

Abstract
Atrial fibrillation (AF), a common and serious cardiac rhythm disturbance, is responsible for substantial morbidity and mortality in the population. Currently about 2.3 million people in the US are diagnosed with AF and, based of the US census, this number is expected to rise to 5.6 million by 2050. It doubles in prevalence with each decade of age, reaching almost 9% at age 80–89 years. It has increased in prevalence over the calendar decades, reaching ‘epidemic’ proportions. This alarming increase in prevalence is incompletely explained by an increase in the population prevalence of elderly individuals, valve disease, heart failure or myocardial infarction. New onset AF also doubles with each decade of age, independent of the prevalence of known predisposing conditions.
Based Framingham Study data, men have a 1.5-fold greater risk of developing AF than women after adjustment for age and predisposing conditions. Of the standard cardiovascular risk factors, hypertension, diabetes and obesity are significant independent predictors of AF. Because of its high prevalence hypertension is responsible for more AF in the population (14%) than any other risk factor.
Adjusting for cardiovascular risk factors, heart failure, valvular heart disease and myocardial infarction substantially increase the likelihood of AF. Echocardiographic predictors of AF include left atrial enlargement, left ventricular fractional shortening, left ventricular wall thickness, and mitral annular calcification, offering prognostic information for AF beyond traditional clinical risk factors. Novel risk factors for AF include reduced vascular compliance, atherosclerosis, insulin resistance, environmental factors, inflammation and natriuretic peptides. There is emerging evidence that genetic variation also contributes to risk of atrial fibrillation.
The chief hazard of AF is a 4–5-fold increase in embolic stroke, assuming great importance in advanced age when it becomes a dominant factor. The attributable risk for stroke associated with AF increases steeply with age to 23.5% at age 80–89 years. AF is associated with a doubling of mortality in both sexes.
Synopsis
Atrial fibrillation (AF), an increasingly common dysrithmia, is responsible for substantial morbidity and mortality. Currently in the US about 2.3 million people are diagnosed with AF and, based on the US census, this number may rise to 5.6 million by 2050. Risk factors for AF include advancing age, cardiovascular disease and its risk factors. The chief hazard of AF is embolic stroke which is increased 4–5-fold, assuming great importance in advanced age when it becomes a dominant factor. AF is associated with about a doubling of mortality.
Introduction
Before the Framingham study report in 1982 there were many misconceptions about AF (1). Its prognosis was believed to be dependent on the underlying cardiac condition, not AF per se. AF unassociated with overt cardiovascular disease was considered a benign condition. Risk of embolism was not considered excessive unless the AF was intermittent or associated with mitral stenosis. The Framingham study report established that AF, further increased stroke risk associated with coronary heart disease and heart failure (1).
AF is responsible for substantial morbidity and mortality in the general population, chiefly from stroke and leads to more hospital admissions than any other dysrhythmia (2–4). In addition to often disabling symptoms and impaired quality of life, AF can precipitate heart failure and trigger potentially fatal ventricular dysrhythmias. Reflecting this widespread ‘epidemic’ of AF, data from US, Scottish and Danish studies reported a 2–2.5-fold increase in hospitalization rates for AF between the 1980’s and 1990’s (5–7).
AF doubles in prevalence with each decade of age and is becoming increasingly prevalent in the population. The reason for the alarming increase is largely unexplained. There is a need for new strategies to prevent AF and improve its treatment. Although newer pharmacological and non-pharmacological therapies are being developed, more effective measures are needed to treat AF safely and prevent its occurrence and its cardiovascular consequences.
Incidence, Prevalence and Lifetime Risk
AF is a highly prevalent sustained dysrhythmia. It is the most common cardiac rhythm disturbance treated in clinical practice, accounting for approximately one-third of hospitalizations for cardiac dysrhythmias. It is estimated to currently affect over 6 million patients in Europe and approximately 2.3 million in the United States, and this number continues to grow rapidly because of the increasing proportion of the ageing population with and without underlying heart disease. Reports from the Cardiovascular Health Study and the Framingham Study indicate that the incidence of AF per 1000 person-years in subjects under 64 years is 3.1 in men and 1.9 in women, rising sharply to about 19.2 per 1000 person-years in those 65–74 years, and is as high as 31.4–38.0 in octogenarians (8,9).
The estimated prevalence of AF in the general population is 0.4% to 1%, increasing with advancing age (10,13). AF is uncommon before 60 years of age, but the prevalence increases markedly thereafter, afflicting about 10% of the population by 80 years of age (13). The median age of AF patients is about 75 years with approximately 70% between 65 and 85 years of age. About one-third of all patients with AF are aged 80 years or older and it is estimated that by 2050 half will be in this age group (13).
Multiple studies of the incidence and prevalence of AF in the US, Europe and Australia have produced reasonably consistent findings (10). For reasons that are largely unexplained, the age-adjusted prevalence of AF in the US is greater in men than in women, both in a large cross-sectional study of adults enrolled in the Kaiser Permanente health maintenance organization and in the Framingham Study. Likewise, in the large population-based Rotterdam study, the prevalence of AF increased with age and was higher in men than in women in each age group, but the high lifetime risk of AF differed little between the sexes. ( 11)
Because of the more than half century surveillance of the Framingham Study cohort it was possible to determine the lifetime risk of developing AF which is 1 in 4 for men and women 40 years of age and older (12). These lifetime risks for AF remain high (1 in 6), even in the absence of antecedent predisposing conditions such as heart failure or myocardial infarction (Table 1). Prospective data from the Rotterdam Study, also found a high lifetime AF risk (22–24% at age 40 years) similar to North American epidemiological data. (11) The substantial lifetime risks underscore the major public health burden posed by AF and the need for further investigation into predisposing conditions, preventive strategies, and more effective therapies.
TABLE 1.
Lifetime Risk for AF in the Absence of Antecedent or Concurrent Diagnosis of CHF or Myocardial Infarction
| Index Age, y | Men | Women |
|---|---|---|
| Lifetime risk for AF without antecedent or concurrent CHF | ||
| 40 | 20.5 | 17.0 |
| 50 | 20.5 | 17.3 |
| 60 | 20.3 | 17.4 |
| 70 | 19.1 | 17.0 |
| 80 | 17.6 | 15.9 |
| Lifetime risk for AF without antecedent or concurrent CHF or myocardial infarction | ||
| 40 | 16.3 | 15.6 |
| 50 | 16.6 | 15.9 |
| 60 | 16.8 | 16.1 |
| 70 | 16.5 | 15.9 |
| 80 | 16.0 | 14.8 |
All values are percentages.
From: DM Lloyd-Jones et al. Circulation. 2004;110:1042–1046.
Most of the literature on the epidemiology of atrial fibrillation is based on white individuals residing in North American or Europe. (14) Based on limited data, the age-adjusted risk of developing AF in African-Americans is reported to be less than half of that in whites. AF is also less common among African-American than white patients with heart failure. (15–18)
Secular Trends
The prevalence of AF has increased over the past few decades, though studies have varied as to whether the increasing prevalence is restricted to men or both sexes. In the Copenhagen City Heart Study, the prevalence in men more than doubled from the 1970s to the 1990s, whereas the prevalence in women remained unchanged.(19) However, other studies show that it is increasing in both sexes (20,21). The alarming increase in numbers of patients with AF in the general population is not due to increasing use of the electrocardiogram in the community, because in the Framingham Study cohort electrocardiograms are routinely obtained on each examination; there was an age-adjusted secular increase in prevalence of AF on clinic electrocardiogram (5). Also in the Rochester population, utilization of the electrocardiogram increased by only 9–12%, over a 30-year period, whereas there was 2–3 fold increase in the prevalence of AF (22). In Denmark, standardizing by age and 10-year age group, the AF incidence rates approximately doubled for both men and women (197 per 100,000 in 1980 and 448 per 100,000 in 1999) (21)
A more credible explanation of the increasing prevalence of AF over time is that the elderly population of today has a higher prevalence of predisposing conditions for AF such as diabetes, obesity, heart failure, coronary and valvular heart disease, and prior cardiac surgery. This trend, brought about by advances in the treatment of cardiovascular disease, has produced a population of elderly survivors containing more candidates for AF than formerly. However, the Rochester study observed only modest increases in the prevalence of these predisposing conditions over a 3 decade period, that did not appear to more than partially explain the observed magnitude of the increase in prevalence of AF.(22)
US census projections for the next 50 years estimate that about 3 million Americans will have AF by the year 2020, increasing to 5.6 million by the year 2050, with more than half affected age 80 or older (13,23–25). The magnitude of these projections is may be underestimated because many episodes of AF go undetected.
