

Abstract
Transthoracic echocardiography is a primary non-invasive modality for investigation of heart transplant recipients. It is a versatile tool which provides comprehensive information about cardiac structure and function. Echocardiographic examinations can be easily performed at the bedside and serially repeated without any patient's discomfort. This review highlights the usefulness of Doppler echocardiography in the assessment of left ventricular and right ventricular systolic and diastolic function, of left ventricular mass, valvular heart disease, pulmonary arterial hypertension and pericardial effusion in heart transplant recipients. The main experiences performed by either standard Doppler echocardiography and new high-tech ultrasound technologies are summarised, pointing out advantages and limitations of the described techniques in diagnosing acute allograft rejection and cardiac graft vasculopathy. Despite the sustained efforts of echocardiographic technique in predicting the biopsy state, endocardial myocardial biopsies are still regarded as the gold standard for detection of acute allograft rejection. Conversely, stress echocardiography is able to identify accurately cardiac graft vasculopathy and has a recognised prognostic in this clinical setting. A normal stress-echo justifies postponement of invasive studies. Another use of transthoracic echocardiography is the monitorisation and the visualisation of the catheter during the performance of endomyocardial biopsy. Bedside stress echocardiography is even useful to select appropriately heart donors with brain death. The ultrasound monitoring is simple and effective for monitoring a safe performance of biopsy procedures.
Background
Over the past decade heart transplantation (HT) has evolved from a rarely performed procedure to an accepted therapy for advanced heart failure. About 45% of the candidates to HT have ischemic cardiomyopathy while 55% have some form of dilated cardiomyopathy of various origin. The prognosis for HT patients following the orthotopic procedure has greatly improved over the past 20 years, and a recent report (August 2006) of Heart Transplants: Statistics of American Heart Association. informs that the 5 years survival rates is 66.9% in women and 71.2% in men. Although significant advances have been reached in surgical techniques, in donor and recipient selection criteria, and also in the management of transplant patients, allograft rejection remains the most important cause of morbidity and. the primary limitation for the survival of these patients.
Acute allograft rejection (AAR) is frequent in the first months after HT. Because it is initially asymptomatic, regular rejection surveillance is obligatory by monitoring immunosuppressive treatment, clinical and laboratory data and, in particular, by performing endomyocardial biopsies (EMBs), which represent the gold standard for the detection of rejection. AAR is characterised histologically by inflammatory cell infiltrates, interstitial edema and myocite necrosis which ultimately translates into structural and functional abnormalities of the allograft. A first international grading system for cardiac allograft biopsies, adopted in 1990 by the International Society for Heart Transplantation [1], has been updated in 2004 by the International Society for Heart and Lung Transplantation (ISHLT) (Table 1) [2].
Table 1.
Grading of rejection of endomyocardial biopsy according to International Society of Heart and Lung Transplantation (update 2004)
| Grade | Signs of rejection |
| Grade 0 R | No acute cellular rejection |
| Grade 1 R | Mild, low-grade, acute cellular rejection |
| Grade 2 R | Moderate, intermediate-grade, acute cellular rejection |
| Grade 3 R | Severe, high-grade, acute cellular rejection |
Long-term survival of allografted hearts is limited by a progressive fibro-proliferative disease, resulting in intimal thickening and occlusion of the grafted coronary vessels. This disease, variously defined as accelerated transplant coronary artery disease (CAD) or cardiac graft vasculopathy (CAV), is also known as chronic allograft rejection [3]). After the first year transplant peripheral and cerebro-vascular disease, end-stage renal disease, malignancy and infections are the other main causes of death. Specific side-effects of the immunosuppressive agents like renal failure, arterial hypertension and diabetes mellitus shall be also taken into account.
The role of Doppler echocardiography in the transplanted heart
Echocardiography is particularly useful for the assessment of HT recipients since it is easily performable and not associated with the risks of the invasive procedures. Its versatility allows it to be applied in a wide variety of situations in the post-transplant setting.
The echocardiographic features of left and right atria
During HT procedure donor cardiectomy involves only partial atrial resection. With the standard surgical procedure (biatrial surgical approach) an anastomosis is made between the residual recipient atrial tissue and the donor atria such that there is a characteristic unique echocardiographic atrial morphological appearance. Therefore, transplanted hearts have increased size in both atria, primarily caused by an increase in their long-axis dimension. Sometimes, an echo dense ridge is also visualisable at mid-atrial level (best appreciated in apical 4-chamber view), it being the site of anastomosis between the residual recipient atrial tissue and the donor atria [4] (Figure 1). The standard surgical technique has been reported to contribute to sub-optimal hemodynamics, specifically abnormal patterns of LV filling and to predispose to atrial thrombus formation, due to blood stasis in the dilated atrial cavities [5]. It is not unexpected, therefore, that post-HT echocardiographically determined left atrial area is inversely correlated with patient's survival [4]. The bicaval operative technique, introduced in the last decade, is associated with better preservation of atrial morphology [6] and lower risk for development of atrial thrombus [7].
