and 95 percent confidence intervals (CI) of Parkinson’s disease according to baseline consumption of dairy products (1992–2001)
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | P trend | |
|---|---|---|---|---|---|---|
| Total dairy (g/day) | 0–133.6 | 133.6–228.5 | 228.5–345.9 | 345.9–502.0 | >502.0 | |
| All | ||||||
| Cases / person years | 53 / 218,219 | 79 / 221,412 | 79 / 222,398 | 83 / 223,874 | 94 / 221,502 | |
| RR† (95% CI) | 1.0 | 1.4 (1.0, 2.0) | 1.4 (1.0, 1.9) | 1.4 (1.0, 2.0) | 1.6 (1.1, 2.2) | 0.05 |
| Men | ||||||
| Cases / person years | 33 / 89,490 | 46 / 97,155 | 49 / 100,279 | 58 / 103,805 | 64 / 100,972 | |
| RR† (95% CI) | 1.0 | 1.2 (0.8, 1.9) | 1.3 (0.8, 2.0) | 1.4 (0.9, 2.2) | 1.6 (1.0, 2.5) | 0.04 |
| Women | ||||||
| Cases / person years | 20 / 128,730 | 33 / 124,257 | 30 / 122,119 | 25 / 120,069 | 30 / 120,531 | |
| RR† (95% CI) | 1.0 | 1.6 (0.9, 2.9) | 1.5 (0.9, 2.7) | 1.3 (0.7, 2.3) | 1.5 (0.8, 2.8) | 0.5 |
| Milk (g/day)** | 0–84.3 | 84.4–155.4 | 155.4–273.1 | 273.1–397.1 | >397.1 | |
| All | ||||||
| Cases / person years | 49 / 220,625 | 78 / 221,516 | 87 / 221,931 | 76 / 223,149 | 98 / 220,184 | |
| RR† (95% CI) | 1.0 | 1.4 (1.0, 2.1) | 1.6 (1.1, 2.3) | 1.4 (0.9, 1.9) | 1.7 (1.2, 2.4) | 0.03 |
| Men | ||||||
| Cases / person years | 31 / 92,680 | 50 / 94,678 | 54 / 98,612 | 45 / 103,635 | 70 / 102,095 | |
| RR† (95% CI) | 1.0 | 1.4 (0.9, 2.2) | 1.5 (1.0, 2.4) | 1.2 (0.7, 1.9) | 1.8 (1.2, 2.9) | 0.02 |
| Women | ||||||
| Cases / person years | 18 / 127,945 | 28 / 126,838 | 33 / 123,318 | 31 / 119,514 | 28 / 118,090 | |
| RR† (95% CI) | 1.0 | 1.4 (0.8, 2.6) | 1.8 (1.0, 3.1) | 1.7 (0.9, 3.0) | 1.5 (0.8, 2.8) | 0.5 |
| Cheese (g/day)** | 0–1.7 | 1.7–4.9 | 4.9–9.4 | 9.7–19.6 | >19.6 | |
| All | ||||||
| Cases / person years | 68 / 216,829 | 65 / 223,837 | 84 / 213,424 | 83 / 233,543 | 88 / 219,773 | |
| RR† (95% CI) | 1.0 | 0.9 (0.7, 1.3) | 1.3 (0.9, 1.8) | 1.1 (0.8, 1.6) | 1.3 (0.9, 1.8) | 0.1 |
| Men | ||||||
| Cases / person years | 38 / 88,678 | 35 / 87,742 | 65 / 93,008 | 52 / 109,826 | 60 / 112,446 | |
| RR† (95% CI) | 1.0 | 0.9 (0.6, 1.4) | 1.6 (1.1, 2.4) | 1.1 (0.7, 1.7) | 1.2 (0.8, 1.9) | 0.5 |
| Women | ||||||
| Cases / person years | 30 / 128,150 | 30 / 136,094 | 19 / 120,417 | 31 / 123,717 | 28 / 107,327 | |
| RR† (95% CI) | 1.0 | 1.0 (0.6, 1.6) | 0.7 (0.4, 1.3) | 1.3 (0.7, 2.1) | 1.3 (0.8, 2.3) | 0.1 |
| Yogurt (g/day)** | 0 | 4.0–14.7 | 14.7–35.4 | 35.4–92.9 | >92.9 | |
| All | ||||||
| Cases / person years | 171 / 476,919 | 76 / 160,036 | 44 / 153,863 | 55 / 155,688 | 42 / 160,900 | |
| RR† (95% CI) | 1.0 | 1.3 (1.0, 1.8) | 0.9 (0.7, 1.3) | 1.1 (0.8, 1.4) | 0.9 (0.6, 1.3) | 0.4 |