Public Health Burden and Cost
AF, first described in 1909, has acquired increasing clinical and public health importance as a result of an expanding elderly population containing more vulnerable candidates (6). Data from a National Hospital Discharge Survey, indicate that hospital admissions resulting from AF increased two- to three fold from 1985 to 1999. During this period, hospitalizations listing AF increased from under 800 thousand to more than 2 million, predominantly in the elderly and men. Coyne et al assessing direct costs of treating AF in the US lists AF as one of the principal discharge diagnoses for 350,000 hospitalizations, and 5 million office visits in 2001. The total costs in 2005 dollars were estimated at 6.65 billion including 2.93 billion for hospitalizations. (26)
Data from both the United States and the United Kingdom indicate that AF is a costly public health problem. (27). Many factors contribute to the high cost of AF with hospitalizations constituting the major contributor (52%), followed by drugs (23%), consultations (9%), further investigations (8%), loss of work (6%), and paramedical procedures (2%). Globally, the annual cost per patient is close to $3600. Considering the prevalence of AF, the total economic burden is huge. (18)
Clinical Manifestations
AF may cause palpitations, fatigue, lightheadedness and dyspnea on exertion by precipitating cardiac failure. If there is underlying coronary artery disease it can initiate or aggravate angina from the associated rapid heart rate. However, AF often goes undetected because of lack of symptoms. It is frequently first detected by routine electrocardiographic examination, in the course of a myocardial infarction or stroke, on implanted pacemakers, or ambulatory ECG monitoring. AF was diagnosed incidentally in 12% of patients having an electrocardiogram for unrelated reasons in the Cardiovascular Health Study (16) and in 45% of patients in the Stroke Prevention in AF Trials (28) In a study of patients with paroxysmal AF, there were 12 times as many asymptomatic as symptomatic episodes of AF and 38% the patients with implanted pacemakers who experienced AF for more than 48 hrs were unaware of it (29). The low prevalence of AF in the absence of clinical and subclinical cardiovascular disease in the Cardiovascular Health Study of the elderly (1.6%) suggests that “lone atrial fibrillation” is fairly uncommon in the elderly (15).
Prognosis
AF is associated with an increased long-term risk of stroke, heart failure, and all-cause mortality, particularly in women.(30) The mortality rate of AF patients is about double that of patients in normal sinus rhythm and linked to the severity of underlying heart disease.(31–33) About two-thirds of the 3.7% mortality over 8.6 months in the ALFA Study was attributed to cardiovascular causes (34). However, AF independently predicts excess mortality and is associated with an increased incidence of embolic stroke, accounting for between 75,000 and 100,000 strokes per year in the USA (3). AF is in itself a powerful risk factor for stroke among patients of advanced age. The epidemic of AF in the 21st century is occurring in conjunction with a rising prevalence of heart failure, obesity, type-2 diabetes, and the prediabetic metabolic syndrome.(35)
The Framingham Study has shown that AF and heart failure often co-exist and that each may adversely impact the other (36). The decreased survival associated with AF occurs across a wide age range, partially attributable to the vulnerability of AF patients to development of heart failure. The differences in mortality reported among studies may be influenced by the proportion of deaths from heart failure as well as thromboembolism. In large heart failure trials AF is a strong independent risk factor for mortality and major morbidity. In the carvedilol or metoprolol European trial (COMET), there was no difference in all-cause mortality in subjects with AF at entry, but mortality increased in those who developed AF during follow-up.(37) In the Val-HeFT cohort of patients with chronic heart failure, development of AF was associated with significantly worse outcomes.(38) Heart failure promotes AF, AF aggravates failure, and persons with either share a poor prognosis. Thus, managing AF in conjunction with heart failure is a major challenge requiring more trial data to guide and optimize its management.
The most feared consequence of AF is stroke, the risk of which is increased 4–5-fold. AF assumes greater importance as a stroke hazard with advancing and by the ninth decade becomes a dominant factor. The attributable risk for stroke associated with AF increases steeply from 1.5% at age 50–59 years to 23.5% at age 80–89 years. AF is associated with a doubling of mortality in both sexes, which is decreased to 1.5–1.9-fold after adjusting for associated cardiovascular conditions. The decreased survival associated with AF occurs across a wide age range.
In the distant past, paroxysmal AF was considered more dangerous than persistent, chronic AF postulating that the former was more likely to embolize. The Framingham Study found chronic sustained AF to be at least as dangerous (1). Analysis of pooled data from five randomized controlled trials suggested that paroxysmal and chronic AF have similar risks for stroke (39). However, several studies have suggested higher mortality in persistent versus chronic AF (40, 41,42).
Risk Factors
Age and sex
As noted above AF increases with age, doubling in prevalence and incidence with each decade of age, even accounting for known predisposing conditions. Based on 38-year follow-up data from the Framingham Study, men had a 1.5-fold greater risk of developing AF than women after adjustment for age and predisposing conditions. The reason for the male preponderance of risk is currently unexplained (43).
Aging is accompanied by multiple cardiac abnormalities including: gradual loss of nodal fibers and increased fibrous and adipose tissue in the síno-atrial node, decreased ventricular compliance from myocardial fibrosis resulting in atrial dilatation that predisposes to AF, and extensive senile amyloid infiltration of the sinoatrial node may occur (44–46). In patients with AF, aging is associated with left atrial enlargement, reduced left atrial appendage flow velocity, all of which predispose to left atrial thrombus formation.(18). Prothrombin activation fragment and thrombin generation also increase with age, both in the general population and in persons with AF suggesting an age-related prothrombotic diathesis. Age appears to be a more potent risk factor for AF if it is combined with other risk factors (18). Also, aging also reflects longer exposure to predisposing conditions for AF, and even in advanced age some are clearly more vulnerable to the development of AF than others.
Cardiovascular Risk Factors
Of the major cardiovascular risk factors investigated by the Framingham study (9), hypertension and diabetes were significant independent predictors of AF, adjusting for age and other predisposing conditions (Table 2). Cigarette smoking was a significant risk factor in women adjusting only for age (OR = 1.4), but was just short of significance on adjustment for other risk factors. Neither obesity nor alcohol intake appeared to be independently associated with short-term risk (pooled logistic regression) of AF incidence in either sex. However, in other studies with sufficient power and individuals who consume alcohol at sufficiently high amounts, it appears that alcohol abuse is related to occurrence of AF.(47,48). As will be discussed below, obesity has been associated with long-term risk of atrial fibrillation (Cox model), which appears to be partially mediated by left atrial enlargement.
TABLE 2.
Cardiovascular Risk Factors for AF 38-Year Follow-up: Framingham Study
| Odds Ratios
|
||||
|---|---|---|---|---|
| Age-Adjusted
|
RF-Adjusted
|
|||
| Risk Factors
|
Men
|
Women
|
Men
|
Women
|
| Diabetes | 1.7† | 2.1‡ | 1.4* | 1.6† |
| ECG-LVH | 3.0‡ | 3.8‡ | 1.4 | 1.3 |
| Hypertension | 1.8‡ | 1.7‡ | 1.5† | 1.4* |
| Cigarettes | 1.0 | 1.4* | 1.1 | 1.4 |
| BMI | 1.03 | 1.02 | — | — |
| Alcohol | 1.01 | 0.95 | — | — |
p<0.05,
p<0.01,
p<0.001.
For men and women, respectively, diabetes conferred a 1.4- and 1.6-fold risk, and hypertension a 1.5- and 1.4-fold risk, after adjusting for other associated conditions. Because of its high prevalence, hypertension was responsible for more AF in the population (14%) than any other risk factor (9, 43).
Increased pulse pressure, a reflection of aortic stiffness, increases the cardiac load and has been shown to increase AF risk in the Framingham Study (49). Cumulative 20-year AF incidence rates were 5.6% for subjects with a pulse pressure 40 mm Hg or less (25th percentile) and 23.3% for those with a pulse pressure greater than 61 mm Hg (75th percentile). In models adjusted for age, sex, baseline and time dependent change in mean arterial pressure, and clinical risk factors for AF (body mass index, smoking, valvular disease, diabetes, electrocardiographic left ventricular hypertrophy, hypertension treatment, and prevalent myocardial infarction or heart failure), pulse pressure was associated with increased risk for AF (adjusted hazard ratio [HR], 1.26 per 20-mm Hg increment; 95% confidence interval [CI], 1.12–1.43; P=0.001).
In contrast, mean arterial pressure was unrelated to incident AF. Systolic pressure was related to AF (HR, 1.14 per 20-mm Hg increment; 95% CI, 1.04–1.25; P=0.006). However, when diastolic pressure was added, the model fit improved and the diastolic relation was inverse (adjusted HR, 0.87 per 10-mm Hg increment); consistent with a with a pulse pressure effect. Furthermore, the association between pulse pressure and AF persisted in models that adjusted for baseline left atrial dimension, left ventricular mass, and left ventricular fractional shortening (adjusted HR, 1.23; 95% CI, 1.09–1.39; P=.001). It appears that pulse pressure is an important risk factor for incident AF. Further research is needed to determine whether interventions that reduce pulse pressure can help retard the growing incidence of AF.
