

Lemierre syndrome (LS) is a life-threatening condition characterized by antecedent oropharyngeal infection, disseminated foci of infection or septic emboli, and bacteremia demonstrated by blood cultures positive for Fusobacterium.1 Lemierre syndrome classically affects young, healthy men. At the onset of disease, a patient often visits a primary care provider with only a fever and recent sore throat.1,2 The condition, however, is highly curable if appropriate antibiotic therapy is administered promptly.1,2 Family physicians should, therefore, maintain a high index of suspicion for LS to ensure that this potentially fatal disease is detected as early as possible.
Case description
A 24-year-old previously healthy man presented with a 1-month history of intermittent fevers, weight loss of about 2 kg (5 lb), and generalized myalgia. The patient also reported occasional chills and sweats, but denied contacts with visibly unwell people, recent travel, or risk factors for HIV and hepatitis. He had no history of serious medical problems and was not currently taking any medications. On further questioning, he recalled experiencing a mild viral prodrome of sore throat, neck pain, and rhinorrhea a few weeks before, but review of systems was otherwise unremarkable. He was ultimately diagnosed with the flu, advised about adequate fluid intake and rest, and discharged home with a follow-up appointment the next week.
The patient returned a day later complaining of similar, albeit worsening, symptoms. On repeat assessment, he looked unwell and was perspiring. Additional physical findings included a temperature of 38.6°C, a pulse of 114 beats/min, and a respiratory rate of 32 breaths/min. The oropharynx was reddened, and the cervical chain lymph nodes were tender. The remainder of the head and neck, cardiopulmonary, and abdominal examinations were unremarkable. The patient was referred to the nearest emergency department to expedite further workup.
Routine investigations showed that the white blood cell count was elevated at 16.4 x 109/L, of which 86% were neutrophils. The patient also had laboratory evidence of anemia (hemoglobin 108 g/L, mean corpuscular volume 82 fL) and thrombocytosis (platelets 510 x 109/L). Liver enzymes were mildly increased: alanine aminotransferase 38, aspartate aminotransferase 33, alkaline phosphatase 128, and γ-glutamyl-transferase 109 U/L. Electrolytes and renal function tests were within normal limits, but albumin was decreased at 26 g/L. Electrocardiogram and chest x-ray film appeared normal. Echocardiogram result was negative for endocarditis, but subsequent computed tomographic scans demonstrated a 4.5-cm abscess in the right lobe of the liver (Figure 1) as well as small areas of septic emboli in the lower lobes of both lungs. Abdominal ultrasound showed hepatic vein thrombosis. Blood cultures were drawn and revealed gram-negative anaerobic bacilli.
Figure 1.
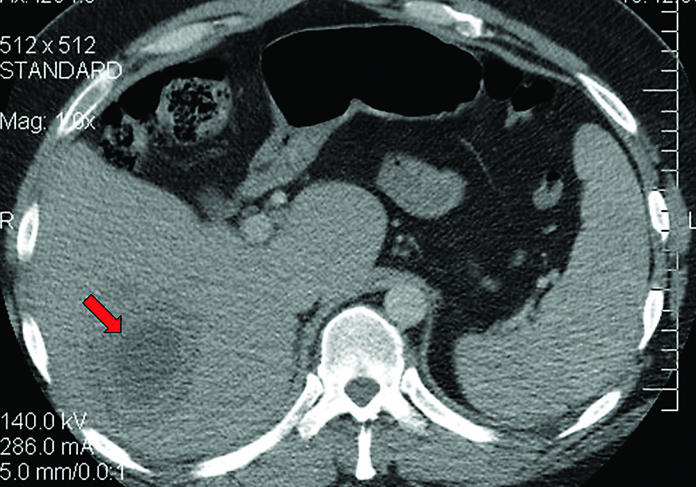
Tomographic scan showing a 4.5-cm abscess in the right lobe of the liver
The patient was admitted to hospital for parenteral antimicrobial therapy (metronidazole 500 mg intravenously every 6 hours) for his bacteremia and anticoagulation for his thrombosis. Nearly 4 weeks after hospital admission, the bacteria in the blood were identified as Fusobacterium nucleatum. The patient’s treatment was gradually changed to metronidazole 500 mg orally 4 times daily to complete a 6-week course of antibiotics. His symptoms resolved completely with repeat blood cultures confirming clearance of his bacteremia.