| Men | ||||||
| Cases / person years | 127 / 261,438 | 41 / 63,325 | 27 / 55,505 | 33 / 62,106 | 22 / 49,325 | |
| RR† (95% CI) | 1.0 | 1.2 (0.8, 1.7) | 1.0 (0.7, 1.5) | 1.1 (0.7, 1.5) | 0.9 (0.6, 1.4) | 0.7 |
| Women | ||||||
| Cases / person years | 44 / 215,481 | 35 / 96,711 | 17 / 98,358 | 22 / 93,581 | 20 / 111,575 | |
| RR† (95% CI) | 1.0 | 1.7 (1.1, 2.6) | 0.9 (0.5, 1.6) | 1.1 (0.7, 1.8) | 1.0 (0.6, 1.6) | 0.5 |
| Ice cream (g/day)** | 0 | 1.4–6.4 | 6.7–12.9 | 15–30.9 | >35 | |
| All | ||||||
| Cases / person years | 90 / 328,560 | 67 / 198,273 | 71 / 196,897 | 95 / 213,427 | 65 / 170,248 | |
| RR† (95% CI) | 1.0 | 1.2 (0.9, 1.7) | 1.3 (0.9, 1.7) | 1.4 (1.0, 1.8) | 1.1 (0.8, 1.5) | 0.9 |
| Men | ||||||
| Cases / person years | 43 / 120,008 | 35 / 69,626 | 43 / 70,086 | 74 / 125,648 | 55 / 106,333 | |
| RR† (95% CI) | 1.0 | 1.4 (0.9, 2.2) | 1.7 (1.1, 2.5) | 1.6 (1.1, 2.3) | 1.4 (0.9, 2.1) | 0.5 |
| Women | ||||||
| Cases / person years | 47 / 208,552 | 32 / 128,647 | 28 / 126,811 | 21 / 87,779 | 10 / 63,916 | |
| RR† (95% CI) | 1.0 | 1.1 (0.7, 1.7) | 0.9 (0.5, 1.4) | 1.1 (0.7, 1.9) | 0.7 (0.3, 1.4) | 0.4 |
adjusted for baseline age, sex, smoking, energy intake, and ibuprofen use, vigorous physical activity, education level, and pesticide use reported in 1982.
Approximate serving sizes include 240 g/cup for milk and yogurt, 52 g for 2 oz cheese, 78 g for ½ cup ice cream
In nutrient analyses, total intakes of calcium and protein (from all sources) were associated with a higher risk of Parkinson’s disease (Table 3), but these associations were stronger for calcium and protein from dairy than from non dairy sources. In contrast, intake of calcium supplements was not associated with Parkinson’s disease risk: compared with individuals who did not take supplemental calcium, the multivariate RRs were 0.7 for users of 1–130 mg/day, 1.0 for 131–620 mg/day, and 1.2 (95 percent CI: 0.9,1.7, p for trend=0.2) for more than 620 mg /day. Further, supplemental intake of vitamin D was associated with a lower risk of Parkinson’s disease, the corresponding RRs for individuals with intake 1-399 IU/day and ≥400 IU/day compared with nonusers were 0.7 and 0.8 (95 percent CI: 0.6, 1.0; p for trend=0.03) respectively. Further analyses with the same nutrients from different sources simultaneously adjusted in the same analytic model confirmed that only nutrients from dairy products, except for dairy fat, tended to be positively associated with Parkinson’s disease risk (data not shown). Energy intake was not related to PD risk in this study population (data not shown).
Table 3.
