

Abstract
Ceramic systems have limited long-term fracture resistance, especially when they are used in posterior areas or for fixed partial dentures. The objective of this study was to determine the site of crack initiation and the causes of fracture of clinically failed ceramic fixed partial dentures. Six Empress 2® lithia-disilicate (Li2O·2SiO2)-based veneered bridges and 7 experimental lithia-disilicate-based non-veneered ceramic bridges were retrieved and analyzed. Fractography and fracture mechanics methods were used to estimate the stresses at failure in 6 bridges (50%) whose fracture initiated from the occlusal surface of the connectors. Fracture of 1 non-veneered bridge (8%) initiated within the gingival surface of the connector. Three veneered bridges fractured within the veneer layers. Failure stresses of the all-core fixed partial dentures ranged from 107 to 161 MPa. Failure stresses of the veneered fixed partial dentures ranged from 19 to 68 MPa. We conclude that fracture initiation sites are controlled primarily by contact damage.
Keywords: fractography, dental ceramics, indentation, lateral cracks, fracture mechanics
Introduction
Increasing interest in ceramic fixed prostheses has followed improvements in strength, aesthetics, and ease of processing. Such advances include introduction of lithia disilicate (Li2O·2SiO2) reinforced glass ceramics for dental use. The increased strength and improved esthetics of these systems are well-documented in the dental literature (Höland et al., 2000). In addition, clinical fractures of a bilayer full-ceramic fixed partial denture system have been reported in a previous clinical study (Sorensen et al., 1999). However, the mechanisms for the failure of dental ceramics have not been studied extensively, although fractographic analysis is a key element in the design and development of dental structural materials (Kelly et al., 1989).
Fractographic analysis has been critical in efforts to analyze failure mechanisms, to identify fracture initiation sites, and to determine the probable cause of failure from fractographic analysis of retrieved clinical specimens. One can determine whether the failure is caused by a processing defect, by contact damage, or by an overload. Quantitative fractography is the application of fracture mechanics to characteristic features on the fracture surface, including the size of the fracture-initiating flaw. The overall objective of this study was to identify, by fractographic techniques, the principal crack initiation site and the cause of failure of fractured ceramic fixed partial dentures.
Materials & Methods
Veneered and non-veneered (all-core) lithia-disilicate-based glass-ceramic fixed partial dentures were analyzed in this study. Veneered glass-ceramic fixed partial dentures were made from the Empress 2® all-ceramic system (Ivoclar Vivadent AG, Schaan, Liechtenstein). X-ray diffraction analysis showed that the veneering ceramic consisted primarily of amorphous glass. Core fixed partial dentures were made with an experimental lithia-disilicate glass-ceramic that has a crystal volume fraction greater than that of the Empress 2® core ceramic. Clinically failed fixed partial dentures were retrieved from a clinical study.
To determine the fracture toughness of the monolithic core and veneer ceramics and the apparent fracture toughness of core-veneer bilayer ceramics, we prepared four-point bending specimens from Empress 2 veneer, Empress 2 core ceramic, lithia-disilicate-based experimental core ceramic, and bilayer Empress 2 core-veneer ceramic. The expected increase in strength in the bilayer composite is associated with the compressive residual stresses in the veneer (Taskonak et al., 2004), because of the difference between thermal expansion co-efficients of veneer and those of core ceramics. In addition, the glass veneer is a visco-elastic material and contributes to compressive residual stress development. Thus, the toughness calculated is termed ‘apparent toughness’. The final dimensions of beam specimens were 1.6 mm (height) × 4 mm (width) × 25 mm (length). The veneer thickness was 0.6 mm for each bilayer specimen. The core/veneer thickness ratio was 10/6. The span length/specimen thickness ratio was 15/1.6, so that large deflections and high shear stresses within the beam specimens could be avoided. In total, 10 specimens were used for each group for fracture toughness calculations. Thus, 30 beam specimens were used in the study. Specimens were indented on the veneer surface with a Vickers indenter (M-400, Leco, Tokyo, Japan) at a load of 9.7 N to produce controlled cracks. Specimens were stored in air for 24 hrs to ensure complete crack growth. They were then loaded to fracture at a crosshead speed of 0.5 mm/min by means of a four-point bending fixture in an Instron Universal testing machine. Flexure experiments were performed with a fixture having an 18-mm outer span and a 6-mm inner span. The veneer layer was placed in tension for bilayer flexure test specimens. The strength (σf) of the laminated composites was calculated according to composite beam theory (Beer and Johnston, 1981).
