

Abstract
Syncope is a common problem in the older patient. Sometimes syncope is caused by extreme bradycardia secondary to atrioventricular (AV) block. We describe a case in which a 90-year-old woman presented with complete AV block due to severe hypothyroidism. After suppletion with levothyroxine, AV conduction was restored. (Neth Heart J 2008;16:57-9.)
Keywords: hypothyroidism, atrioventricular block
Syncope and fatigue are common problems in the elderly population. A possible cause of syncope may be extreme bradycardia. A pronounced reduction in the heart rate can be secondary to atrioventricular (AV) block. Symptomatic AV block requires treatment, and the choice of treatment depends on the cause of the block. Atrioventricular block may be due to fibrosis and sclerosis of the conduction system, ischaemic heart disease, increased vagal tone, or drugs. Drugs that can reduce AV conduction and that result in AV block include digitalis, calcium antagonists, β- antagonists and amiodarone.1 We report an unusual cause of AV block in an elderly patient due to severe hypothyroidism.
Case report
A 90-year-old woman presented to our emergency department with long-standing fatigue and dizziness. In the months prior to presentation the patient had been feeling progressively dizzy and tired. On the day of presentation she collapsed and was unresponsive for a short while. She had not suffered from any episodes of syncope before. Her medical history revealed Bechterew’s disease. The patient was not taking any medications.
On physical examination, the patient was conscious; her blood pressure was 150/100 mmHg and her heart rate was approximately 15 beats/min. She had a puffy face and examination of the neck revealed no struma. The jugular venous pressure was normal. Cardiac auscultation revealed normal heart sounds and a soft (II/VI) diastolic murmur at the fourth intercostal space. Upon auscultation the lungs were clear. Mild pretibial oedema was found bilaterally.
The electrocardiogram (ECG) (figure 1) showed a total atrioventricular block with an escape rhythm of 15 beats/min deriving from the posterior fascicle. There was a right bundle branch block and a left axis deviation.
Figure 1.
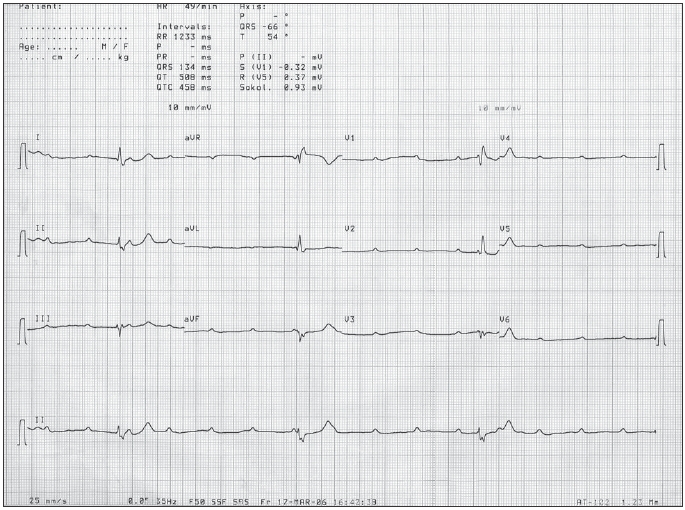
ECG from our patient on the day of arrival, showing a third degree atrioventricular conduction block.
Laboratory findings revealed severe hypothyroidism with a thyroid-stimulating hormone (TSH) level >100 pmol/l (normal range 0.3-5.0) and a free T4 of 2 pmol/l (normal range 9-24). Other findings revealed a renal insufficiency with urea of 25.1 mmol/l and creatinine 217 μmol/l.
Chest x-ray showed a grossly enlarged heart and pulmonary congestion. Transthoracic echocardiography showed normal left ventricular wall motion and mild aortic regurgitation.
An external pacemaker was inserted via the external femoral vein and pacing with a ventricular rate of 70 beats/min was initiated. We treated the patient with low-dose levothyroxine. After several days AV conduction was restored and the patient had a sinus rhythm of 40 beats/min. The external pacemaker was then removed.
Six weeks after presentation, the TSH had decreased to 28.9 pmol/l and the free T4 was within the normal range.
Three months after suppletion our patient had a sinus rhythm of 65 beats/min (figure 2). Her pretibial oedema had diminished and her renal function had returned to a normal level. Both TSH and free T4 had normalised. The renal insufficiency was thought to be secondary to a diminished cardiac output.
Figure 2.