Relative risks (RR)* and 95 percent confidence intervals (CI) of Parkinson’s disease according to baseline intakes of nutrients from dairy products or other sources (1992–2001)
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | P trend | |
|---|---|---|---|---|---|---|
| Calcium (mg) | ||||||
| Total intake | 82.1 – 558.0 | 558.0 – 727.7 | 727.7 – 921.4 | 921.4 – 1252.2 | >1252.2 | |
| No. of cases | 50 | 76 | 88 | 79 | 95 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.3 (0.9, 1.9) | 1.4 (1.0, 2.0) | 1.3 (0.9, 1.8) | 1.6 (1.1, 2.3) | 0.02 |
| From dairy products | 0 – 258.3 | 258.3 – 394.1 | 394.1 – 539.6 | 539.6 – 756.9 | >756.9 | |
| No. of cases | 54 | 74 | 81 | 89 | 90 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.3 (0.9, 1.8) | 1.3 (0.9, 1.9) | 1.4 (1.0, 2.0) | 1.3 (0.9, 1.9) | 0.2 |
| From other sources | 37.2 – 203.5 | 203.5 – 252.4 | 252.4 – 316.3 | 316.3 – 465.1 | >465.1 | |
| No. of cases | 64 | 78 | 101 | 68 | 77 | |
| RR† (95%CI) | 1.0 (Ref.) | 0.9 (0.7, 1.3) | 1.1 (0.8, 1.5) | 0.7 (0.5, 1.0) | 1.1 (0.8, 1.5) | 0.6 |
| Vitamin D (IU) | ||||||
| Total intake | 0 – 110.3 | 110.3 – 172.8 | 172.8 – 287.4 | 287.4 – 527.7 | >527.7 | |
| No. of cases | 55 | 93 | 88 | 79 | 73 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.5 (1.0, 2.0) | 1.3 (0.9, 1.9) | 1.3 (0.9, 1.8) | 1.1 (0.8, 1.6) | 0.6 |
| From dairy products | 0 – 39.2 | 39.2 – 71.3 | 71.3 – 112.7 | 112.7 – 175.0 | >175.0 | |
| No. of cases | 40 | 87 | 81 | 89 | 91 | |
| RR† (95%CI) | 1.0 (Ref.) | 2.0 (1.4, 2.9) | 1.8 (1.2, 2.7) | 1.9 (1.3, 2.8) | 1.8 (1.3, 2.7) | 0.06 |
| From other sources | 0 – 41.2 | 41.2 – 61.2 | 61.2 – 92.8 | 92.8 – 419.8 | >419.8 | |
| No. of cases | 76 | 68 | 106 | 68 | 70 | |
| RR† (95%CI) | 1.0 (Ref.) | 0.8 (0.6, 1.1) | 1.1 (0.8, 1.4) | 0.8 (0.6, 1.1) | 0.8 (0.6, 1.1) | 0.08 |
| Protein (% of energy) | ||||||
| Total intake | 3.3 – 13.7 | 13.7 – 15.4 | 15.4 – 16.9 | 16.9 – 18.9 | >18.9 | |
| No. of cases | 63 | 80 | 77 | 75 | 93 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.2 (0.9, 1.7) | 1.2 (0.8, 1.6) | 1.2 (0.8, 1.6) | 1.6 (1.1, 2.2) | 0.01 |
| From dairy products | 0 – 2.1 | 2.1 – 3.2 | 3.2 – 4.3 | 4.3 – 6.0 | >6.0 | |
| No. of cases | 71 | 70 | 92 | 62 | 93 | |
| RR† (95%CI) | 1.0 (Ref.) | 0.9 (0.7, 1.3) | 1.3 (0.9, 1.7) | 0.9 (0.6, 1.2) | 1.3 (1.0, 1.8) | 0.09 |
| From other sources | 1.0 – 9.8 | 9.8 – 11.2 | 11.2 – 12.6 | 12.6 – 14.3 | >14.3 | |
| No. of cases | 70 | 82 | 84 | 71 | 81 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.1 (0.8, 1.6) | 1.2 (0.8, 1.6) | 1.0 (0.7, 1.4) | 1.2 (0.9, 1.7) | 0.5 |
| Fat (% of energy) | ||||||
| Total intake | 4.2 – 26.6 | 26.6 – 32.5 | 32.5 – 37.3 | 37.3 – 42.4 | >42.4 | |
| No. of cases | 77 | 88 | 95 | 66 | 62 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.1 (0.8, 1.5) | 1.2 (0.9, 1.6) | 0.8 (0.6, 1.2) | 0.8 (0.6, 1.2) | 0.1 |
| From dairy products | 0 – 2.0 | 2.0 – 3.5 | 3.5 – 5.4 | 5.4 – 8.6 | >8.6 | |
| No. of cases | 77 | 70 | 86 | 82 | 73 | |
| RR† (95%CI) | 1.0 (Ref.) | 0.9 (0.6, 1.2) | 1.1 (0.8, 1.5) | 1.1 (0.8, 1.5) | 1.0 (0.7, 1.3) | 0.9 |
| From other sources | 0.3 – 21.9 | 21.9 – 26.7 | 26.7 – 30.9 | 30.9 – 35.8 | >35.8 | |
| No. of cases | 75 | 89 | 98 | 74 | 52 | |
| RR† (95%CI) | 1.0 (Ref.) | 1.1 (0.8, 1.6) | 1.2 (0.9, 1.7) | 0.9 (0.7, 1.3) | 0.7 (0.5, 1.0) | 0.04 |
adjusted for baseline age, sex, smoking, energy intake, and ibuprofen use, vigorous physical activity, education level, and pesticide use reported in 1982.