Fracture toughness of the beam specimens was measured by quantitative fractography. Fracture in brittle materials generally occurs by the unstable propagation of a defect as a result of the combination of high stress and a large flaw (Mecholsky, 2001).
Almost all mechanically induced cracks can be idealized as semi-elliptical, sharp cracks of depth, a, and half-width, 2b. The crack sizes are approximated by an equivalent semicircular crack size, c [c = (ab)1/2]. Fracture toughness, KC, is calculated based on the stress at fracture, or strength, σf, and the crack size, c:
| (1) |
where KC is the critical stress intensity factor (fracture toughness), and Y is a geometric factor, which accounts for the shape of the fracture-initiation crack and loading condition. The quantity Y depends on the ratio a/b. The equation [c = (ab)1/2] allows many irregular crack shapes to be analyzed, and avoids the complications of calculating a geometric factor for each crack (Mecholsky, 1991). For surface cracks that are small relative to the thickness of the sample, Y ∼ 1.24. For sharp cracks that are induced by a Vickers or Knoop indentation, Y ∼ 1.65, and for internal cracks, Y ∼ 1.4 (Mecholsky, 1991).
Cracks induced by a microhardness indenter are associated with local residual stress around the indentation impression. The residual stress must be accounted for in the fracture toughness equation. A geometrical factor of Y ∼ 1.65 compensates for local residual stresses (Marshall et al., 1980; Mecholsky, 1991).
We determined the fracture origins by examining the fracture surface and tracing the characteristic markings back to the initiation site (Mecholsky, 1995). These markings included twist hackle (river marks), wake hackle (fracture tails), cleavage steps, Wallner lines, and branching locations.
When characterizing fracture origins, we made scanning electron microscope images (JSM-6400, Jeol, Tokyo, Japan) of the overall sample and of an enlargement of the fracture origin region. The general fractographic procedure is outlined in ASTM standard C1322 (ASTM, 1999). We measured crack-initiating flaws to determine the fracture toughness of each specimen.
Residual stress caused in bilayer specimens by the thermal expansion coefficient mismatch of the veneer ceramic and core ceramic was estimated by (Lawn, 1993):
| (2) |
where σR is the global residual stress within the veneer layer, Δα is the difference between thermal expansion co-efficients of the veneer and core ceramics, and ΔT is the difference between the glass transition temperature of the veneer and room temperature. Subscripts C and V refer to core and veneer, respectively. The terms v and E are Poisson's ratio and Young's modulus, respectively. Since the glass phase of the bilayer composite is visco-elastic, global compressive residual stress was produced by a visco-elastic relaxation mechanism of the glass phase (Scherer, 1986). The term ‘global residual stress’ represents overall residual stresses within a specimen.
Results
We concluded, from preliminary examination of the fracture surfaces, that 7 (88%) of the 8 connector failures and 2 (66%) of the 3 veneer ceramic failures were acceptable for fracture surface analysis (Fig. 1). Primary fracture origins of the 3 discarded samples were missing as a result of a chipping near the origin. All fracture surfaces exhibited multiple crack initiation sites as a result of multidirectional and repeated loading. Arrest lines in the form of ridges were present on the fracture surfaces (Fig. 2a). In addition, some curved markings resulted from the intersection of two crack fronts (Fig. 2a). Twist hackle markings helped us determine the primary fracture origin in the core ceramic (Fig. 2b). Wake hackle markings from pores were selected as reference points for determination of the location of fracture origins in the glass veneer (Fig. 2b) (Mecholsky, 1995). The wake hackle markings were observed next to pores on the opposite side, away from the fracture origin in the veneer layer. Porosity existed within the glass veneer because of slurry preparation and the sintering of veneer powders.
Figure 1.
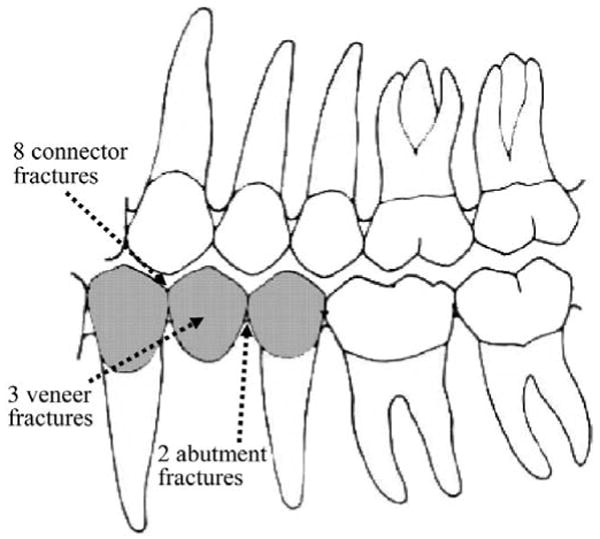
Schematic of a fixed partial denture with fracture initiation sites and numbers.