Diabetes was also a significant independent predictor of AF in 4 other studies, associated with an average relative risk of 1.8, but in 2 other studies it was not (18). Because the strength of diabetes as a predictor appears to be greater in lower-risk patients with AF, it is speculated that it may also be associated with non-cardioembolic strokes. Diabetes is a less powerful independent predictor than prior stroke/TIA, hypertension, or age, but further analysis is needed to refine its predictive value for thrombo-embolism in patients with AF. The reduction in stroke in warfarin-treated patients with diabetes was below average in 2 studies (18).
Thyroid Disease
Hyperthyroidism has long been implicated as a condition predisposing to AF. The prevalence of AF reported in patients at time of diagnosis of overt hyperthyroidism varies widely from 2–30 % (50–53). About 10–15% of persons with overt hyperthyroid disease and AF have been reported to have an arterial embolic event (53, 54,55). Studies have also suggested that subclinical abnormalities in thyroid stimulating hormone levels have detrimental effects on the cardiovascular system. In one small study based on samples from a central reference laboratory, AF developed in 3 of 32 subjects with subclinical hyperthyroidism over 2 years of follow-up, compared to none in 35 with normal thyrotropins (56).
Although AF is an acknowledged manifestation of hyperthyroidism, older people in whom AF is common, do not often have clinically overt hyperthyroidism but subclinical hyperthyroidism signified by a low serum thyrotropin is more common. It was not firmly established that subclinical hyperthyroidism imposed a risk for AF until the Framingham Study investigated this hypothesis. The Framingham Study examined prospectively the incidence of AF in relation to serum thyrotropin concentrations over 10-years in study participants over 60 years of age. A low serum thyrotropin (<0.1 mU per liter) was found to be associated with a threefold higher risk of developing AF over a decade after adjusting for other known risk factors.( 57).
The increased AF risk of hyperthyroidism was confirmed in the Cardiovascular Health Study of community-dwellers aged 65 years or older for whom baseline serum thyroid-stimulating hormone levels were measured and the relationship between baseline thyroid status and incident AF, incident cardiovascular disease, and mortality in older men and women not taking thyroid medication was determined (58). Eighty-two percent of participants (n = 2639) had normal thyroid function, 15% (n = 496) had subclinical hypothyroidism, 1.6% (n = 51) had overt hypothyroidism, and 1.5% (n = 47) had subclinical hyperthyroidism. After exclusion of those with prevalent AF, individuals with subclinical hyperthyroidism had a greater incidence of AF compared with those with normal thyroid function (67 events versus 31 events per 1000 person-years; (adjusted HR, 1.98; CI 1.29–3.03). No differences were seen between the subclinical hyperthyroidism and euthyroidism groups for incident coronary heart disease, stroke, cardiovascular death, or all-cause mortality. Likewise, there were no differences between the subclinical hypothyroidism or overt hypothyroidism groups and the euthyroidism group for cardiovascular outcomes or mortality. These data show an association between subclinical hyperthyroidism and development of AF but do not support the hypothesis that unrecognized subclinical hyperthyroidism or subclinical hypothyroidism is associated with other cardiovascular disorders that might predispose to AF.
Cardiovascular Conditions
Persons who develop AF are usually elderly and more likely than persons of the same age to have coronary disease, valvular heart disease, heart failure, echocardiographic abnormalities, or left ventricular hypertrophy (9,43). About 20% of men and a third of women have valvular heart disease, about a quarter of both sexes have heart failure and 28% of men and 14% of women have myocardial infarctions. These overt cardiac conditions impose a substantial risk. Adjusting for other relevant conditions, heart failure was associated with a 4.5- and 5.9-fold risk and valvular heart disease a 1.8- and 3.4-fold risk for AF in men and women, respectively. Myocardial infarction significantly increased the risk factor-adjusted likelihood of AF by 40% in men only (Table 3).
TABLE 3.
Odds of Developing AF for Specified Cardiac Conditions: Framingham Study Subjects Ages 55–94 Yr 38-Yr Follow-up
| Odds Ratios
|
||||
|---|---|---|---|---|
| Age-Adjusted
|
RF-Adjusted
|
|||
| Cardiac Conditions
|
Men
|
Women
|
Men
|
Women
|
| MI | 2.2† | 2.4† | 1.4* | 1.2 |
| Heart failure | 6.1‡ | 8.1‡ | 4.5‡ | 5.9‡ |
| Valve disease | 2.2‡ | 3.6‡ | 1.8† | 3.4‡ |
p<0.05,
p<0.01,
p<0.001
Echocardiographic Abnormalities
Valvular heart disease, echocardiographic enlargement of the left atrial dimension, and abnormal mitral or aortic valve function were independently associated with increased prevalence and incidence of AF in the Cardiovascular Health Study (8,15). Based on Framingham Study data, echocardiographic predictors of AF include left atrial enlargement (39% increase in risk per 5-mm increment), left ventricular fractional shortening (34% per 5% decrement), and left ventricular wall thickness (28% per 4-mm increment). (Table 4) These echocardiographic features offer prognostic information for AF beyond the traditional clinical risk factors (43,59).
Table 4.
Echocardiographic Predictors of Atrial Fibrillation: Framingham Study Subjects ages 50–59 Years
| Echocardiographic | Atrial Fibrillation |
|---|---|
| Features | Risk |
| Left Atrial Size | 29% incr. per 5mm |
| Left Ventricular Fractional Shortening | 34% incr. per 5% |
| Left Ventricular wall thickness | 28% incr. per 4 mm |
| Two or more of above vs none | 17% vs 3.7% |
Vazirí SM, et al Circulation 1994; 89:724–730.
Mitral annular calcification is associated with adverse cardiovascular disease outcomes and stroke in longitudinal and community-based cohorts. Prospective data are limited on its association with AF. The Framingham study investigated the association between mitral annular calcification and long-term risk of AF (over 16 years of follow-up) in participants in the original cohort attending routine examinations between 1979 and 1981 (60). The age- and sex-adjusted incidence rate the condition was 362 per 10,000 person-years in subjects with mitral annular calcification compared with 185 per 10,000 person-years in those without it. In multivariable-adjusted analyses, mitral annular calcification was associated with 1.6 fold increased risk of AF. This association was attenuated somewhat upon further adjustment for left atrial size (HR 1.4, 95% CI 0.9–2.0) suggesting that the association between mitral annular calcification and incident AF is only partially mediated through left atrial enlargement (60).
In a double-blind randomized parallel-group study of 8831 men and women with hypertension and ECG left ventricular hypertrophy enrolled in the Losartan Intervention for Endpoint Reduction in hypertension Study, the occurrence of new onset AF was investigated in relation to in-treatment regression or continued absence of ECG left ventricular hypertrophy (61). Quantified regression of ECG left ventricular hypertrophy was found to be associated with a reduced likelihood of new onset AF, independent of blood pressure lowering and treatment.
Novel Risk Factors
A large number of novel risk factors for AF that have been identified, some modifiable, and some not. These include: inflammatory markers, the obesity-induced metabolic syndrome, insulin resistance, thrombogenic tendencies, sleep apnea, decreased arterial compliance, left atrial volume and diastolic dysfunction.
Inflammation
The suspicion that inflammation contributes to some types of AF is supported by the frequent occurrence of AF after cardiac surgery (25% to 40%), genetic studies and the association of AF with pericarditis and myocarditis. The time course of AF following cardiac surgery parallels activation of the complement system and release of proinflammatory cytokines.(62,63)
C-reactive protein, a sensitive marker of inflammation, is a predictor of adverse cardiac events that has recently been linked to AF (64,65). In the Cardiovascular Health Study a large, population-based study of cardiovascular disease in the elderly, C-reactive protein was independently associated with the presence of AF at baseline and also predicted patients at increased risk for developing future AF.(67). It is not clear whether indices of inflammation should be regarded as direct risk factors for AF by causing an atrial inflammatory state, or whether these are markers for the underlying atherosclerotic vascular disease.