To date, three prospective studies have evaluated dairy or milk consumption in relation to Parkinson’s disease. These studies varied in sample sizes, population composition, length of follow-up, and methods in dietary assessment and case identification. Despite these differences, a meta-analysis of these studies clearly demonstrated that higher dairy/milk consumption was associated with a moderately increased risk of Parkinson’s disease, particularly in men. The combined RRs between extreme intake categories were 1.6 (95 percent CI: 1.3–2.0, p=0.000) for men and women combined, 1.8 (95 percent CI: 1.4–2.4, p=0.000) for men, and 1.3 (95 percent CI: 0.8–2.1, p=0.3) for women (Figure).
Figure.
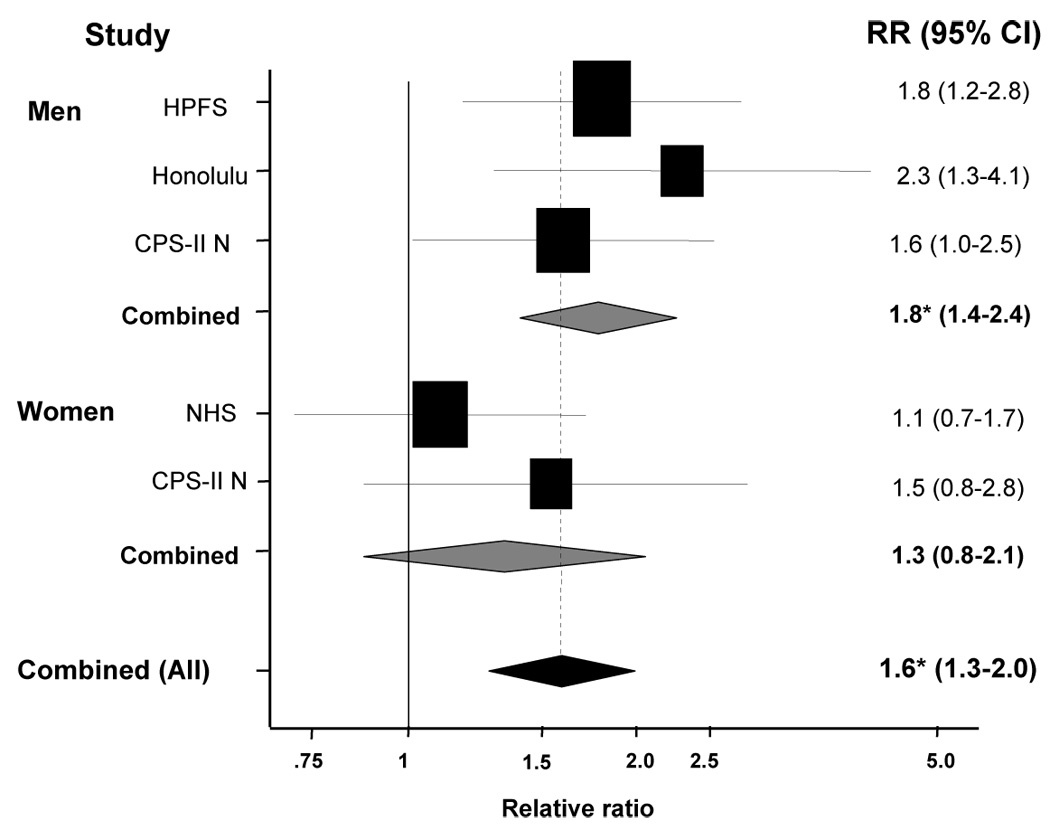
A meta-analysis of all prospective studies on dairy / milk consumption and risk of Parkinson’s disease in men and women, comparing the highest intake category with the lowest. Relative risk (RR) and 95 percent confidence interval (CI) are provided. Squares indicate individual RR in each study. The size of the square is proportional to the percent weight of individual study in the meta-analysis; horizontal line represents the 95 percent CI. The pooled RR and 95 percent CI are indicated by the shaded diamond.