Figure 2.

Fracture origin can be identified by fracture markings. (a) All fracture surfaces exhibit multiple crack initiation sites as a result of multidirectional loading. Arrest lines in the form of ridges are present on the fracture surfaces. One of the arrest lines is a result of intersection of 2 fracture paths. Arrows represent the fracture propagation direction. (b) Wake hackle markings were used to establish the reference points for determining the fracture origin in the glass veneer. Wake hackle markings were also observed on porosities as an outcome of fracture passage through pores. The markings indicate the direction of the fracture origin in the veneer layer. Black arrows specify the direction of the fracture propagation. (c) Fracture toughness of the glass veneer was used to calculate the stress at failure of samples in which the fracture origin was within the veneer layer. Fracture propagates quickly without any increase in stress from the point where the semi-minor axis of the fracture origin ends. Arrows represent the interface between core and veneer layers, as well as fracture origin.
In 7 of the 8 (88%) connector failures examined, fracture initiated on the surfaces of the prostheses. Six (75%) of the 8 connector failures originated on the occlusal surface of the fixed partial dentures, and 1 initiated from the gingival surface. Fracture origins of the veneered samples occurred within the veneer layer (Table). Two fixed partial dentures failed in their posterior abutments, and 1 of them had an identifiable fracture origin in the margin area. The fracture initiation site of the latter was located on the outer side of the margin, and fracture occurred along the mesiodistal axis of the abutment. Two failures within the veneer layer failed from ‘chipping’, and both originated at internal flaws. The thickness of the veneer layers in clinically failed fixed partial dentures varied based on their location. On labial surfaces of fixed partial dentures, the veneer layer was thicker compared with those on the occlusal surface (Fig. 2c).
Table.
Failure Stress (σf), Critical Flaw Size (c), Semi-minor (a) and Semi-major (2b) Axes of the Specimens, and Residual Stress (σR)
| Sample ID | a (μm) | 2b (μm) | c (μm) | Failure Stress (MPa) | Crack Initiation Site | Material |
|---|---|---|---|---|---|---|
| 1 | 376 | 1129 | 460 | 116 | Connector (gingival surface) | Experimental core ceramic |
| 2 | 94 | 1223 | 240 | 161 | Posterior abutment margin | Experimental core ceramic |
| 3 | 361 | 918 | 407 | 124 | Connector (occlusal surface) | Experimental core ceramic |
| 4 | 282 | 941 | 364 | 131 | Connector (occlusal surface) | Experimental core ceramic |
| 5 | 188 | 706 | 258 | 156 | Connector (occlusal surface) | Experimental core ceramic |
| 6 | 283 | 1367 | 440 | 27+22 (σR) | Connector (occlusal surface) | Experimental core ceramic/glass veneer |
| 7 | 376 | 1543 | 539 | 107 | Connector (occlusal surface) | Experimental core ceramic |
| 8 | 229 | 829 | 308 | 32+22 (σR) | Connector (occlusal surface) | Experimental core ceramic/glass veneer |
| 9 | 791 | 2232 | 939 | 19+22 (σR) | Veneer chipping | Experimental core ceramic/glass veneer |
| 10 | 283 | 1367 | 440 | 68+22 (σR) | Veneer chipping | Experimental core ceramic/glass veneer |
Crack sizes (c in Eq. 1) of the indented glass veneer beam specimens ranged between 7 × 10-5 m and 15 × 10-5 m. The fracture toughness values of the lithium-disilicate-based glass-ceramic core and the glass veneer were determined from beam samples, by quantitative fractography (Eq. 1). The mean fracture toughness of the core ceramic was 3.1 ± 0.1 MPa·m1/2, and the mean fracture toughness of the glass veneer was 0.7 ± 0.1 MPa·m1/2. We used the fracture toughness value of the glass veneer to calculate the stress at failure (Eq. 1) for the specimens in which fracture initiation occurred within the veneer surface. Fractographic analysis can determine the stress that would occur from a crack or flaw of a particular size only if the toughness or apparent toughness is known. For the all-core fixed partial dentures, the failure stress can be estimated directly from the crack size, and known toughness from the core ceramic beam specimens. However, for the veneered fixed partial dentures, we showed previously that residual compressive stress within the veneer layer is generated because of the elastic thermal mismatch and visco-elastic relaxation (Taskonak et al., 2004). Therefore, the calculated stress should include an additional term that compensates for the compressive residual stress, which has to be overcome before tensile loading. This is the value listed in the Table as σR. The critical flaw sizes, estimated failure stresses, and fracture initiation sites for each ceramic fixed partial denture are listed in the Table. The critical flaw size, c, of the specimens for which an origin could be found ranged from 240 to 939 μm. Estimated failure stresses of the fixed partial dentures that had fracture initiation sites within the veneer layers ranged from 19 to 68 MPa. Failure stresses of all-core fixed partial dentures that fractured in the connector area ranged from 107 to 161 MPa.