Insulin risistance and the metabolic syndrome
Concurrently, the prevalence of obesity, diabetes, and the metabolic syndrome have reached major proportions around the world. In a retrospective analysis of the incidence of AF in relation to body mass index in consecutive cardiac surgery patients obesity was reported to be an important determinant of new-onset AF after cardiac surgery (68). It has been unclear as to what extent cardiovascular risk factors mediate the association between obesity and AF. In a population-based Veterans Administration case-control study of subjects with new-onset AF and controls identified through medical record review of inpatient and outpatient visits, the association of AF with BMI appeared to be partially mediated by diabetes mellitus but minimally through other cardiovascular risk factors (69)
Obesity is associated with atrial enlargement and ventricular diastolic dysfunction, which are established predictors of AF. The Framingham Study investigated the association between body mass index and the long-term risk of developing new onset of AF in a prospective, community-based observational cohort (70). During a mean follow-up of 13.7 years, age-adjusted incidence rates for AF were found to increase across the 3 body mass index categories (normal, overweight, and obese) in men (9.7, 10.7, and 14.3 per 1000 person-years) and women (5.1, 8.6, and 9.9 per 1000 person-years). In multivariable models adjusted for cardiovascular risk factors and interim myocardial infarction or heart failure, a 4% increase in AF risk per 1-unit increase in BMI was observed in men and women. The adjusted hazard ratios for AF associated with obesity were 1.5 for men and women, compared with individuals with normal BMI. After adjustment for echocardiographic left atrial diameter in addition to clinical risk factors, BMI was no longer associated with AF risk. It was concluded that obesity is an important, potentially modifiable risk factor for AF, the excess risk of which appears to be mediated chiefly by left atrial dilatation. These prospective data suggest that interventions to promote normal weight may reduce the population burden of AF.
The inter-relationship between obesity, diabetes and the metabolic syndrome strongly suggests an insulin resistant state. In a prospective analysis of consecutive hospitalized patients in sinus rhythm and without obvious structural heart disease, paroxysmal AF or flutter occurred in 9% of the patients with metabolic syndrome, but only 4% of patients without the syndrome (p=0.02). Multivariate logistic regression analysis indicated that the metabolic syndrome was a significant risk factor that was independent of left atrial diameter or age (odds ratio 2.8 p<0.01). Among the 5 components of the metabolic syndrome, body mass index was the most strongly associated with AF/Flutter (OR; 3.0, p=0.02). It was concluded that the metabolic syndrome is strongly associated with AF/Flutter in patients without structural heart diseases and that obesity may be an important underlying mechanism. (71)
A community-based, cross-sectional observational study conducted in a primary health care facility in Sweden explored the prevalence of AF in patients with hypertension and type 2 diabetes seeking possible mechanisms for its development. An association of AF with combined hypertension and type-2 diabetes was found that remained significant when adjusted for other cardiovascular disease risk factors. Body mass index AF risk was attenuated by adjustment for ischemic ECG findings and lost significance with adjustment for insulin resistance, OR 1.3 (0.5–3.1). It was suggested that AF may be associated with the combined occurrence of type 2 diabetes and hypertension because of insulin (72).
Given the evidence that the metabolic syndrome is pro-inflammatory and that AF has been linked to inflammation, the relationship of these risk factors to incident AF merits further investigation. The finding that new onset AF is significantly related to BMI in multivariate analysis, adjusting for age and sex also has some credibility because obesity is an independent predictor of diastolic dysfunction, also a major determinant of AF (73).
Stature
Data from, a multicenter registry of patients with impaired left ventricular function (ADVANCENT) were used to investigate the influence of stature on AF in high-risk patients with reduced left ventricular systolic function (74). Because left atrial size is strongly associated with stature it was hypothesized that height and body surface area are risk factors for AF, independent of other known associations. The study was based on 25,268 patients (mean age of 66 years) consisting mostly of white men (72%) with ischemic cardiomyopathy (72%), and with a mean left ventricular ejection fraction of 31%.
A history of AF was present in 7,027 patients (27.8%). AF prevalence was found to increase significantly between the lowest and highest height quartiles (32% relative increase, p<0.0001). In multivariable analysis, the effect of height on AF risk persisted after adjusting for age, sex, race, left ventricular ejection fraction, heart failure class and etiology, hypertension, diabetes, and medication use. In patients with LV dysfunction, increasing stature appears to portend a higher risk of AF after accounting for other traditional risk factors for the arrhythmia. This association may account for some of the higher prevalence of AF in men (74) Height has also been observed to be associated with an increased risk of incident AF in the community (hazard ratio 1.03 per cm [1.02–1.05]).(8).
Plasma Natriuretic Peptides
Obesity-promoted natriuretic peptides are secreted from cardiomyocytes. They play a fundamental role in cardiovascular remodeling, volume homeostasis, and response to ischemia. Investigation of the relation of B-type natriuretic peptide and N-terminal pro-atrial natriuretic peptide by the Framingham Study has shown these natriuretic peptides to be associated with an increased risk of AF and its predisposing cardiovascular conditions such as heart failure and stroke (75) (Table 5).
Table 5.
Plasma B-Type Natriuretic Peptides and Risk of CVD: Framingham Study
| CVD Event | % increase in CVD Per SD Increment | M-V H.R# > 80th Percentile |
|---|---|---|
| Heart Failure | 77% | 3.1** |
| Arial Fibrillation | 66% | 1.9* |
| Stroke/TIA | 53% | 2.0* |
| First CV Event | 28% | 1.8* |
| Death | 27% | 1.6* |
Peptide Levels not significantly related to CHD
Adjusted for: age, diabetes, BP, smoking, creatinine, LV mass and systolic function. 80th percentile BNP: women 23.3 pg/ml, men 20 pg/ml
P<.05,
P<.01
Wang TJ, et al. N Engl J Med 2004: 350:655-663.
Sleep apnea
There is a well documented relationship between obesity and sleep apnea, but the prevalence of sleep disordered breathing is also substantial in the non-obese. A high recurrence of AF in patients undergoing cardioversion is reported and AF recurrences are found to be more common in untreated than treated obstructive sleep apnea. Patients undergoing cardioversion are reported to have a 49% prevalence of sleep apnea compared with a 39% frequency among other cardiac patients without AF, which is not attributable other predisposing conditions. (76,77) Mechanisms postulated include: hypoxia, hypercarbia, autonomic imbalance, stretching of the atrium and left ventricular wall stress. Increased right-sided cardiac pressure stimulates atrial natriuretic peptide release that is noted in AF. Prospective studies of the relationship of sleep-disordered breathing with AF are needed, taking into account the sleep apnea relationship to obesity, the metabolic syndrome, coronary artery disease, heart failure, and stroke (78,79).
Diastolic dysfunction
Diastolic dysfunction, is a common accompaniment of ageing, hypertension, obesity, diabetes, heart failure and coronary artery disease in the elderly. Elderly patients in sinus rhythm at the time of an echocardiographic examination, were found to develop of AF at a 1% rate with mild diastolic dysfunction compared with 12% with moderate diastolic dysfunction, and 20% severe diastolic dysfunction. Diastolic dysfunction provides additional predictive information, for development of AF over that obtained from the clinical risk factors. As left atrial volumes increase diastolic function deteriorates providing predictive information for the development of AF and stroke (80,81). Furthermore, left atrial volume is a predictor of other cardiovascular events including myocardial infarction, stroke, and coronary revascularization all of which predispose to AF. (82,83)
AF as a Stroke Risk Factor
AF is an established major independent risk factor for embolic stroke or transient ischemic attack; AF is associated with a 4–5-fold greater risk than in the unaffected population (3). However, there is also evidence that a stroke may precipitate the occurrence of AF, because of its hemodynamic and autonomic consequences. About half of all elderly AF patients have hypertension as a major risk factor for stroke. Hypertension is a powerful independent predictor of stroke in AF, and an important risk factor for developing AF. The strong association between AF, hypertension, and stroke could depend on reduced aortic compliance, left ventricular hypertrophy, diastolic dysfunction, and left atrial dilatation, giving rise to stasis and thrombus formation.(28,84,85).
AF accounts for about 45% of all embolic strokes. The risk of stroke in placebo-treated patients in randomized warfarin trials is reported as 4.5% per year (84,86). A collaborative analysis of five randomized trials, by the AF Investigators identified five major risk factors for stroke in AF patients; namely, prior stroke or transient ischemic attack, a history of hypertension, advanced age, a history of heart failure, and diabetes (85) (Table 6). The risk of stroke increases at least five-fold in patients with clinical risk factors, and this is in marked contrast to the low risk of stroke in younger patients without clinical risk factors. Other factors, such as female sex, systolic blood pressure over 160 mm Hg, and left ventricular dysfunction, have been variably linked to stroke.
TABLE 6.
Risk Factors for Ischemic Stroke and Systemic Embolism in Patients with Nonvalvular Atrial Fibrillation
| Risk Factors | Relative Risk |
|---|---|
| Previous stroke or TIA | 2.5 |
| Diabetes mellitus | 1.7 |
| History of hypertension | 1.6 |
| Heart failure | 1.4 |
| Advanced age (continuous, per decade) | 1.4 |
Data derived from collaborative analysis of 5 untreated control groups in primary prevention trials.47 As a group, patients with AF carry about a 6-fold increased risk of thromboembolism compared with patients in sinus rhythm. Relative risk refers to comparison of patients with AF to patients without these risk factors.