HPFS: Health Professionals Follow-up Study (men only)
NHS: Nurses’ Health Study (women only)
CPS-II N: Cancer Prevention Study II Nutrition Cohort
HAAS: Honolulu Asian Aging Study (men only)
* p=0.000
DISCUSSION
In this large observational study, we found that higher dairy consumption was associated with increased risk of Parkinson’s disease. The association was stronger in men and was mostly explained by milk consumption. Because this investigation was based on a prospective cohort with a long follow-up period and validated dietary assessment, recall and selection biases are unlikely the explanation of our findings. Reverse causality or confounding by known Parkinson’s disease risk factors such as age and smoking are also not very likely, because the association remained after excluding the first two years of follow-up or adjusting for relevant covariates. However, potential confounding by unmeasured factors such as a lack of novelty-seeking personality (15) could not be excluded. Another potential limitation of the current study is that we were unable to physically examine individual Parkinson’s disease patients and had to rely on the diagnoses made by treating neurologists for case confirmation. Although a few misdiagnoses are likely, recent clinico-pathological studies revealed that 90 percent of neurologist diagnosed Parkinson’s disease patients could be confirmed at autopsy (16). Further, any diagnostic error would have probably attenuated the association between dairy and Parkinson’s disease, because case identification was most likely independent of the dietary assessment.
The findings of the present study are consistent with those from two previous prospective investigations: in the first study (5), men in the highest dairy consumption category had 80 percent higher risk than men in the lowest; in women, the results showed a slightly inverse “U” shape association with higher risk among women with moderate dairy consumptions. In the second study (7), a study of Japanese American men in Honolulu, Hawaii, Park et al. reported that men with more than 16 ounces of milk consumption had 130 percent higher risk of Parkinson’s disease than those who did not drink milk.
In all studies, the results could not be attributed to measured dairy nutrients such as calcium. A pooled analysis of the current study with the previous ones confirmed a moderate positive association between dairy consumption and risk of Parkinson’s disease, particularly in men. In both the current and previous investigations, the relationship was less clear in women than in men. Among women in the Nurses Health Study, the RRs for dairy intake quartiles were 1.0 (referent), 1.3, 1.3, and 1.1 with a p value for linear trend of 0.9. In the current study, on the other hand, Parkinson’s disease risk among women increased approximately 60 percent at the second dairy consumption quintile and tended to remain at that level for higher consumption categories. However, both analyses were based on a relatively small number of cases; a prospective study with more female cases is needed to better evaluate this relationship in women.
So far, the epidemiological evidence suggests that the dairy and Parkinson’s disease association is unlikely due to calcium, vitamin D, or fat. All three studies generally found that calcium and vitamin D were positively associated with Parkinson’s disease risk only when they were from dairy foods, and fat from either dairy foods or other sources were not related to increased risk of Parkinson’s disease. Further, neither calcium nor vitamin D from supplements was significantly related to increased risk of Parkinson’s disease.
The observation of similar findings in all three well-established prospective studies on dairy and Parkinson’s disease risk suggests that the association is unlikely to be fortuitous. One possibility is that dairy products are contaminated with neurotoxic chemicals. Substantial epidemiological and experimental evidence suggest that pesticides may increase Parkinson’s disease risk (17) and postmortem studies found higher levels of organochlorines, polychlorinated biphenyls, and dieldrin in the brains of Parkinson’s disease patients than in control brains (18, 19); some of these compounds present at low levels in dairy products. Further, chemicals such as tetrahydroisoquinolines (20) and precursors of β-carbolines that induce parkinsonism in rodents and primates (21, 22) are present in a variety of dairy foods (23, 24). However, the overall contribution of dairy consumption to exposures to pesticides and other neurotoxins is probably only modest. Another potential explanation for the positive association between dairy and Parkinson’s disease may involve the potential effects of dairy products on circulating levels of uric acid. Higher dairy consumption has been related to lower circulating levels of uric acid and also lower risk of gout (25–27). Uric acid has been hypothesized to be neuroprotective by preventing oxidative damage caused by reactive nitrogen and oxygen species, and higher plasma levels of uric acid have been prospectively linked to a lower risk of incident Parkinson’s disease in two cohorts (28, 29). Because of the lack of experimental data, any potential explanation is speculative.