Figure 1.
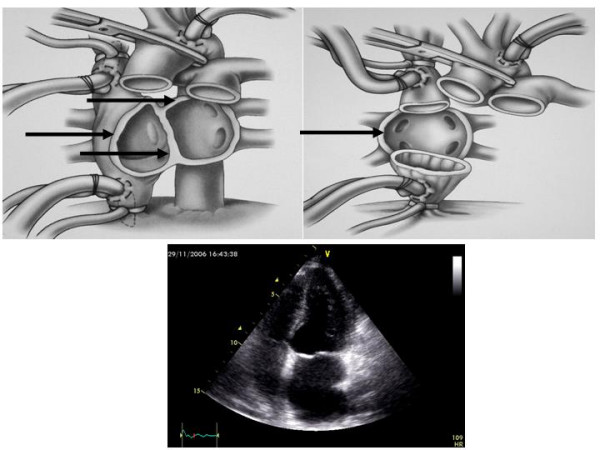
In the upper left panel a pericardial view (frontal) showing the edge of both atria which are preserved for conventional surgical technique (Shumway technique): possibility of interatrial ridge are dependent of the redundancy of donor as well as recipient residual tissue (arrows). In the upper right panel pericardial view (frontal) showing how the edge of both atria are removed for bicaval surgical technique: possibility of interatrial ridge are dependent of the redundancy of recipient septal residual tissue only (arrow). In the lower panel 2-D echocardiographic apical 4-chamber view showing left atrial enlargement and point of suture of a transplanted heart. Mod from Heart Transplantation – Churcill Livingstone – James K. Kirklin et al. 2002.
Assessment of left ventricular systolic function
The normalisation of left ventricular (LV) systolic function (M-mode derived endocardial fractional shortening or 2-D ejection fraction [EF])) after successful HT is responsible for early improvement of symptoms and has a strong impact on prognosis. In AAR LV systolic function is rarely affected but an early alteration of fractional shortening predicts subsequent development of CAV [8]. On a cohort of 65 HT recipients, 10–15 years after surgery, LV chamber dimension were well maintained and mean EF was 63% [9]. LV systolic dysfunction late after HT is often due to the effects of CAV and is associated to a poor prognosis [10]. Worthy of note, pulsed Tissue Doppler derived myocardial systolic velocity (Sm) of ≤ 10 cm/s has been found to be associated with a 97.2% likelihood for transplant CAD whereas Sm values of > 11 cm/s exclude CAD with 90.2% probability [11].
Assessment of left ventricular diastolic function
Although early AAR can be often responsible for the development of LV restrictive pattern, the recent literature does not support the use of Doppler indices of LV diastolic function as markers of AAR [12]. Standard Doppler appears as a method with an excellent specificity but insufficient sensitivity and this is mainly due to the influence of recipient atrial contraction timing on early ventricular filling and to sinus tachycardia which induces a frequent overlapping between E and A velocities [13]. Preserving left atrial morphology by using surgical bicaval techniques permits the maintenance of normal ventricular filling dynamics [4]. Because of the relatively load independency of myocardial velocities demonstrated also in HT recipients [14], pulsed Tissue Doppler has been proposed for the evaluation of LV diastolic properties due to AAR [11,15,16]. In the experience of Dandel et al, the negative and positive predictive values for AAR and transplant CAD of Tissue Doppler derived myocardial early diastolic velocity (Em) appeared high enough (= 92–96%) to allow a reliable non-invasive monitoring, instead of routinely scheduled EMBs [11]. Another study, which used Am velocity, has reported less favourable data, with good sensitivity (= 82%) but low specificity (= 53%) in predicting significant AAR [17]. In 50 HT patients, assessed by either right-sided cardiac catheterisation and Doppler echocardiography (including pulsed Tissue Doppler of the mitral annulus) simultaneously, mean wedge pressure was related weakly to mitral inflow variables but strongly to E/Em [r = 0.80; wedge pressure = 2.6+1.46(E/Em)] [18] (Figure 3), an index validated also in the general clinical setting (19). Figure 2 shows a slightly abnormal E/Em ratio (= 9) in a transplanted patient (normal cut-off value < 8) [19].
Figure 3.