TIA indicates transient ischemic attack.
Source:. Analysis of pooled data from five randomized controlled trials Arch Intern Med. 1994; 154: 1449–57.
In patients 80 to 89 years old, 36% of strokes occur in those with AF. The annual risk of stroke for octogenarians with AF is in the range of 3% to 8% per year, depending on associated stroke risk factors.(3) The powerful impact of age and clinical risk factors on the risk of stroke in patients with AF suggests that vigorous control of accompanying risk factors should be undertaken to lower the risk.
Ischemic stroke and systemic arterial occlusion in AF are generally attributed to embolism of thrombus from the left atrium, however, up to 25% of strokes in patients with AF may be due to intrinsic cerebrovascular diseases, other cardiac sources of embolism, or atherosclerotic pathology in the proximal aorta (18, 84). Although 12% harbor carotid artery stenosis, carotid atherosclerosis is not substantially more prevalent in AF patients with stroke and appears to be a relatively minor contributing factor.(87,88)
Genetic Influences
Familial occurrence of AF has been recognized for many years, but was considered uncommon. The Framingham Study found that parental AF increases the future risk for offspring AF about 2–3-fold after excluding persons with predisposing conditions, an observation supporting a genetic susceptibility to developing this dysrhythmia (89). (Figure 1). In such families with AF, familial linkage studies are beginning to explore the genetics of AF, particularly in younger persons. (90,91)
Figure 1.

Risk of Atrial Fibrillation by Parental Atrial Fibrillation Status: Framingham Offspring Cohort
Purported genetically determined constitutional factors such as blood pressure, obesity and greater stature, have been found to predispose to AF. It is uncertain how these constitutional factors promote AF, but metabolic disorders and genetic factors seem to be implicated.
Identification of a gene defect linked to chromosome 10q in a Spanish family, nearly half the members of which had AF, supports the hypothesis of familial AF (91,93). However, the majority of patients with AF in these families are younger, than age 65 years suggesting that the postulated genes causing AF may not be directly involved in the elderly
The National Heart Lung and Blood Institute is sponsoring several projects that will examine the genetic contribution to AF and other cardiovascular phenotypes in the community. Two studies in particular will genotype 1000s of candidate genes (Candidate gene Association REsource, “CARE” project) and a 550K genome wide scan of genetic polymorphisms (SNP Health Association Resource, SHARe) with 1000s of participants across many of the NHLBI’s cohort studies. The data from these studies will be available for analysis to investigators with approved projects and ethnical oversight. The aggregate results of these studies will be web-posted (http://www.ncbi.nlm.nih.gov/projects/gap/cgi-bin/study.cgi?id=phs000007). Over the next decade the advent of large scale genotyping efforts will undoubtedly lead to major advances in understanding the contribution of common complex genetic variation to AF in the community.
Multivariable Risk Assessment
Multivariable risk assessment of the stroke risk of patients with AF is desirable for selecting those who most and least need aggressive anticoagulant therapy. The number needed to treat to prevent one event is inversely related to the level of risk. Estimating the risk of stroke for individual AF patients is crucial for the decision to prescribe anticoagulation therapy, but the threshold risk warranting anticoagulation is controversial. Patients with a stroke risk of 2% per year or less do not benefit substantially from oral anticoagulation, and it would require treating 100 or more patients for 1 year to prevent a single stroke (18). For high-risk AF patients, with stroke rates of 6% per year or greater, the comparable number needed-to-treat is 25 or fewer, strongly favoring anticoagulation. For patients at intermediate stroke risk (annual rate 3% to 5%) opinion about routine anticoagulation remains divided.
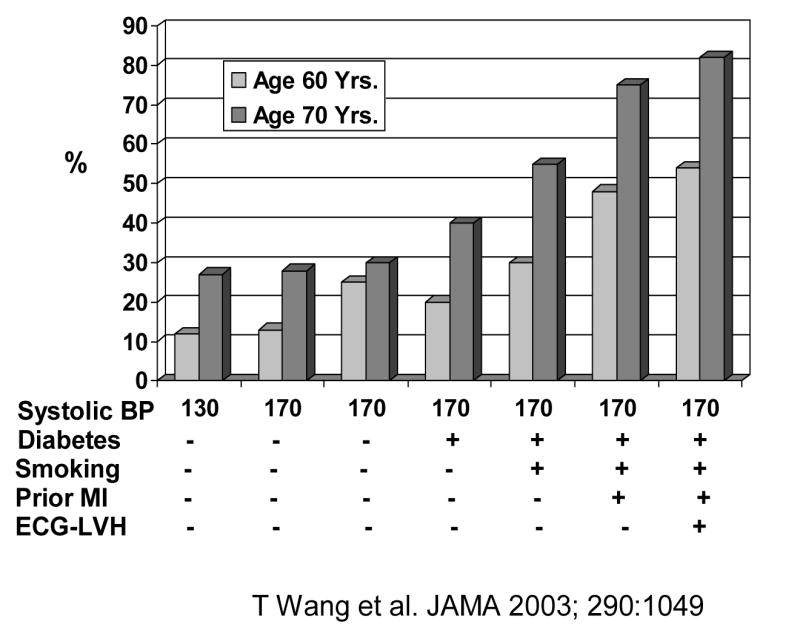
AF is a major component of the Framingham stroke risk prediction algorithm (3). Framingham Study investigators sought to further risk stratify and elucidate which individuals with AF were at particularly increased risk of stroke or stroke and death (94). Their multivariable analysis examined risk factors for stroke among 705 patients with recently detected AF, excluding those who had sustained ischemic stroke, TIA, or death within 30 days of diagnosis (Figure 2). The significant predictors of ischemic stroke in subjects with AF were age (RR = 1.3 per decade), female sex (RR = 1.9), prior stroke or TIA (RR = 1.9), and diabetes mellitus (RR = 1.8). Systolic blood pressure became a significant predictor of stroke if warfarin was included in a time-dependent Cox proportional hazards model. With a scoring system based on age, gender, systolic hypertension, diabetes, and prior stroke or TIA, the proportion of patients classified as low risk varied from 14.3% to 30.6% depending upon whether selected stroke rate thresholds were less than 1.5% per year or less than 2% per year.
Figure 2.
5-Year Stroke/Death Risk in Atrial Fibrillation Framingham Study
Preventive Measures
AF remains a substantial global health burden requiring detection of candidates likely to develop it for preventive management. The disappointing results of anti-dysrhythmic therapy for AF require a therapeutic approach that focuses treatment on the underlying myocardial pathology leading to the occurrence of the AF. Many risk factors for AF are shared by other cardiac conditions that in turn predispose to the occurrence of AF. The premordial prevention of the risk factors would jointly prevent their emergence and in turn the AF they promote. Identification of modifiable risk factors specific for AF enables intervention early in the course of the disease when preventative or corrective strategies are most efficient. Improvement of the multivariable risk profile to prevent a stroke, coronary disease or cardiovascular disease in general should carry a bonus of prevention of AF
For example, ACE-inhibitors and angiotensin receptor blockers, which are recommended for hypertensive cardiovascular disease, appear to reduce the rate of recurrence of AF after cardioversion and protect against development of AF in patients with left ventricular dysfunction.(95,96). They may also inhibit the pro-inflammatory and sympathetic effects of angiotensin and interfere with the triggers and substrate of AF (18).
Warfarin anticoagulant therapy is highly effective for prevention of strokes in patients with AF, reducing the risk by 62% (28,84). Meta-analysis according to the principle of intention to treat showed that adjusted-dose oral anticoagulation is highly efficacious for prevention of all stroke (both ischemic and hemorrhagic), with a risk reduction of 62% (95% CI 48% to 72%) versus placebo (84). This reduction was similar for both primary and secondary prevention and for both disabling and non-disabling strokes. Using “on-treatment analysis” (excluding patients not on oral anticoagulation at the time of stroke) the preventive efficacy of oral anticoagulation exceeded 80%. Despite this a survey of treatment for patients with CVD indicates that only 50% are being treated to recommended standards of care. The deficits found in adherence to recommended processes for basic care for cardiovascular disease in general and AF in particular pose serious threats to the health of the American public. Strategies to reduce these deficits in care are urgently needed.
Summary
We are confronted with a rapidly growing epidemic of AF, the scope of which urgently demands improved prevention and treatment of this condition and its predisposing cardiovascular substrate. The cardiovascular conditions associated with AF are justifiably considered risk factors rather than risk markers. It is also likely that AF and the left atrial enlargement associated with it are direct causes of embolic stroke requiring, early detection and treatment. AF is now a global health burden requiring targeted screening to detect persons likely to develop this condition.