Dilatometric analysis showed that there was a slight difference between the thermal expansion coefficients, (α), of the core and veneer in the range of temperatures from 25°C to 600°C. The a values were 10.0 × 10-6/K and 10.4 × 10-6/K for the core and glass veneer, respectively. The glass transition temperature (Tg) of the glass veneer is 540°C (813°K), and the difference between Tg and room temperature is 518°K. Poisson's ratio is 0.23 for the glass veneer (vV) and 0.24 for the core ceramics (vC). In addition, Young's modulus, EV, is 64 GPa for the glass veneer and 96 GPa for the core ceramic (EC). The estimated residual stress within the veneer layer of the bilayer prostheses, according to the above parameters and Eq. (2), was 22 MPa (compressive) as shown in the Table. This calculation assumes that veneer/core materials are identical in heat treatment and geometry.
Discussion
Fracture surface analyses of failed ceramic fixed partial dentures showed that failure origins occurred mostly at surface flaws, except for the cases of ‘chipping’ failures, where fracture occurred within the veneer layer of the prostheses. Previous investigations have reported that fracture initiated typically along the veneer/core interface of ceramic crowns (Kelly et al., 1989; Thompson et al., 1994). However, this was not the case in our study.
Since most of the connector failures were associated with fractures that initiated from occlusal surfaces, these crack-initiating flaws were most likely introduced as a result of repeated contact damage. Evidence that supports this conclusion is the observation that fractures were multidirectional (Fig. 2a). During the mastication process, the mandible makes lateral, centric, and protrusive movements that allow the opposing cusp tip in the maxilla to exert multidirectional forces on the prosthesis. As a result, fracture can occur in the most vulnerable part of the ceramic fixed partial dentures, i.e., the connector (Oh et al., 2002). Fracture markings in sample 3 (Table) indicated that there were 2 fracture origins on the occlusal surface of the fixed partial denture (Fig. 2a). To determine the primary fracture origin that caused the failure, we analyzed fracture markings that were farther away from both fracture origins. These markings indicated that the primary fracture origin was the one with the longest path (the one on the left of the fracture surface) (Fig. 2a). The ridge between the 2 fracture origins represents the intersection of 2 of the propagating cracks. In addition, mechanical damage resulting from the occlusal adjustment by the dentist or the dental technician can introduce flaws in the fixed partial dentures.
In 2 of the 3 chipping failures, fracture origins were visible. In the third case, fracture initiated from the internal part of the veneer layer and propagated in 2 directions.
Fracture toughness of the glass veneer was used to calculate the stress at failure of specimens in which the fracture origin occurred within the veneer layer (Fig. 2c). The fracture-initiating crack propagates immediately upon reaching the failure stress. Even though the core layer is tougher than the veneer, once crack propagation begins in the veneer, the crack does not arrest or deviate out of plane. Crack progression is not impeded by the core ceramic at the interface between the core and veneer. Thus, the toughness of the veneer is appropriate for calculating the stress from the crack size (Eq. 1). The bilayer materials also include a term for the compressive residual stress generated by the thermal expansion anisotropy (∼ 22 MPa) and visco-elastic process (Taskonak et al., 2005).
We calculated failure stresses in core/veneer specimens that were relatively low compared with those reported by Höland et al. (2000). We reported that the increase in the strength of bilayer, core/veneer ceramics occurred because of a global compressive residual stress (Taskonak et al., 2004) (Table). However, it is not only the global residual stress that plays a role in the failure mechanism of bilayer dental ceramics. Local residual tensile and compressive stresses adjacent to points of contact damage from previous loading, and tensile stresses from flexural and/or subsequent contact loading can also cause failure. The superimposition of these stresses can cause lateral cracks to develop and/or propagate to the surface (Lawn, 1993). Even if the stresses are not sufficient to propagate median cracks, they can still produce lateral cracks and cause spalling (chipping) of the glass veneer. We conclude that fracture initiation sites of these glass-ceramic fixed partial dentures occurred primarily on occlusal surfaces in the veneered units. Any new systems that are developed should focus on toughening the veneer ceramic rather than the core ceramic.
