

Abstract
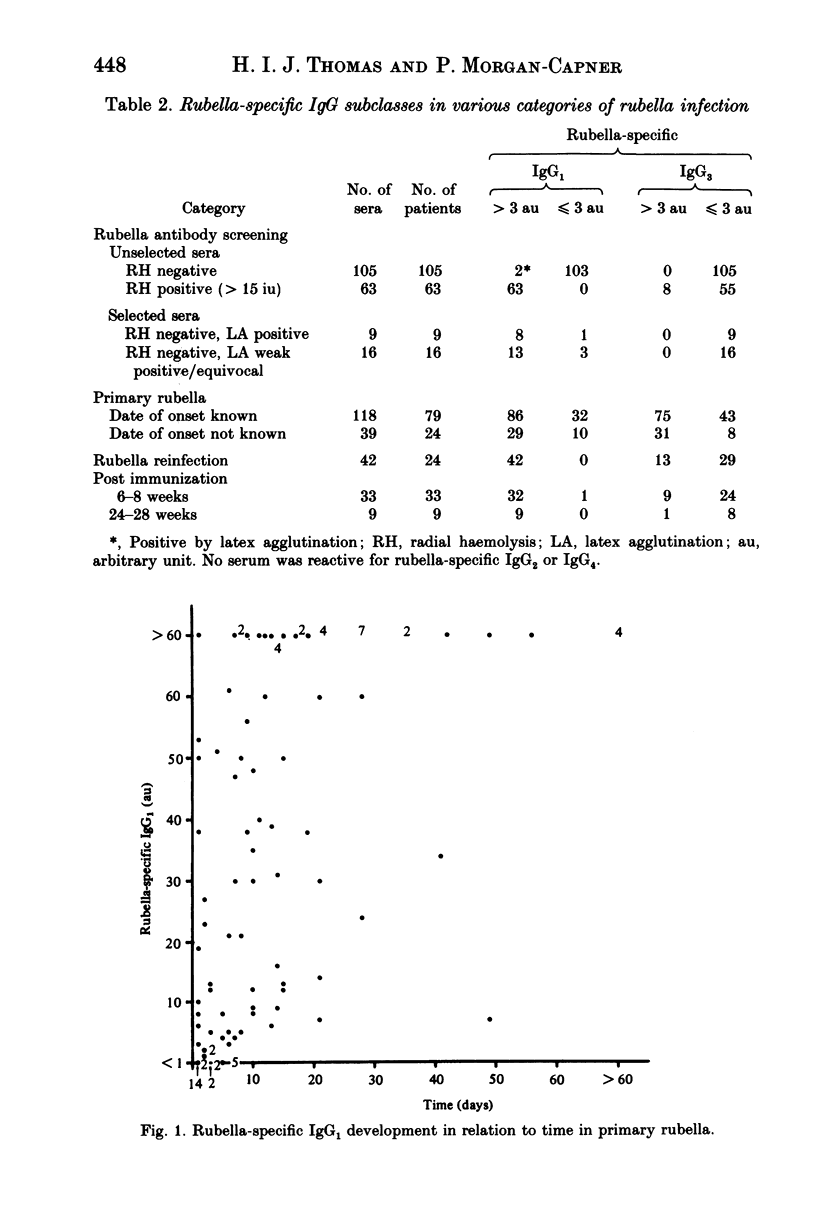
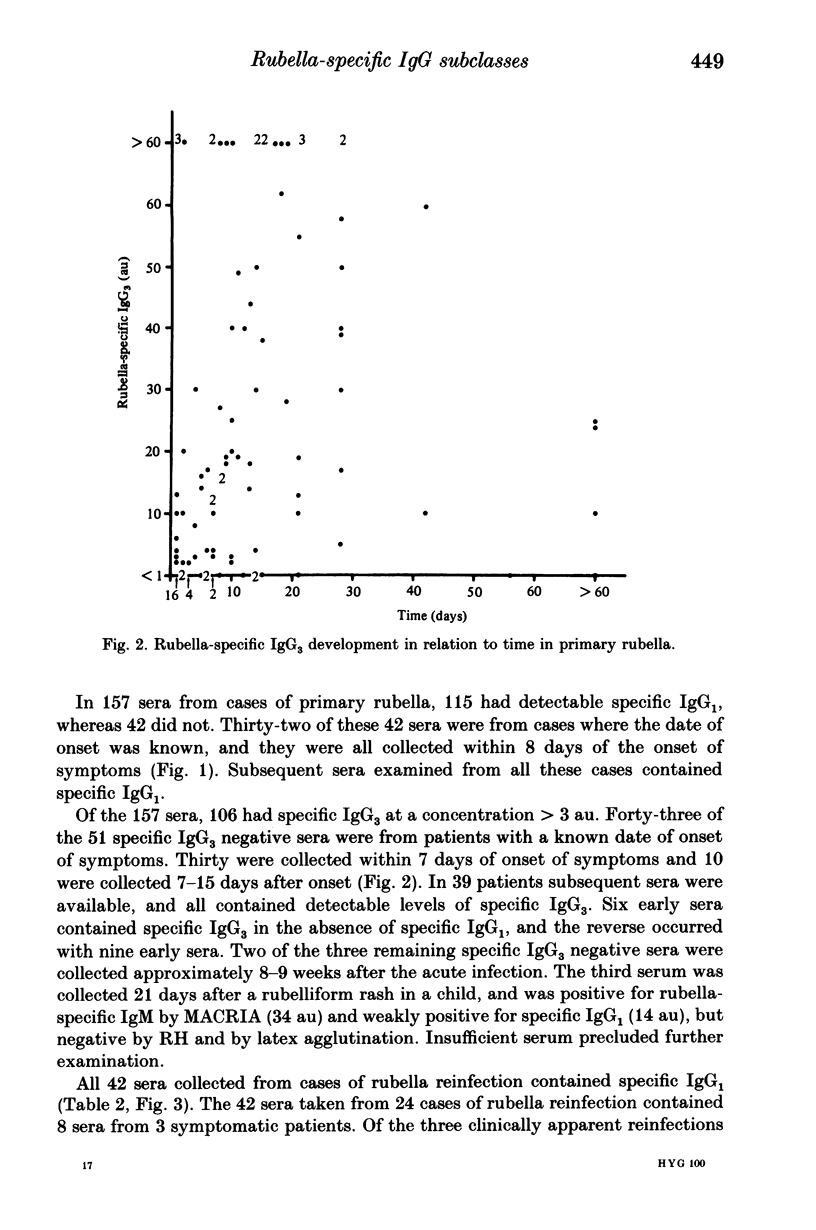
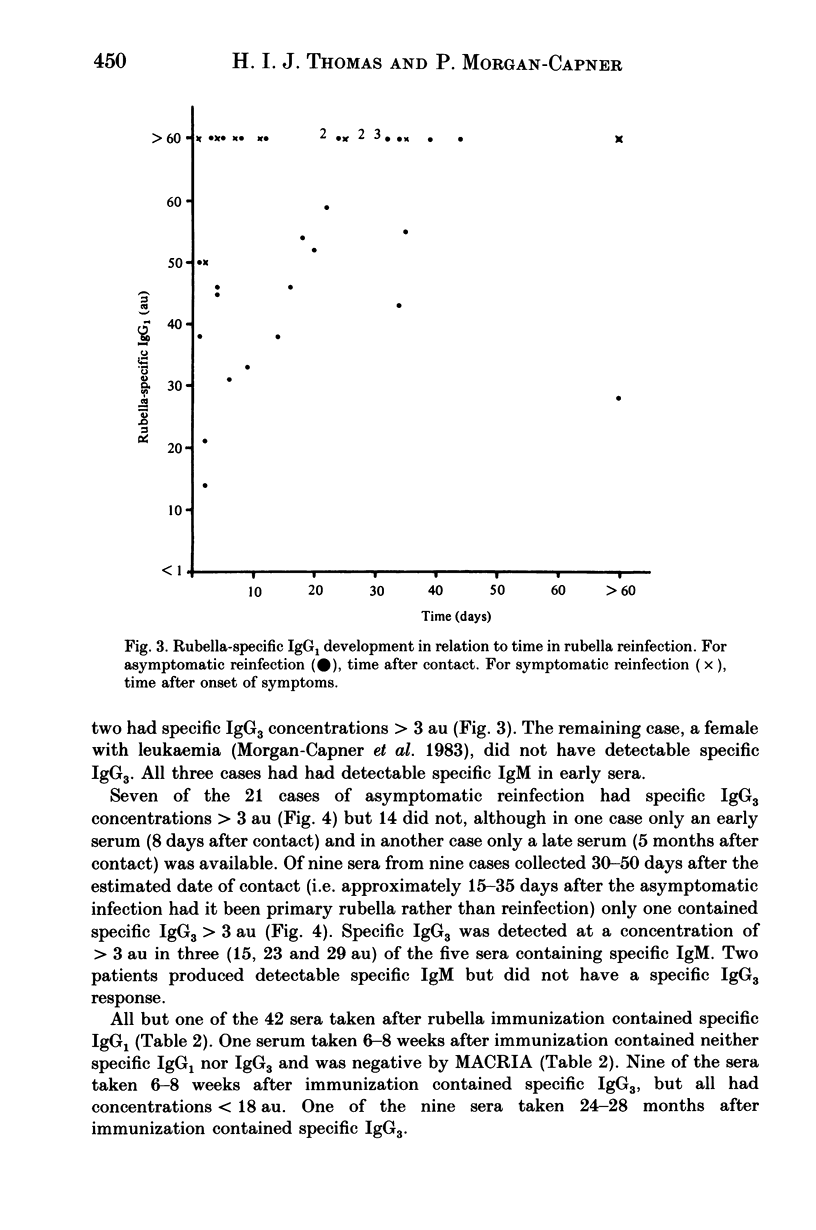
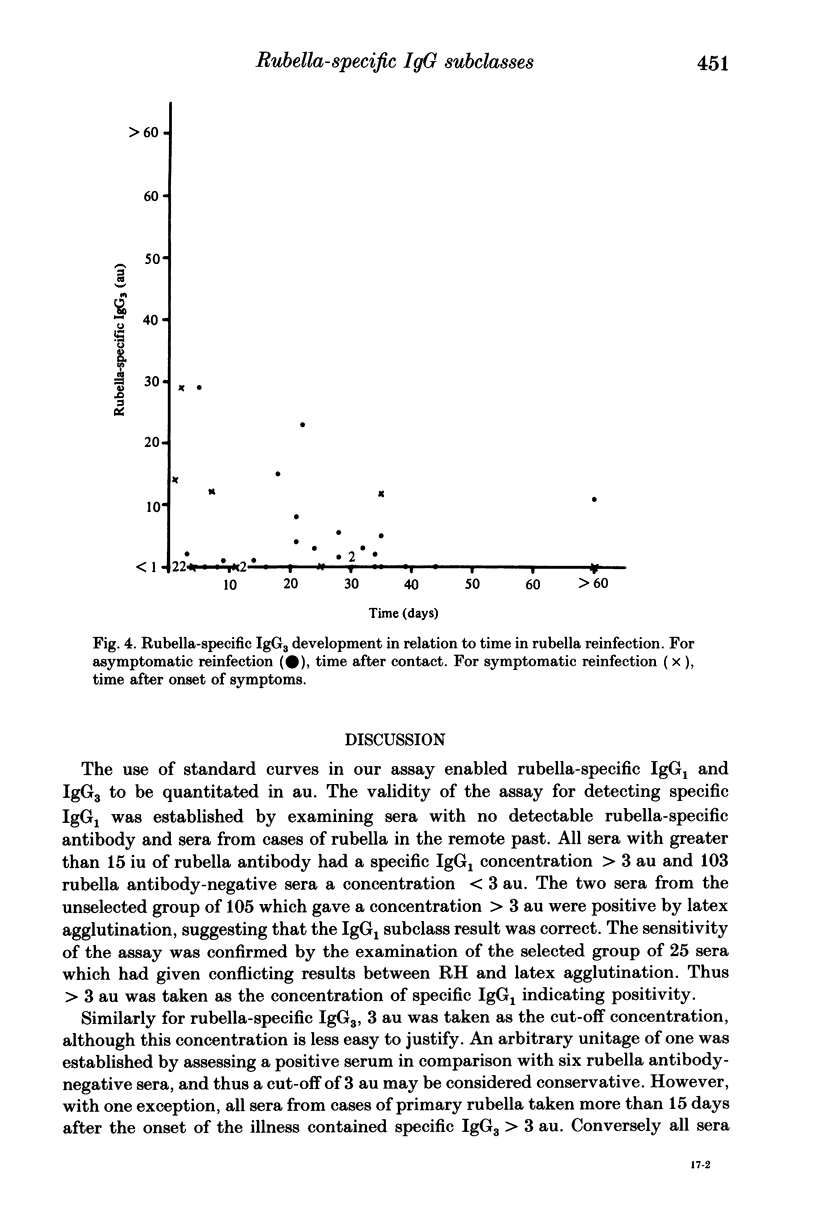
A solid-phase antigen enzyme-linked immunosorbent assay (ELISA) was developed for the detection of rubella-specific IgG subclasses. For rubella-specific IgG1 and IgG3 sera were quantitated in arbitrary units (au) by comparison with standard curves. A concentration of 3 au was taken as that indicating positivity for specific IgG1 and specific IgG3. No sera reactive for specific IgG2 and IgG4 have been found, and thus the assay reagents were controlled by testing dilutions of a standard calibrant serum containing known concentrations of the specific IgG subclasses. Of 105 unselected sera negative for rubella antibody by radial haemolysis (RH), two gave concentrations of specific IgG1 greater than 3 au and both were positive by rubella latex agglutination (LA). The sensitivity of the assay for specific IgG1 was confirmed by examining 25 selected sera negative by RH but reactive by LA. Twenty-one gave concentrations greater than 3 au. None of these 130 was positive for specific IgG3. All 63 sera containing greater than 15 international units rubella antibody by RH from cases