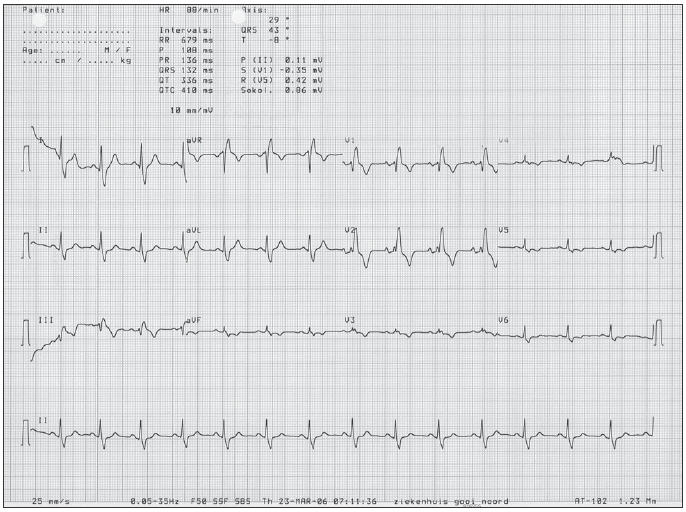
The ECG from our patient six weeks after starting treatment with levothyroxine. The AV block had completely disappeared. We see a sinus rhythm of 88 beats/min and a right bundle branch block.
Discussion
Elderly patients often present with syncope. Frequently, no apparent abnormalities are found. In some cases extreme bradycardia due to AV block may cause syncope. AV block is often caused by fibrosis or sclerosis of the conduction system secondary to ischaemic cardiac disease or drugs.
Another, less common, cause is of AV block is severe hypothyroidism. Since symptoms of hypothyroidism such as fatigue, cold intolerance, dry skin, constipation, depression, dyspnoea and oedema can easily be confused with symptoms of ageing, hypothyroidism is often underdiagnosed in the elderly population. The incidence of hypothyroidism varies from 1 to 17%, with women being more commonly affected than men.2,3 Dyspnoea and exercise intolerance due to skeletal muscular dysfunction, bradycardia with AV block, hypertension, poor cardiac contractility, dilatation, or pericardial effusion have also been described in association with hypothyroidism.2,3
In our case we describe a previously healthy elderly woman, taking no medication, who presented with a complete AV block and myxoedema. This prompted us to measure her TSH levels.
In patients with severe hypothyroidism, reversion of the conduction block to normal sinus rhythm is usually seen several days to weeks after thyroxin supplementation.4-6
Decades ago, several case reports presented similar cases describing complete AV block secondary to severe hypothyroidism.4-6 Recovery to sinus rhythm after treatment with levothyroxine was reported. We started treatment with low-dose levothyroxine and used a temporary pacemaker instead of implantation of a permanent pacemaker, expecting the thyroid levels to increase within one or two months.
As expected, our patient responded well to treatment with levothyroxine and implantation of a permanent pacemaker was avoided.
Conclusion
Our case study demonstrates that thyroid function abnormalities should always be tested when patients present with syncope due to AV conduction block, since the AV block may be caused by hypothyroidism. In these cases unnecessary pacemaker implantation can be avoided.
References
- 1.Braunwald E, editor. Heart disease: a textbook of cardiovascular medicine. Philadelphia: Saunders, 2001. [Google Scholar]
- 2.Laurberg P, Andersen S, Bulow Pedersen I, Carle A. Hypothyroidism in the elderly: pathophysiology, diagnosis and treatment. Drugs Aging 2005;22:23-8. [DOI] [PubMed] [Google Scholar]
- 3.Levy EG. Thyroid disease in elderly. Med Clin North Am 1991;75: 151-67. [DOI] [PubMed] [Google Scholar]
- 4.Singh JB, Starobin OE, Guerrant RL, Manders EK. Reversible atrioventricular block in myxedema. Chest 1973;63:582-5. [DOI] [PubMed] [Google Scholar]
- 5.Schantz ET, Dubbs AW, Allentown MD. Complete auriculoventricular block in myxedema with reversion to normal sinus rhythm on thyroid therarapy. Am Heart J 1951;41:613-9. [DOI] [PubMed] [Google Scholar]
- 6.Nakayama Y, Ohno M, Yonemura S, Uozumi H, Kobayakawa N, Fukushima K, et al. A case of transient 2:1 atrioventricular block, resolved by thyroxin supplementation for subclinical hypothyroidism. Pace 2006;29:106-8. [DOI] [PubMed] [Google Scholar]