Discussion
A MEDLINE search was performed using the key words Lemierre syndrome, Fusobacterium, oropharyngeal infection, and pharyngitis. Articles on LS and its history, epidemiology, clinical features, and diagnosis and management were reviewed in detail.
The genus Fusobacterium is a group of obligate anaerobic gram-negative bacilli responsible for causing LS—an entity first described by Courmont and Cade in 1900, which subsequently acquired its eponym following a published review of 20 affected patients by Dr Andre Lemierre.3
Lemierre syndrome is typically characterized by 1) oropharyngeal infection, 2) Fusobacterium septicemia, 3) findings of metastatic infection, and, occasionally, 4) clinical or radiologic evidence of thrombosis or suppurative thrombophlebitis of the internal jugular vein (IJV).1 The last component of the tetrad is not an absolute requirement for diagnosis.1 The syndrome classically affects young adults between the ages of 16 and 25 years.2 There is a male predominance of about 75%, and affected individuals are usually immunocompetent without serious comorbidity.2
In the pre-antibiotic era, LS was a frequent complication of oropharyngitis and was invariably associated with a poor prognosis (90% to 100% mortality).3 The advent and widespread use of β-lactam antibiotics have reduced the incidence to 0.8 to 1.5 cases per million persons per year, leading some to refer to LS as the forgotten disease because its diagnosis is now seldom considered at initial presentation.4 Nevertheless, it remains a potentially life-threatening condition, with an estimated mortality rate of about 15% despite antibiotic therapy.5
The syndrome manifests as pharyngotonsillitis at the outset, but can infrequently present as sinusitis or mastoiditis.6 Several weeks after the onset of sore throat, neck pain, and lethargy, the patient develops fevers, rigour, and septicemia complicated by thromboembolic metastases.6 The lungs are the most common site of emboli, but the spleen, joints, and bones can also be affected.7 Involvement of the liver (eg, abscess, thrombosis) as seen in our patient is rare, but has been reported.8,9
Fusobacterium is ubiquitous in the normal flora of the oropharyngeal, gastrointestinal, and genitourinary tracts of healthy humans. A preceding pharyngitis, however, weakens the host mucosal barrier to allow this commensal organism to reach the bloodstream, potentially leading to dental abscess formation, endocarditis, or other systemic infections.6 In LS, Fusobacterium necrophorum is the organism most commonly isolated from the blood, apparently present in up to 90% of cases.1–3 Fusobacterium nucleatum is rare, but is reportedly associated with liver involvement.8
Diagnosis of LS is primarily based on the identification of Fusobacterium in one or more blood cultures. However, because the organism is fastidious and can take several weeks to grow, early detection of the disease and prompt initiation of treatment rely heavily on an astute clinical suspicion. In practice, the diagnosis of LS should be suspected in any young adult who presents with ongoing fever after a recent episode of pharyngitis. Imaging studies to search for multiple septic emboli can sometimes help to elucidate the diagnosis while awaiting culture results. In particular, a computed tomographic scan of the neck should be performed to determine whether thrombosis or suppurative thrombophlebitis of the IJV is present.10 It is not uncommon, however, for some patients to exhibit only neck pain or tender cervical nodes as their sole manifestation of IJV thrombophlebitis.
While penicillins remain the treatment of choice in most cases of LS, cephalosporins (such as cefoxitin and cefotetan), metronidazole, or clindamycin monotherapy can sometimes be used as first-line drugs owing to the rare emergence of penicillin-resistant strains with β-lactamase activity.11 Penicillin G at a dose of 24 million units daily by continuous infusion is a reasonable treatment. Therapy is generally administered parenterally for up to 2 weeks, and then orally for a total duration of 6 weeks. Surgical drainage of abscesses is usually indicated for patients who fail to respond adequately to antibiotics alone.11 The use of anticoagulation in LS is common, but remains controversial.12
Conclusion
This report underscores the fact that LS is a rare but grave condition, and that early recognition is paramount to ensure optimal outcomes. Although lungs are the most common site of emboli, this case indicates that other organs, such as the liver, are not immune to such phenomena. To this end, family physicians must maintain a high level of clinical suspicion for any young adult who presents with unexplained, persistent fever after a recent oropharyngeal infection so that prompt diagnosis and therapy can be offered.
EDITOR’S KEY POINTS
Lemierre syndrome is a rare condition typically characterized by oropharyngeal infection, Fusobacterium septicemia, findings of metastatic infection, and occasionally clinical or radiologic evidence of thrombosis or suppurative thrombophlebitis of the internal jugular vein (which is not an absolute requirement for diagnosis).