of rubella in the remote past contained specific IgG1 and eight contained specific IgG3. In 79 cases of primary rubella, specific IgG1 developed in all cases by day 8. Specific IgG3 became detectable in all cases except one by day 16. Serum taken on day 21 from one case was negative for specific IgG3 but the absence of later sera precluded further investigation. One case had become negative for specific IgG3 by day 56. Sera from 24 cases of rubella reinfection were examined and all contained specific IgG1. In three cases of symptomatic reinfection, specific IgG3 was detectable in two but not in the remaining case. In 2 of the 21 cases of asymptomatic reinfection only a very early or a very late serum was available. Of the remaining 19 cases, 7 had detectable specific IgG3. However, only one of 9 sera collected 30-50 days after contact contained specific IgG3. Thus for the asymptomatic patient for whom other serological tests suggest a recent rubella infection, the failure to detect specific IgG3 in sequential sera collected after contact suggests reinfection rather than primary rubella. The detection of specific IgG3 did not correlate with the presence of specific IgM. Sera collected 6-8 weeks after rubella vaccination had detectable specific IgG1 in 32 of 33 cases and specific IgG3 in 9 of 33. The remaining vaccinee was seronegative.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cradock-Watson J. E., Ridehalgh M. K., Anderson M. J., Pattison J. R. Outcome of asymptomatic infection with rubella virus during pregnancy. J Hyg (Lond) 1981 Oct;87(2):147–154. doi: 10.1017/s0022172400069345. [DOI] [PMC free article] [PubMed] [Google Scholar]
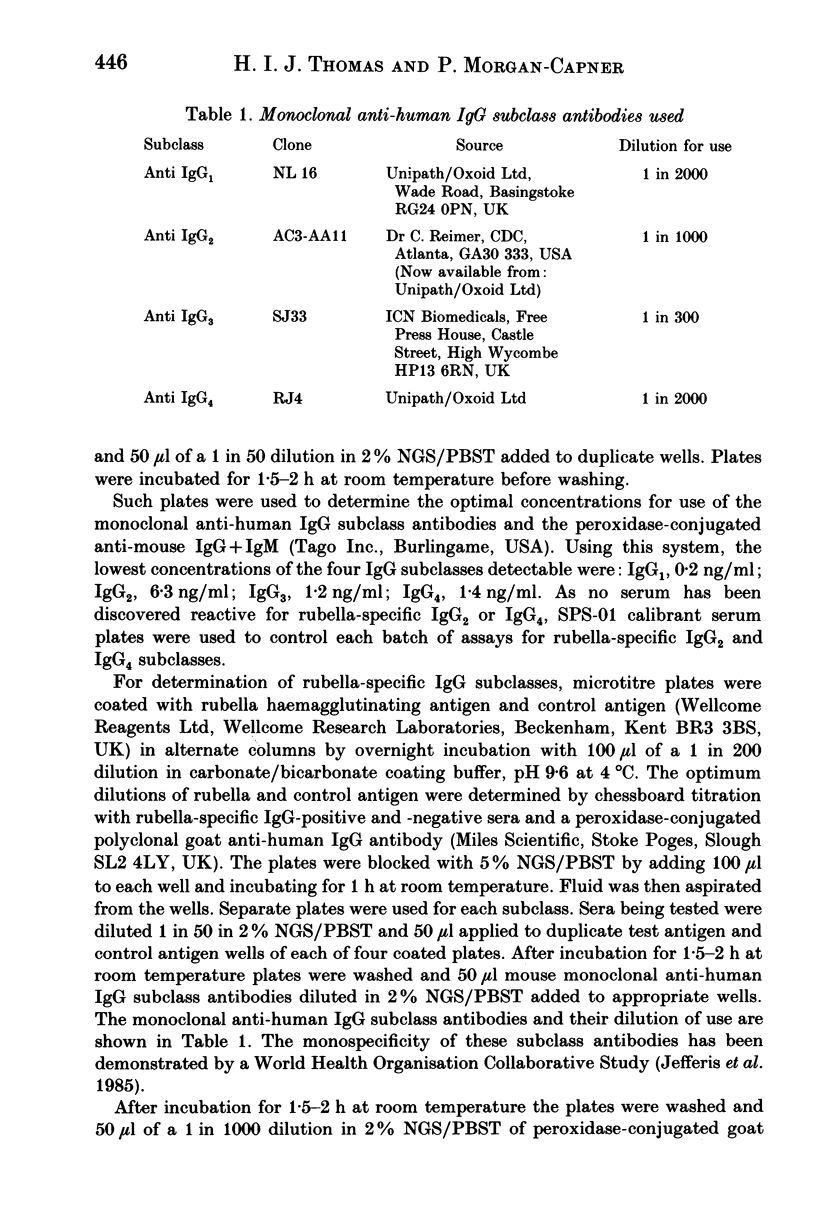
- Jefferis R., Reimer C. B., Skvaril F., de Lange G., Ling N. R., Lowe J., Walker M. R., Phillips D. J., Aloisio C. H., Wells T. W. Evaluation of monoclonal antibodies having specificity for human IgG sub-classes: results of an IUIS/WHO collaborative study. Immunol Lett. 1985;10(3-4):223–252. doi: 10.1016/0165-2478(85)90082-3. [DOI] [PubMed] [Google Scholar]
- Kurtz J. B., Mortimer P. P., Mortimer P. R., Morgan-Capner P., Shafi M. S., White G. B. Rubella antibody measured by radial haemolysis. Characteristics and performance of a simple screening method for use in diagnostic laboratories. J Hyg (Lond) 1980 Apr;84(2):213–222. doi: 10.1017/s0022172400026711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehtinen M. Affinity and sub-class distribution of IgG-class antibodies following vaccination with a live rubella virus vaccine. Vaccine. 1987 Jun;5(2):88–89. doi: 10.1016/0264-410x(87)90052-1. [DOI] [PubMed] [Google Scholar]