In summary, accumulating evidence from this and previous prospective studies supports a positive association between dairy consumption and risk of Parkinson’s disease, particularly in men. Future epidemiological and experimental investigations are needed to further evaluate this association and to ascertain the underlying mechanisms.
Acknowledgements
This study was supported by a fast track research grant from the Michael J. Fox Foundation for Parkinson Research, a gift from the Kinetics Foundation, a K-08 grant from NIH (NS48468), and (in part) the Intramural Research Program of the NIH, National Institute of Environmental Health Sciences. The authors thank Dr. Yiqing Song for his technical help.
Approved Abbreviations
- CI
confidence interval
- RR
relative risk
Footnotes
Disclosure: The authors have reported no conflicts of interest.
References
- 1.Hellenbrand W, Boeing H, Robra BP, et al. Diet and Parkinson's disease. II: A possible role for the past intake of specific nutrients. Results from a self-administered food-frequency questionnaire in a case-control study. Neurology. 1996;47:644–650. doi: 10.1212/wnl.47.3.644. [DOI] [PubMed] [Google Scholar]
- 2.Anderson C, Checkoway H, Franklin GM, et al. Dietary Factors in Parkinson's Disease: The role of Food Groups and Specific Foods. Movement Disorders. 1999;14:21–27. doi: 10.1002/1531-8257(199901)14:1<21::aid-mds1006>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 3.Johnson CC, Gorell JM, Rybicki BA, et al. Adult nutrient intake as a risk factor for Parkinson's disease. Int J Epidemiol. 1999;28:1102–1109. doi: 10.1093/ije/28.6.1102. [DOI] [PubMed] [Google Scholar]
- 4.Scheider WL, Hershey LA, Vena JE, et al. Dietary antioxidants and other dietary factors in the etiology of Parkinson's disease. Mov Disord. 1997;12:190–196. doi: 10.1002/mds.870120209. [DOI] [PubMed] [Google Scholar]
- 5.Chen H, Zhang SM, Hernan MA, et al. Diet and Parkinson's disease: A potential role of dairy products in men. Ann Neurol. 2002;52:793–801. doi: 10.1002/ana.10381. [DOI] [PubMed] [Google Scholar]
- 6.Chen H, Zhang SM, Hernan MA, et al. Dietary intakes of fat and risk of Parkinson's disease. Am J Epidemiol. 2003;157:1007–1014. doi: 10.1093/aje/kwg073. [DOI] [PubMed] [Google Scholar]
- 7.Park M, Ross GW, Petrovitch H, et al. Consumption of milk and calcium in midlife and the future risk of Parkinson disease. Neurology. 2005;64:1047–1051. doi: 10.1212/01.WNL.0000154532.98495.BF. [DOI] [PubMed] [Google Scholar]
- 8.Calle EE, Rodriguez C, Jacobs EJ, et al. The American Cancer Society Cancer Prevention Study II Nutrition Cohort: rationale, study design, and baseline characteristics. Cancer. 2002;94:2490–2501. doi: 10.1002/cncr.101970. [DOI] [PubMed] [Google Scholar]
- 9.Ascherio A, Zhang SM, Hernán MA, et al. Prospective study of caffeine consumption and risk of Parkinson's disease in men and women. Ann Neurol. 2001;50:56–63. doi: 10.1002/ana.1052. [DOI] [PubMed] [Google Scholar]
- 10.Block G, Hartman AM, Naughton D. A reduced dietary questionnaire: development and validation. Epidemiology. 1990;1:58–64. doi: 10.1097/00001648-199001000-00013. [DOI] [PubMed] [Google Scholar]
- 11.Flagg EW, Coates RJ, Calle EE, et al. Validation of the American Cancer Society Cancer Prevention Study II Nutrition Survey Cohort Food Frequency Questionnaire. Epidemiology. 2000;11:462–468. doi: 10.1097/00001648-200007000-00017. [DOI] [PubMed] [Google Scholar]
- 12.Jacobs EJ, Connell CJ, Chao A, et al. Multivitamin use and colorectal cancer incidence in a US cohort: does timing matter? Am J Epidemiol. 2003;158:621–628. doi: 10.1093/aje/kwg190. [DOI] [PubMed] [Google Scholar]
