

Abstract
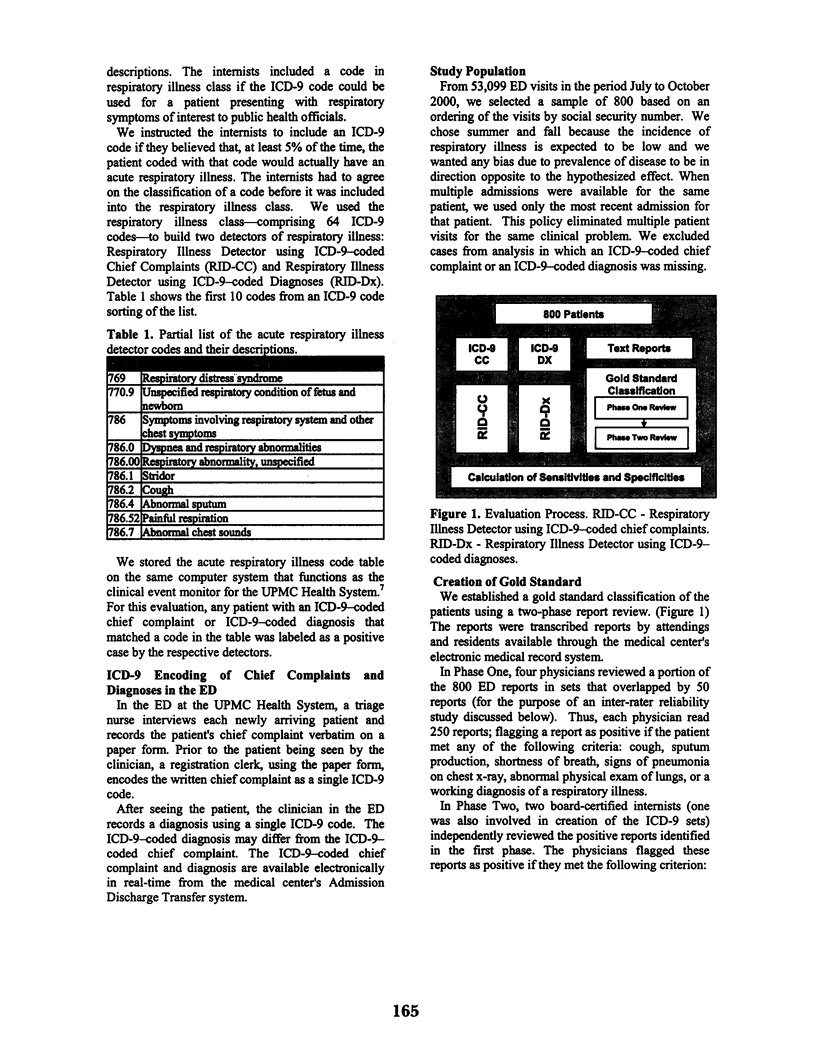
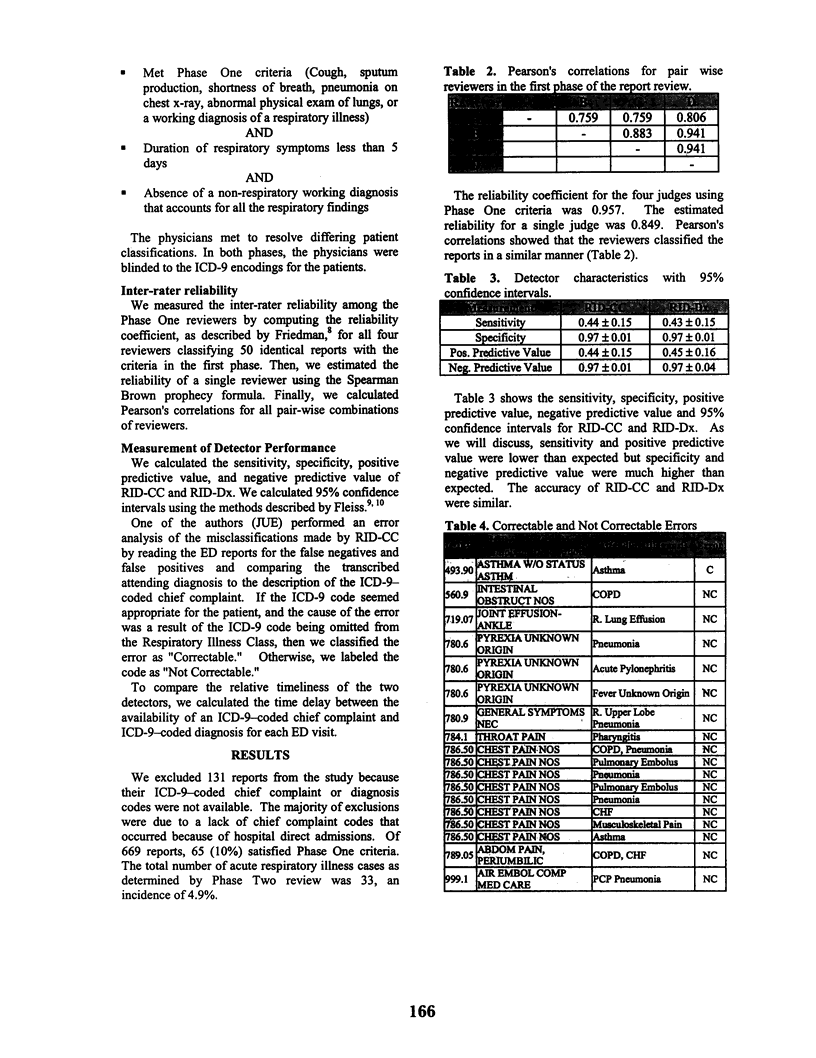
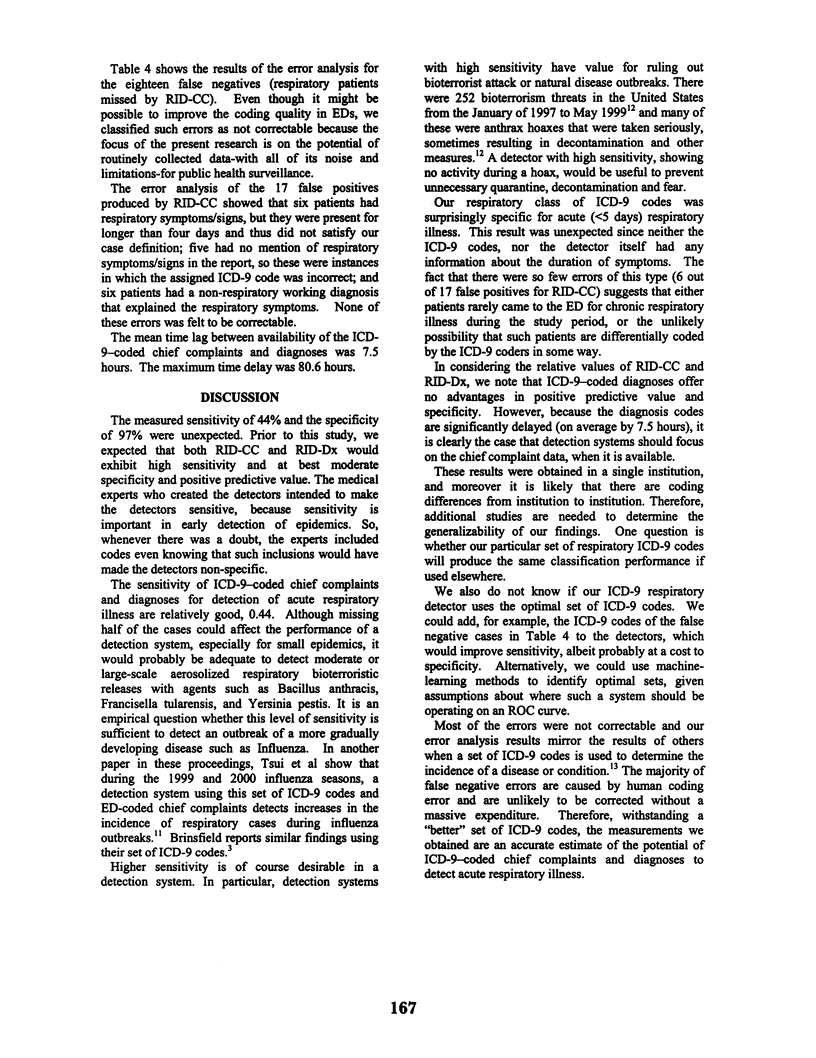
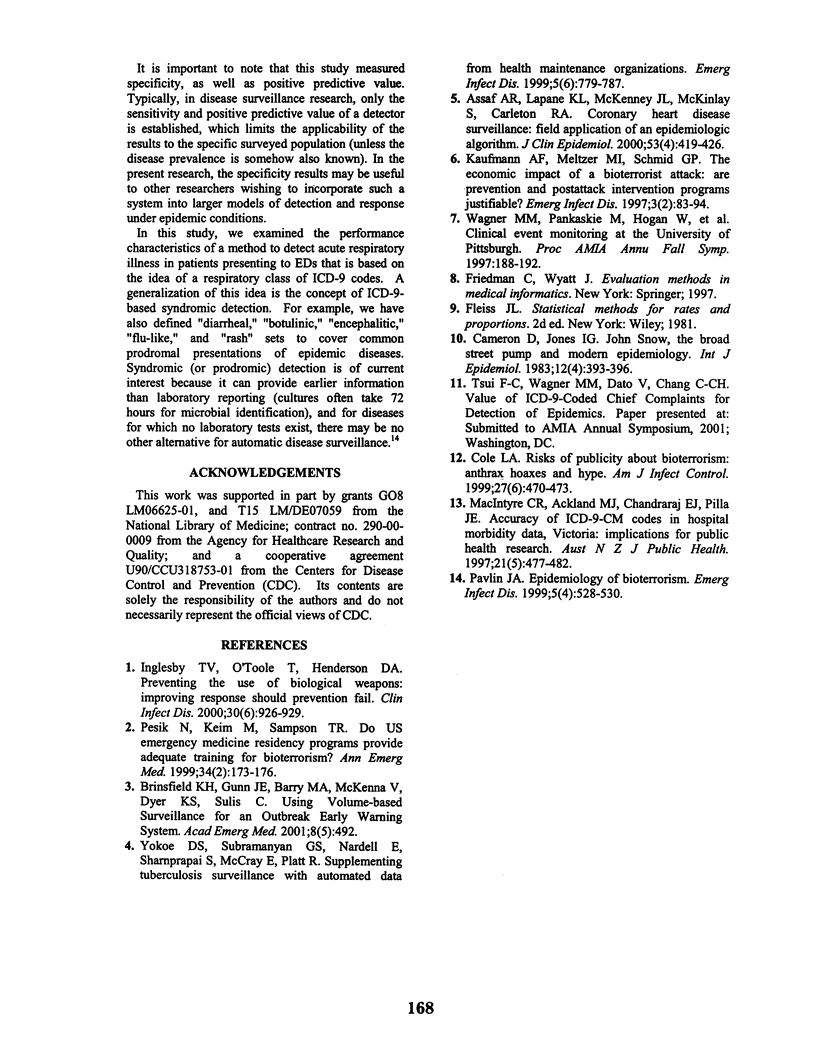
ICD-9-coded chief complaints and diagnoses are a routinely collected source of data with potential for use in public health surveillance. We constructed two detectors of acute respiratory illness: one based on ICD-9-coded chief complaints and one based on ICD-9-coded diagnoses. We measured the classification performance of these detectors against the human classification of cases based on review of emergency department reports. Using ICD-9-coded chief complaints, the sensitivity of detection of acute respiratory illness was 0.44 and its specificity was 0.97. The sensitivity and specificity using ICD-9-coded diagnoses were no different. These properties of excellent specificity and moderate sensitivity, coupled with the earliness and electronic availability of such data, support the use of detectors based on ICD-9 coding of emergency department chief complaints in public health surveillance.