The disappointing results of therapy to suppress or eliminate the rhythm disturbance have focused greater attention on treatment to prevent or delay myocardial changes leading to the occurrence of the AF. Many risk factors associated with AF also predispose to cardiovascular diseases that beget the development of AF so that their eradication should theoretically confer a substantial public health and healthcare benefit. Identification and treatment of modifiable risk factors specific for AF in high-risk candidates for the condition would enable early intervention when preventative or corrective measures are most effective. In addition, advances in identifying genetic and biological markers of risk for AF and its complications will provide pathophysiological insights and enable better risk stratification for more personalized and targeted therapy.
Acknowledgments
N01-HC 25195; RO1 HL076784; 1R01 AG028321; 6R01-NS 17950
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Kannel WB, Abbott RD, Savage DD, et al. Epidemiologic features of chronic atrial fibrillation: the Framingham Study. N Engl J Med. 1982;306:1018–1022. doi: 10.1056/NEJM198204293061703. [DOI] [PubMed] [Google Scholar]
- 2.Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, et al. Impact of atrial fibrillation on risk of death: the Framingham study. Circulation. 1999;98:946–52. doi: 10.1161/01.cir.98.10.946. [DOI] [PubMed] [Google Scholar]
- 3.Wolf PA, Abbot RD, Kannel WB. Atrial fibrillation as independent risk factor for stroke: the Framingham study. Stroke. 1991;22:983–8. doi: 10.1161/01.str.22.8.983. [DOI] [PubMed] [Google Scholar]
- 4.Bialy D, Lehnmann MH, Schumacher DN, et al. Hospitalization for arrhythmias in the United States. Importance of atrial fribrillation. J Am Coll Cardiol. 1992;19:41A. Abstract. [Google Scholar]
- 5.Wolf PA, Benjamin EJ, Belanger AJ, et al. Secular trends in the prevalence of atrial fibrillation: the Framingham study. Am Heart J. 1996;131:790–5. doi: 10.1016/s0002-8703(96)90288-4. [DOI] [PubMed] [Google Scholar]
- 6.Stewart S, MacIntyre K, MacLeod MMC, Bailey AEM, Capewell S, McMurray JJV. Trends in hospital activity, morbidity and case fatality related to atrial fibrillation in Scotland, 1986–1996. Eur Heart J. 2001;22:693–701. doi: 10.1053/euhj.2000.2511. [DOI] [PubMed] [Google Scholar]
- 7.Frost L, Engholm G, Møller H, Husted S. Decrease in mortality in patients with a hospital diagnosis of atrial fibrillation in Denmark during the period 1980–1993. Eur Heart J. 1999;20:1592–9. doi: 10.1053/euhj.1999.1713. [DOI] [PubMed] [Google Scholar]
- 8.Psaty BM, Manolio TA, Kuller LH, et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997;96:2455–2461. doi: 10.1161/01.cir.96.7.2455. [DOI] [PubMed] [Google Scholar]
- 9.Benjamin EJ, Levy D, Vaziri SM, D’Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort: the Framingham heart study. JAMA. 1994;271:840–4. [PubMed] [Google Scholar]
- 10.Feinberg WM, Blackshear JL, Laupacis A, et al. Prevalence, age distribution and gender of patients with atrial fibrillation: analysis and implications. Arch Intern Med. 1995;155:469–473. [PubMed] [Google Scholar]
- 11.Heeringa J, van der Kuip DAM, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27:949–953. doi: 10.1093/eurheartj/ehi825. [DOI] [PubMed] [Google Scholar]
- 12.Lloyd-Jones DM, Wang TJ, Leip E, et al. Lifetime Risk for Development of Atrial Fibrillation The Framingham Heart Study. Circulation. 2004;110:1042–1046. doi: 10.1161/01.CIR.0000140263.20897.42. [DOI] [PubMed] [Google Scholar]
- 13.Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–5. doi: 10.1001/jama.285.18.2370. [DOI] [PubMed] [Google Scholar]
- 14.Ryder KM, Benjamin EJ. Epidemiology and significance of atrial fibrillation. Am J Cardiol. 1999;84:131R–138R. doi: 10.1016/s0002-9149(99)00713-4. [DOI] [PubMed] [Google Scholar]
- 15.Furberg CD, Psaty BM, Manolio TA, et al. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study) Am J Cardiol. 1994;74:236–241. doi: 10.1016/0002-9149(94)90363-8. [DOI] [PubMed] [Google Scholar]
- 16.Psaty BM, Manolio TA, Kuller LH, et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997;96:2455–61. doi: 10.1161/01.cir.96.7.2455. [DOI] [PubMed] [Google Scholar]
- 17.Ruo B, Capra AM, Jensvold NG, et al. Racial variation in the prevalence of atrial fibrillation among patients with heart failure: the Epidemiology, Practice, Outcomes, and Costs of Heart Failure (EPOCH) study. J Am Coll Cardiol. 2004;43:429–35. doi: 10.1016/j.jacc.2003.09.035. [DOI] [PubMed] [Google Scholar]
- 18.Writing committee for ACC/AHA/ESC. 2006 Guidelines for the management of patients with atrial fibrillation. Circulation. 2006;114:e257–e354. doi: 10.1161/CIRCULATIONAHA.106.177292. [DOI] [PubMed] [Google Scholar]
- 19.Friberg J, Scharling H, Gadsboll N, et al. Sex-specific increase in the prevalence of atrial fibrillation (The Copenhagen City Heart Study) Am J Cardiol. 2003;92:1419–23. doi: 10.1016/j.amjcard.2003.08.050. [DOI] [PubMed] [Google Scholar]
- 20.DeWilde S, Carey IM, Emmas C, et al. Trends in the prevalence of diagnosed atrial fibrillation, its treatment with anticoagulation and predictors of such treatment in UK primary care. Heart. 2006;92:1064–1070. doi: 10.1136/hrt.2005.069492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Frost L, Vestergaard P, Mosekilde L, Mortensen LS. Trends in incidence and mortality in the hospital diagnosis of atrial fibrillation or flutter in Denmark, 1980–1999. Int J Cardiol. 2005 doi: 10.1016/j.ijcard.2004.08.024. [DOI] [PubMed] [Google Scholar]
- 22.Tsang TS, Petty GW, Barnes ME, et al. The prevalence of atrial fibrillation in incident stroke cases and matched population controls in Rochester, Minnesota: changes over three decades. J Am Coll Cardiol. 2003;42:93–100. doi: 10.1016/s0735-1097(03)00500-x. [DOI] [PubMed] [Google Scholar]
- 23.Gillum R. Trends in acute myocardial infarction and coronary heart disease death in the United States. J Am Coll Cardiol. 1994;23:1273–1277. doi: 10.1016/0735-1097(94)90367-0. [DOI] [PubMed] [Google Scholar]
- 24.McGovern PG, Jacobs DR, Jr, Shahar E, et al. Trends in acute coronary heart disease mortality, morbidity, and medical care from 1985 through 1997: the Minnesota Heart Survey. Circulation. 2001;104:19–24. doi: 10.1161/01.cir.104.1.19. [DOI] [PubMed] [Google Scholar]
- 25.Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: implications for primary prevention. Circulation. 2003;108:711–716. doi: 10.1161/01.CIR.0000083722.42033.0A. [DOI] [PubMed] [Google Scholar]
- 26.Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9:348–356. doi: 10.1111/j.1524-4733.2006.00124.x. [DOI] [PubMed] [Google Scholar]
- 27.Stewart S, Murphy N, Walker A, McGuire A, McMurray JJ. Cost of an emerging epidemic: an economic analysis of atrial fibrillation in the UK. Heart. 2004;90:286–292. doi: 10.1136/hrt.2002.008748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.The SPAF III Writing Committee for the Stroke Prevention in Atrial Fibrillation Investigators. Patients with nonvalvular atrial fibrillation at low risk of stroke during treatment with aspirin: stroke prevention in atrial fibrillation. III [PubMed] [Google Scholar]