Acknowledgments
This investigation was supported by Research Grants DE-06672-20 and DE-13492-01 from the National Institute of Dental and Craniofacial Research, National Institutes of Health, Bethesda, MD 20892, USA. We appreciate the assistance of Mr. Robert Lee in fabricating the ceramic specimens. The ceramic materials used in this study were provided by Ivoclar Vivadent AG, Schaan, Liechtenstein.
References
- ASTM. 1999 Annual Book of ASTM Standards. Vol. 15.01. West Conshohocken, PA: American Society for Testing and Materials; 1999. Standard practice for fractography and characterization of fracture origins in advanced ceramics. ASTM Designation C1322-96a. [Google Scholar]
- Beer FP, Johnston ER. Mechanics of materials. 2nd rev. New York: McGraw-Hill; 1981. pp. 150–233. [Google Scholar]
- Höland W, Schweiger M, Frank M, Rheinberger V. A comparison of the microstructure and properties of the IPS Empress 2 and the IPS Empress glass-ceramics. J Biomed Mater Res. 2000;53:297–303. doi: 10.1002/1097-4636(2000)53:4<297::aid-jbm3>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- Kelly JR, Campbell SD, Bowen HK. Fracture-surface analysis of dental ceramics. J Prosthet Dent. 1989;62:536–541. doi: 10.1016/0022-3913(89)90075-9. [DOI] [PubMed] [Google Scholar]
- Lawn B. Fracture of brittle solids. 2nd. Cambridge: Cambridge University Press; 1993. pp. 194–306. [Google Scholar]
- Marshall DB, Lawn BR, Mecholsky JJ. Effect of residual contact stresses on mirror flaw-size relations. J Am Ceram Soc. 1980;63:358–360. [Google Scholar]
- Mecholsky JJ., Jr Quantitative fractography: an assessment. In: Alfred NY, Varner JR, Fréchette VD, Quinn GD, editors. Fractography of glasses and ceramics; Proceedings of the conference on the fractography of glasses and ceramics; August 3-6, 1986; Westerville, OH: American Ceramic Society; 1991. pp. 413–451. [Google Scholar]
- Mecholsky JJ., Jr Fractography: determining the sites of fracture initiation. Dent Mater. 1995;11:113–116. doi: 10.1016/0109-5641(95)80045-X. [DOI] [PubMed] [Google Scholar]
- Mecholsky JJ. Fractography of brittle materials. In: Buschow KH, Cahn RW, Flemings MC, Ilschner B, Kramer EJ, Mahajan S, et al., editors. Encyclopedia of materials: science and technology. St. Louis, MO: Elsevier Science Ltd.; 2001. pp. 3257–3265. [Google Scholar]
- Oh W, Götzen N, Anusavice KJ. Influence of connector design on fracture probability of ceramic fixed-partial dentures. J Dent Res. 2002;81:623–627. doi: 10.1177/154405910208100909. [DOI] [PubMed] [Google Scholar]
- Scherer GW. Relaxation in glass and composites. 1st. New York: Wiley- Interscience publication; 1986. pp. 75–174. [Google Scholar]
- Sorensen JA, Cruz M, Mito WT, Raffeiner O, Meredith HR, Foser HP. A clinical investigation on three-unit fixed partial dentures fabricated with a lithium disilicate glass-ceramic. Pract Periodontics Aesthet Dent. 1999;11:95–106. [PubMed] [Google Scholar]
- Taskonak B, Anusavice KJ, Mecholsky JJ., Jr Role of investment interaction layer on strength and toughness of ceramic laminates. Dent Mater. 2004;20:701–708. doi: 10.1016/j.dental.2003.08.006. [DOI] [PubMed] [Google Scholar]
- Taskonak B, Mecholsky JJ, Jr, Anusavice KJ. Residual stresses in bilayer dental ceramics. Biomaterials. 2005;26:3235–3241. doi: 10.1016/j.biomaterials.2004.08.025. [DOI] [PubMed] [Google Scholar]
- Thompson JY, Anusavice KJ, Naman A, Morris HF. Fracture surface characterization of clinically failed all-ceramic crowns. J Dent Res. 1994;73:1824–1832. doi: 10.1177/00220345940730120601. [DOI] [PubMed] [Google Scholar]