- Linde G. A. Subclass distribution of rubella virus-specific immunoglobulin G. J Clin Microbiol. 1985 Jan;21(1):117–121. doi: 10.1128/jcm.21.1.117-121.1985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller E., Cradock-Watson J. E., Pollock T. M. Consequences of confirmed maternal rubella at successive stages of pregnancy. Lancet. 1982 Oct 9;2(8302):781–784. doi: 10.1016/s0140-6736(82)92677-0. [DOI] [PubMed] [Google Scholar]
- Morgan-Capner P., Burgess C., Ireland R. M., Sharp J. C. Clinically apparent rubella reinfection with a detectable rubella specific IgM response. Br Med J (Clin Res Ed) 1983 May 21;286(6378):1616–1616. doi: 10.1136/bmj.286.6378.1616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan-Capner P., Hodgson J., Hambling M. H., Dulake C., Coleman T. J., Boswell P. A., Watkins R. P., Booth J., Stern H., Best J. M. Detection of rubella-specific IgM in subclinical rubella reinfection in pregnancy. Lancet. 1985 Feb 2;1(8423):244–246. doi: 10.1016/s0140-6736(85)91027-x. [DOI] [PubMed] [Google Scholar]
- Morgan-Capner P., Hodgson J., Sellwood J., Tippett J. Clinically apparent rubella reinfection. J Infect. 1984 Jul;9(1):97–100. doi: 10.1016/s0163-4453(84)94706-6. [DOI] [PubMed] [Google Scholar]
- Mortimer P. P., Edwards J. M., Porter A. D., Tedder R. S., Mace J. E., Hutchinson A. Are many women immunized against rubella unnecessarily? J Hyg (Lond) 1981 Aug;87(1):131–138. doi: 10.1017/s0022172400069308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mortimer P. P., Tedder R. S., Hamblig M. H., Shafi M. S., Burkhardt F., Schilt U. Antibody capture radioimmunoassay for anti-rubella IgM. J Hyg (Lond) 1981 Apr;86(2):139–153. doi: 10.1017/s0022172400068856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sarnesto A., Ranta S., Vänänen P., Mäkelä O. Proportions of Ig classes and subclasses in rubella antibodies. Scand J Immunol. 1985 Mar;21(3):275–282. doi: 10.1111/j.1365-3083.1985.tb01430.x. [DOI] [PubMed] [Google Scholar]
- Skvaril F., Schilt U. Characterization of the subclasses and light chain types of IgG antibodies to rubella. Clin Exp Immunol. 1984 Mar;55(3):671–676. [PMC free article] [PubMed] [Google Scholar]
- Stokes A., Mims C. A., Grahame R. Subclass distribution of IgG and IgA responses to rubella virus in man. J Med Microbiol. 1986 Jun;21(4):283–285. doi: 10.1099/00222615-21-4-283. [DOI] [PubMed] [Google Scholar]