- 13.Rodriguez C, McCullough ML, Mondul AM, et al. Calcium, dairy products, and risk of prostate cancer in a prospective cohort of United States men. Cancer Epidemiol Biomarkers Prev. 2003;12:597–603. [PubMed] [Google Scholar]
- 14.Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. 1997;65:1220S–1228S. doi: 10.1093/ajcn/65.4.1220S. discussion 9S–31S. [DOI] [PubMed] [Google Scholar]
- 15.Menza M. The personality associated with Parkinson's disease. Curr Psychiatry Rep. 2000;2:421–426. doi: 10.1007/s11920-000-0027-1. [DOI] [PubMed] [Google Scholar]
- 16.Hughes AJ, Daniel SE, Kilford L, et al. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55:181–184. doi: 10.1136/jnnp.55.3.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Priyadarshi A, Khuder SA, Schaub EA, et al. A meta-analysis of Parkinson's disease and exposure to pesticides. Neurotoxicology. 2000;21:435–440. [PubMed] [Google Scholar]
- 18.Fleming L, Mann JB, Bean J, et al. Parkinson's disease and brain levels of organochlorine pesticides. Annals of Neurology. 1994;36:100–103. doi: 10.1002/ana.410360119. [DOI] [PubMed] [Google Scholar]
- 19.Corrigan FM, Murray L, Wyatt CL, et al. Diorthosubstituted polychlorinated biphenyls in caudate nucleus in Parkinson's disease. Exp Neurol. 1998;150:339–342. doi: 10.1006/exnr.1998.6776. [DOI] [PubMed] [Google Scholar]
- 20.Nagatsu T. Isoquinoline neurotoxins in the brain and Parkinson's disease. Neurosci Res. 1997;29:99–111. doi: 10.1016/s0168-0102(97)00083-7. [DOI] [PubMed] [Google Scholar]
- 21.Kotake Y, Yoshida M, Ogawa M, et al. Chronic administration of 1-benzyl-1,2,3,4-tetrahydroisoquinoline, an endogenous amine in the brain, induces parkinsonism in a primate. Neurosci Lett. 1996;217:69–71. doi: 10.1016/0304-3940(96)13065-2. [DOI] [PubMed] [Google Scholar]
- 22.Kotake Y, Tasaki Y, Makino Y, et al. 1-Benzyl-1,2,3,4-tetrahydroisoquinoline as a parkinsonism-inducing agent: a novel endogenous amine in mouse brain and parkinsonian CSF. J Neurochem. 1995;65:2633–2638. doi: 10.1046/j.1471-4159.1995.65062633.x. [DOI] [PubMed] [Google Scholar]
- 23.Makino Y, Ohta S, Tachikawa O, et al. Presence of tetrahydroisoquinoline and 1-methyl-tetrahydro-isoquinoline in foods: compounds related to Parkinson's disease. 1988;43:373–378. doi: 10.1016/0024-3205(88)90115-4. [DOI] [PubMed] [Google Scholar]
- 24.Niwa T, Yoshizumi H, Tatematsu A, et al. Presence of tetrahydroisoquinoline, a parkinsonism-related compound, in foods. J Chromatogr. 1989;493:347–352. doi: 10.1016/s0378-4347(00)82740-1. [DOI] [PubMed] [Google Scholar]
- 25.Choi HK, Atkinson K, Karlson EW, et al. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N Engl J Med. 2004;350:1093–1103. doi: 10.1056/NEJMoa035700. [DOI] [PubMed] [Google Scholar]
- 26.Choi HK, Curhan G. Gout: epidemiology and lifestyle choices. Curr Opin Rheumatol. 2005;17:341–345. [PubMed] [Google Scholar]
- 27.Choi HK. Dietary risk factors for rheumatic diseases. Curr Opin Rheumatol. 2005;17:141–146. doi: 10.1097/01.cco.0000152664.87204.3c. [DOI] [PubMed] [Google Scholar]
- 28.Davis JW, Grandinetti A, Waslien CI, et al. Observations on serum uric acid levels and the risk of idiopathic Parkinson's disease. Am J Epidemiol. 1996;144:480–484. doi: 10.1093/oxfordjournals.aje.a008954. [DOI] [PubMed] [Google Scholar]
- 29.de Lau LM, Koudstaal PJ, Hofman A, et al. Serum uric acid levels and the risk of Parkinson disease. Ann Neurol. 2005;58:797–800. doi: 10.1002/ana.20663. [DOI] [PubMed] [Google Scholar]