Penicillins remain the treatment of choice in most cases of Lemierre syndrome, but cephalosporins, metronidazole, or clindamycin monotherapy can sometimes be used.
POINTS DE REPèRE Du RéDaCTEuR
Le syndrome de Lemierre est une affection rare qui se caractérise habituellement par une infection oropharyngée, une septicémie au Fusobacterium, des signes d’infection métastasique et, occasionnellement, une manifestation clinique ou radiologique de thrombose ou de thrombophlébite suppurative de la veine jugulaire interne (ce qui n’est pas une exigence absolue pour poser le diagnostic).
La pénicilline demeure l’antibiothérapie de première intention dans la plupart des cas de syndrome de Lemierre, mais on peut parfois utiliser une monothérapie à la céphalosporine, au métronidazole ou à la clindamycine.
Footnotes
This article has been peer reviewed.
Competing interests
None declared
References
- 1.Hagelskjaer LH, Prag J, Malczynski J, Kristensen JH. Incidence and clinical epidemiology of necrobacillosis, including Lemierre’s syndrome, in Denmark 1990–1995. Eur J Clin Microbiol Infect Dis. 1998;17(8):561–5. doi: 10.1007/BF01708619. [DOI] [PubMed] [Google Scholar]
- 2.Chirinos JA, Lichtstein DM, Garcia J, Tamariz LJ. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine (Baltimore) 2002;81(6):458–65. doi: 10.1097/00005792-200211000-00006. [DOI] [PubMed] [Google Scholar]
- 3.Lemierre A. On certain septicemias due to anaerobic organisms. Lancet. 1936;1:701–3. [Google Scholar]
- 4.Weesner CL, Cisek JE. Lemierre’s syndrome: the forgotten disease. Ann Emerg Med. 1993;22(2):256–8. doi: 10.1016/s0196-0644(05)80216-1. [DOI] [PubMed] [Google Scholar]
- 5.Stallworth JR, Carroll JM. Lemierre’s syndrome: new insights into an old disease. Clin Pediatr. 1997;36(12):715–7. doi: 10.1177/000992289703601209. [DOI] [PubMed] [Google Scholar]
- 6.Dool H, Soetekouw R, van Zanten M, Grooters E. Lemierre’s syndrome: three cases and a review. Eur Arch Otorhinolaryngol. 2005;262(8):651–4. doi: 10.1007/s00405-004-0880-3. Epub 2004 Dec 15. [DOI] [PubMed] [Google Scholar]
- 7.Sinave CP, Hardy GJ, Fardy PW. The Lemierre syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oro-pharyngeal infection. Medicine (Baltimore) 1989;68(2):85–94. [PubMed] [Google Scholar]
- 8.Le Roux K, Seve P, Gomard E, Boibieux A, Beziat C, Stankovic K, et al. [Lemierre syndrome variant: hepatic abscesses and hepatic vein thrombosis due to Fusobacterium nucleatum septicemia.] Rev Med Interne. 2006;27(6):482–6. doi: 10.1016/j.revmed.2005.12.013. Epub 2006 Jan 18. [DOI] [PubMed] [Google Scholar]
- 9.Bentham JR, Pollard AJ, Milford CA, Anslow P, Pike MG. Cerebral infarct and meningitis secondary to Lemierre’s syndrome. Pediatr Neurol. 2004;30(4):281–3. doi: 10.1016/j.pediatrneurol.2003.10.013. [DOI] [PubMed] [Google Scholar]
- 10.Nguyen-Dinh KV, Marsot-Dupuch K, Portier F, Lamblin B, Lasjaunias P. Lemierre syndrome: usefulness of CT in detection of extensive occult thrombophlebitis. J Neuroradiol. 2002;29(2):132–5. [PubMed] [Google Scholar]
- 11.Hagelskjaer LH, Kristensen L, Prag J. Human necrobacillosis, with emphasis on Lemierre syndrome. Clin Infect Dis. 2000;31(2):524–32. doi: 10.1086/313970. [DOI] [PubMed] [Google Scholar]
- 12.Williams A, Nagy M, Wingate J, Bailey L, Wax M. Lemierre’s syndrome: a complication of acute pharyngitis. Int J Pediatr Otorhinlaryngol. 1998;45(1):51–7. doi: 10.1016/s0165-5876(98)00092-5. [DOI] [PubMed] [Google Scholar]