- 29.Israel CW, Gronefeld G, Ehrlich JR, et al. Long-term risk of recurrent atrial fibrillation as documented by an implantable monitoring device: implications for optimal patient care. J Am Coll Cardiol. 2004;43:47–52. doi: 10.1016/j.jacc.2003.08.027. [DOI] [PubMed] [Google Scholar]
- 30.Stewart S, Hart CL, Hole DJ, et al. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113:359–64. doi: 10.1016/s0002-9343(02)01236-6. [DOI] [PubMed] [Google Scholar]
- 31.Kannel WB, Abbott RD, Savage DD, et al. Coronary heart disease and atrial fibrillation: the Framingham Study. Am Heart J. 1983;106:389–6. doi: 10.1016/0002-8703(83)90208-9. [DOI] [PubMed] [Google Scholar]
- 32.Krahn AD, Manfreda J, Tate RB, et al. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba Follow-Up Study. Am J Med. 1995;98:476–84. doi: 10.1016/S0002-9343(99)80348-9. [DOI] [PubMed] [Google Scholar]
- 33.Flegel KM, Shipley MJ, Rose G. Risk of stroke in non-rheumatic atrial fibrillation. Lancet. 1987;1:526–529. doi: 10.1016/s0140-6736(87)90174-7. [published erratum appears in Lancet 1987; 1:878] [DOI] [PubMed] [Google Scholar]
- 34.Levy S, Maarek M, Coumel P, et al. Characterization of different subsets of atrial fibrillation in general practice in France: the ALFA study. The College of French Cardiologists. Circulation. 1999;99:3028–35. doi: 10.1161/01.cir.99.23.3028. [DOI] [PubMed] [Google Scholar]
- 35.Braunwald E. Shattuck lecture—cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. doi: 10.1056/NEJM199711063371906. [DOI] [PubMed] [Google Scholar]
- 36.Wang TJ, Larson MG, Levy D, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107:2920–2925. doi: 10.1161/01.CIR.0000072767.89944.6E. [DOI] [PubMed] [Google Scholar]
- 37.Swedberg K, Olsson LG, Charlesworth A, et al. Prognostic relevance of atrial fibrillation in patients with chronic heart failure on long-term treatment with beta –blockers. Eur Heart J. 2005;26:1303–1308. doi: 10.1093/eurheartj/ehi166. [DOI] [PubMed] [Google Scholar]
- 38.Maggioni AP, Latini R, Carson PE, et al. Valsartan reduces the incidence of atrial fibrillation in patients with heart failure: results from the Valsartan Heart Failure Trial (Val-HeFT) Am Heart J. 2005;149:1–10. doi: 10.1016/j.ahj.2004.09.033. [DOI] [PubMed] [Google Scholar]
- 39.Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic treatment in atrial fibrillation: analysis of pooled data from five randomized controlled studies. Arch Intern Med. 1994;154:1449–1457. [PubMed] [Google Scholar]
- 40.Heuzey JYLE, Paziaud O, Piot O, Said MA, Copie X, Lavergne T, Guize L. Cost of care distribution in atrial fibrillation patients: the COCAF study. Am Heart J. 2004;147:121–126. doi: 10.1016/s0002-8703(03)00524-6. [DOI] [PubMed] [Google Scholar]
- 41.Keating RJ, Gersh BJ, Hodge DO, Weivoda PL, Patel PJ, Hammill SC, Shen WK. Effect of atrial fibrillation pattern on survival in a community-based cohort. Am J Cardiol. 2005;96:1420–1424. doi: 10.1016/j.amjcard.2005.07.050. [DOI] [PubMed] [Google Scholar]
- 42.Ruigomez A, Johansson S, Wallander MA, Garcia Rodriguez LA. Predictors and prognosis of paroxysmal atrial fibrillation in general practice in the UK. BMC Cardiovasc Disord. 2005:20. doi: 10.1186/1471-2261-5-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kannel WB, Wolf PA, Benjamin EJ, et al. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. doi: 10.1016/s0002-9149(98)00583-9. [DOI] [PubMed] [Google Scholar]
- 44.Falk RH. Etiology and complications of atrial fibrillatíon: Insights from pathology studies. Am J Cardiol. 1998;82:10N–176N. doi: 10.1016/s0002-9149(98)00735-8. [DOI] [PubMed] [Google Scholar]
- 45.Manyari DE, Patterson C, Johnson D, et al. Atrial and ventricular arrhythmias in asymptomatic elderly subjects. Correlation with left atrial size and left ventricular mass. Am Heart J. 1990;119:1069–1076. doi: 10.1016/s0002-8703(05)80236-4. [DOI] [PubMed] [Google Scholar]
- 46.Lie JT, Hammond PI. Pathology of the senescent heart: anatomic observations on 237 autopsy studies of patients 90~105 years old. Mayo Clin Proc. 1998;63:552–564. doi: 10.1016/s0025-6196(12)64885-x. [DOI] [PubMed] [Google Scholar]
- 47.Mukamal KJ, Tolstrup JS, Friberg J, Jensen G, Gronbaek M. Alcohol consumption and risk of atrial fibrillation in men and women: the Copenhagen City Heart Study. Circulation. 2005;112:1736–1742. doi: 10.1161/CIRCULATIONAHA.105.547844. [DOI] [PubMed] [Google Scholar]
- 48.Djousse L, Levy D, Benjamin EJ, Blease SJ, Russ A, Larson MG, Massaro JM, D’Agostino RB, Wolf PA, Ellison RC. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am J Cardiol. 2004;93:710–713. doi: 10.1016/j.amjcard.2003.12.004. [DOI] [PubMed] [Google Scholar]
- 49.Mitchell GF, Vasan RS, Keyes MJ, et al. Pulse pressure and risk of new onset atrial fibrillation. JAMA. 2007;297:709–715. doi: 10.1001/jama.297.7.709. [DOI] [PubMed] [Google Scholar]
- 50.White PD, Aub JC. The electrocardiogram in thyroid disease. Arch Intern Med. 1918;22:766–769. [Google Scholar]
- 51.Sandler G, Wilson GM. The nature and prognosis of heart disease in thyrotoxicosis: a review of 150 patients with 131 I. Q J Med. 1959;52:347–369. [PubMed] [Google Scholar]
- 52.Peterson P, Hansen JM. Stroke in thyrotoxicosis with atrial fibrillation. Stroke. 1988;19:15–18. doi: 10.1161/01.str.19.1.15. [DOI] [PubMed] [Google Scholar]
- 53.Nordyke RA, Gilbert FI, Harada As. Graves”disease: influence of age on clinical findings. Arch intern Med. 1988;148:626–631. doi: 10.1001/archinte.148.3.626. [DOI] [PubMed] [Google Scholar]
- 54.Presti CF, Hart RG. Thyrotoxicosis, atrial dfibrillation and embolism revisted. Am Heart J. 1989;117:976–977. doi: 10.1016/0002-8703(89)90642-x. [DOI] [PubMed] [Google Scholar]
- 55.Singer DE. Randomized trials of warfarin for atrial fibrillation. N Engl J Med. 1992;327:1451–1453. doi: 10.1056/NEJM199211123272009. [DOI] [PubMed] [Google Scholar]
- 56.Tenerz A, Forberg R, Jansson R. Is a more acive attitude warranted in patients with subclinical thyrotoxicosis? J Intern med. 1990;228:229–233. doi: 10.1111/j.1365-2796.1990.tb00223.x. [DOI] [PubMed] [Google Scholar]
- 57.Sawin CT, Geller A, Wolf PA, et al. Low serum thyrotropin concentrations as a risk factor for atrail fibrillation in older persons. N Engl J Med. 1994;331:1249–1252. doi: 10.1056/NEJM199411103311901. [DOI] [PubMed] [Google Scholar]
- 58.Cappola AR, Fried LP, Arnold AM, et al. Thyroid status, cardiovascular risk and mortality in older adults. JAMA. 2006;295:1033–1041. doi: 10.1001/jama.295.9.1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Vaziri SM, Larson MG, Benjamin EJ, et al. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation. 1994;89:724–730. doi: 10.1161/01.cir.89.2.724. [DOI] [PubMed] [Google Scholar]
- 60.Fox CS, Parise H, Vasan R, et al. Mitral annular calcification is a predictor for incident atrial fibrillation. Atherosclerosis. 2004;173:291–294. doi: 10.1016/j.atherosclerosis.2003.12.018. [DOI] [PubMed] [Google Scholar]
- 61.Okin PM, Wachtell K, Devereux RB, et al. Regression of electrocardiographic left ventricular hypertrophy and decreased incidence of new-onset atrial fibrillation in patients with hypertension. JAMA. 2006;296:1242–1248. doi: 10.1001/jama.296.10.1242. [DOI] [PubMed] [Google Scholar]
- 62.Falk RH. Atrial fibrillation. N Engl J Med. 2001;344:1067–1078. doi: 10.1056/NEJM200104053441407. [DOI] [PubMed] [Google Scholar]