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Assaf A. R., Lapane K. L., McKenney J. L., McKinlay S., Carleton R. A. Coronary heart disease surveillance: field application of an epidemiologic algorithm. J Clin Epidemiol. 2000 Apr;53(4):419–426. doi: 10.1016/s0895-4356(99)00183-3. [DOI] [PubMed] [Google Scholar]
- Cameron D., Jones I. G. John Snow, the broad street pump and modern epidemiology. Int J Epidemiol. 1983 Dec;12(4):393–396. doi: 10.1093/ije/12.4.393. [DOI] [PubMed] [Google Scholar]
- Cole L. A. Risks of publicity about bioterrorism: anthrax hoaxes and hype. Am J Infect Control. 1999 Dec;27(6):470–473. doi: 10.1016/s0196-6553(99)70023-4. [DOI] [PubMed] [Google Scholar]
- Inglesby T. V., O'Toole T., Henderson D. A. Preventing the use of biological weapons: improving response should prevention fail. Clin Infect Dis. 2000 Jun 30;30(6):926–929. doi: 10.1086/313794. [DOI] [PubMed] [Google Scholar]
- Kaufmann A. F., Meltzer M. I., Schmid G. P. The economic impact of a bioterrorist attack: are prevention and postattack intervention programs justifiable? Emerg Infect Dis. 1997 Apr-Jun;3(2):83–94. doi: 10.3201/eid0302.970201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacIntyre C. R., Ackland M. J., Chandraraj E. J., Pilla J. E. Accuracy of ICD-9-CM codes in hospital morbidity data, Victoria: implications for public health research. Aust N Z J Public Health. 