- 63.Bruins P, Velthuis H, Yazdanbakhsh AP, et al. Activation of the complement system during and after cardiopulmonary bypass surgery: postsurgery activation involves C-reactive protein and is associated with postoperative arrhythmia. Circulation. 1997;96:3542–3548. doi: 10.1161/01.cir.96.10.3542. [DOI] [PubMed] [Google Scholar]
- 64.Boss Christopher J, Lip Gregory YH. The Role of Inflammation in Atrial Fibrillation. Int J Clin Pract. 2005;59(8):870–872. doi: 10.1111/j.1368-5031.2005.0599b.x. [DOI] [PubMed] [Google Scholar]
- 66.Chung MK, Martin DO, Sprecher D, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. 2001;104:2886–2891. doi: 10.1161/hc4901.101760. [DOI] [PubMed] [Google Scholar]
- 67.Aviles RJ, Martin DO. Inflammation as a Risk Factor for Atrial Fibrillation. Circulation. 2003;108:3006. doi: 10.1161/01.CIR.0000103131.70301.4F. [DOI] [PubMed] [Google Scholar]
- 68.Zacharias A, Schwann TA, Riordan CJ, et al. Obesity and risk of new-onset atrial fibrillation after cardiac surgery. Circulation. 2005;112:3247. doi: 10.1161/CIRCULATIONAHA.105.553743. [DOI] [PubMed] [Google Scholar]
- 69.Dublin S, French B, Glazer NL, et al. Risk of new-onset atrial fibrillation in relation to body mass index. Arch Intern Med. 2006;166:2322–2328. doi: 10.1001/archinte.166.21.2322. [DOI] [PubMed] [Google Scholar]
- 70.Wang TJ, Parise H, Levy D, et al. Obesity and the risk of new onset atrial fibrillation. Am J Med. 1995 May;98(5):476–84. [Google Scholar]
- 71.Umetani K, Kodama Y, Nakamura T, et al. High Prevalence of Paroxysmal Atrial Fibrillation and/or Atrial Flutter in Metabolic Syndrome. Circ J. 2007;71:252. doi: 10.1253/circj.71.252. [DOI] [PubMed] [Google Scholar]
- 72.Merlo Östgren CJ, Råstam L, Lindblad U for Skaraborg Hypertension and Diabetes Project. Atrial fibrillation and its association with type 2 diabetes and hypertension in a Swedish community. Diabetes, Obesity and Metabolism. 2004;6:367–374. doi: 10.1111/j.1462-8902.2004.00358.x. [DOI] [PubMed] [Google Scholar]
- 73.Ujino K, Miyasaka Y, Barnes ME, et al. Obesity: an independent predictor of diastolic dysfunction in men and women aged 65 years and older. J Am Soc Echocardiogr. 2003;16:560. [Google Scholar]
- 74.Hanna IR*, Heeke B, Bush H. The Relationship Between Stature and the Prevalence of Atrial Fibrillation in Patients With Left Ventricular Dysfunction. J Am Coll Cardiol. 2006;47:1683–8. doi: 10.1016/j.jacc.2005.11.068. © 2006. [DOI] [PubMed] [Google Scholar]
- 75.Wang TJ, Larson MG, Levy D, et al. Plasma Natriuretic Peptide Levels and the Risk of Cardiovascular Events and Death. N Engl J Med. 2004;350:655–663. doi: 10.1056/NEJMoa031994. [DOI] [PubMed] [Google Scholar]
- 76.Kanagala R, Murali NS, Friedman PA, et al. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation. 2003;107:2589–2594. doi: 10.1161/01.CIR.0000068337.25994.21. [DOI] [PubMed] [Google Scholar]
- 77.Gami AS, Pressman G, Caples SM, et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110:364–367. doi: 10.1161/01.CIR.0000136587.68725.8E. [DOI] [PubMed] [Google Scholar]
- 78.Shamsuzzaman AS, Gersh BJ, Somers VK. Obstructive sleep apnea: implications for cardiac and vascular disease. JAMA. 2003;290:1906–1914. doi: 10.1001/jama.290.14.1906. [DOI] [PubMed] [Google Scholar]
- 79.Krieger J, Laks L, Wilcox I, et al. Atrial natriuretic peptide release during sleep in patients with obstructivesleep apnea before and after treatment with nasal continuous positive airway pressure. Clin Sci. 1989;77:407–11. doi: 10.1042/cs0770407. [DOI] [PubMed] [Google Scholar]
- 80.Redfield MM, Jacobsen SJ, Burnett JC, Jr, et al. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. doi: 10.1001/jama.289.2.194. [DOI] [PubMed] [Google Scholar]
- 81.Tsang TS, Gersh BJ, Appleton CP. Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J Am Coll Cardiol. 2002;40:1636–1644. doi: 10.1016/s0735-1097(02)02373-2. [DOI] [PubMed] [Google Scholar]
- 82.Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study. Circulation. 1995;92:835–841. doi: 10.1161/01.cir.92.4.835. [DOI] [PubMed] [Google Scholar]
- 83.Douglas P. The left atrium: a biomarker of chronic diastolic dysfunction and cardiovascular disease risk. J Am Coll Cardiol. 2003;42:1206–1207. doi: 10.1016/s0735-1097(03)00956-2. [DOI] [PubMed] [Google Scholar]
- 84.Gersh BJ, Tsang TSM, Barnes ME, et al. The changing epidemiology of non-valvular atrial fibrillation: the role of novel risk factors. European Heart Journal Supplements. 2005;7:C5–C11. [Google Scholar]
- 85.Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized, controlled trials. Arch Intern Med. 1994;154:1449–1457. [PubMed] [Google Scholar]
- 86.Krahn AD, Manfreda J, Tate RB, Mathewson FAL, Cuddy TE. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba follow-up study. JAMA. 1994;98:476–84. doi: 10.1016/S0002-9343(99)80348-9. [DOI] [PubMed] [Google Scholar]
- 87.Kanter MC, Tegeler CH, Pearce LA, et al. Carotid stenosis in patients with atrial fibrillation. Prevalence, risk factors, and relationship to stroke in the Stroke Prevention in Atrial Fibrillation Study. Arch Intern Med. 1994;154:1372–7. [PubMed] [Google Scholar]
- 88.Hart RG, Halperin JL. Atrial fibrillation and stroke: concepts and controversies. Stroke. 2001;32:803–8. doi: 10.1161/01.str.32.3.803. [DOI] [PubMed] [Google Scholar]
- 89.Fox CS, Parise H, D’Agostino RB, Sr, et al. Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring. JAMA. 2004;291:2851–2855. doi: 10.1001/jama.291.23.2851. [DOI] [PubMed] [Google Scholar]
- 90.Darbar D, Herron KJ, Ballew JD, et al. Familial atrial fibrillation is a genetically heterogeneous disorder. J Am Coll Cardiol. 2003;41:2185–2192. doi: 10.1016/s0735-1097(03)00465-0. [DOI] [PubMed] [Google Scholar]
- 91.Mestroni L. Genomic medicine in atrial fibrillation. J Am Coll Cardiol. 2003;41:2193–2121. doi: 10.1016/s0735-1097(03)00459-5. [DOI] [PubMed] [Google Scholar]
- 92.Crenshaw BS, Ward SR, Granger CB, et al. Atrial fibrillation in the setting of acute myocardial infarction: the GUSTO-I experience. J Am Coll Cardiol. 1997;30:406–13. doi: 10.1016/s0735-1097(97)00194-0. [DOI] [PubMed] [Google Scholar]
- 93.Chen YH, Xu SJ, Bendahhou S. KCNQ1 gain-of-function mutation in familial atrial fibrillation. Science. 2003;299:251–254. doi: 10.1126/science.1077771. [DOI] [PubMed] [Google Scholar]
- 94.Wang TJ, Massaro JM, Levy D, et al. A risk score for predicting stroke or death in individuals with new onset atrial fibrillation in the community. The Frmingham Heart Study. JAMA. 2003;290:1049. doi: 10.1001/jama.290.8.1049. [DOI] [PubMed] [Google Scholar]
- 95.Vermes E, Tardif JC, Bourassa MG. Enalapril decreases the incidence of atrial fibrillation in patients with left ventricular dysfunction: insight from the Studies of Left Ventricular Dysfunction (SOLVD) Trials. Circulation. 2003;107:2926–2931. doi: 10.1161/01.CIR.0000072793.81076.D4. [DOI] [PubMed] [Google Scholar]
- 96.Klein HU, Goette A. Blockade of atrial angiotensin II type 1 receptors: a novel antiarrhythmic strategy to prevent atrial fibrillation? J Am Coll Cardiol. 2003;41:2205–2206. doi: 10.1016/s0735-1097(03)00469-8. [DOI] [PubMed] [Google Scholar]
- 97.Rowan SB, Bailey DN, Bublitz CE, Anderson RJ. Trends in anticoagulation for atrial fibrillation in the U.S.: an analysis of the national ambulatory medical care survey database. J Am Coll Cardiol. 2007;49:1561–1565. doi: 10.1016/j.jacc.2006.11.045. [DOI] [PubMed] [Google Scholar]