1997 Aug;21(5):477–482. doi: 10.1111/j.1467-842x.1997.tb01738.x. [DOI] [PubMed] [Google Scholar]
- Pavlin J. A. Epidemiology of bioterrorism. Emerg Infect Dis. 1999 Jul-Aug;5(4):528–530. doi: 10.3201/eid0504.990412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pesik N., Keim M., Sampson T. R. Do US emergency medicine residency programs provide adequate training for bioterrorism? Ann Emerg Med. 1999 Aug;34(2):173–176. doi: 10.1016/s0196-0644(99)70226-x. [DOI] [PubMed] [Google Scholar]
- Wagner M. M., Pankaskie M., Hogan W., Tsui F. C., Eisenstadt S. A., Rodriguez E., Vries J. K. Clinical event monitoring at the University of Pittsburgh. Proc AMIA Annu Fall Symp. 1997:188–192. [PMC free article] [PubMed] [Google Scholar]
- Yokoe D. S., Subramanyan G. S., Nardell E., Sharnprapai S., McCray E., Platt R. Supplementing tuberculosis surveillance with automated data from health maintenance organizations. Emerg Infect Dis. 1999 Nov-Dec;5(6):779–787. doi: 10.3201/eid0506.9906. [DOI] [PMC free article] [PubMed] [Google Scholar]