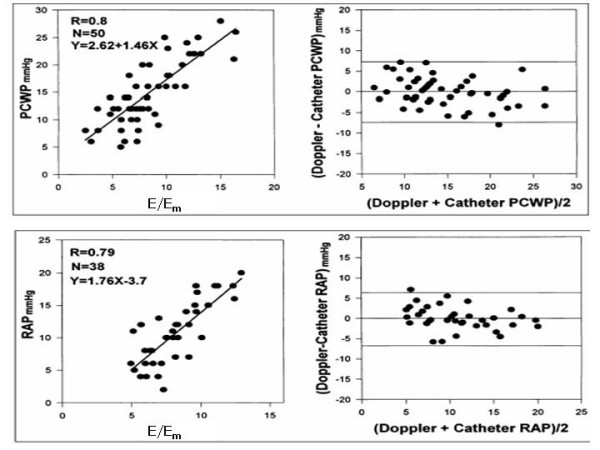
In the upper panel relation (left) and plot of Bland-Altman (right) between pulmonary capillary wedge pressure (PCWP) and mean mitral E/Ea ratio in transplant recipients. In the lower panel relation (left) and plot of Bland-Altman (right) between invasive mean right atrial pressure (RAP) and mean tricuspid E/Ea ratio in transplant recipients. (mod from Sudereswaran et al, Am J Cardiol 1998).
Figure 2.
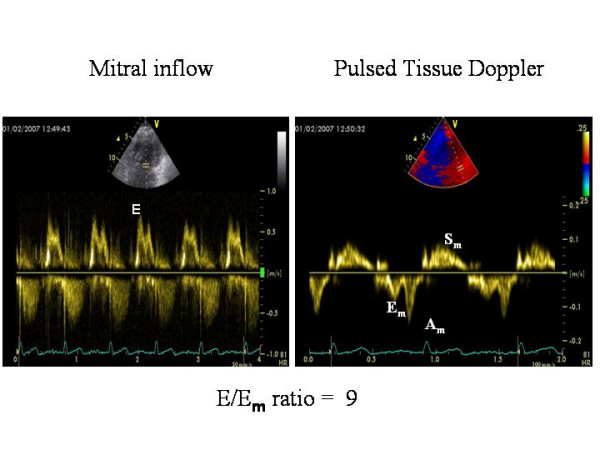
Standard Doppler derived transmitral inflow pattern (left panel) and Pulsed Tissue Doppler of the lateral mitral annulus in a HT recipient. The ratio is = .9.
Index of Myocardial Performance (IMP)
IMP is an index which combines LV systolic and diastolic parameters (= (IVRT + ICT/LVET, where IVRT = isovolumic relaxation time, ICT = Isovolumic contraction time and LVET = left ventricular ejection time) and gives information about LV global performance [20]. The rationale for using IMP in this setting is that, during AAR, LV diastolic dysfunction can be accompanied by subtle abnormalities of LV systolic performance and these are potentially reflected in changes of systolic time intervals. Accordingly, IMP has demonstrated to be sensitive to initial alterations of cardiac function in paediatric patients with AAR [21,22]. In 20 HT adult recipients with grade 3A cellular rejection, there was a mean increase of IMP by 98% (p < 0.0001) during the AAR episode and a decrease to its baseline values after treatment; in addition, the change in IMP was independent of both baseline EF and EF changes during AAR [23]. IMP could be, therefore, an useful non-invasive indicator, in order to assess the impact of therapy for amelioration of AAR. However, in another experience [24], the comparison of intra-recipient changes in Doppler intervals between rejection and non-rejection states demonstrated prolongation of IVRT and shortening of ICT during AAR, with no change in the IMP. It is possible that during AAR IVRT fall is counterbalanced by ICT prolongation and this may result in no significant change of IMP.
Left ventricular mass
After HT, it is evident an increase in wall thickness and LV mass, which can be detected and followed during time by serial echocardiographic examinations. LV hypertrophy is due to several causes (repetitive rejections, arterial hypertension, immunosuppressive therapy, chronic tachycardia and denervation) and its progression occurs mainly in relation to cyclosporine levels and blood pressure levels [25]. It is worthy of note that severe LV hypertrophy predicts mortality at 1-year follow-up in HT recipients [26].
Valvular heart disease
Valvular regurgitation is a fairly common occurrence immediately post HT but structural abnormalities of the aortic and mitral valves are not observed frequently after HT. In a long-term follow-up study, only 13 of 65 patients had mitral valve regurgitation (no patients had severe regurgitation), three cases of aortic valve regurgitation were reported and no patient has significant aortic valve stenosis [10]. Possible causes of mitral regurgitation include papillary muscle ischemia and the effect of multiple AAR episodes.
Tricuspid valve regurgitation
In contrast to the left-sided valves, tricuspid valve regurgitation is very common after HT, its etiology being multifactorial. When its appearance is early after HT, probably it is related to elevated pulmonary arterial pressures and vascular resistance in the recipient as well as to atrial structure and function (in patients who had undergone standard biatrial surgical approach). In the majority of the cases, the resolution of tricuspid regurgitation is possible within 1 month after HT, hand in hand with the normalisation of pulmonary arterial pressures [27]. Tricuspid regurgitation may be also due to injury of the chordal apparatus caused by the repeated EMBs. Biopsy-induced damage includes flail tricuspid leaflets and severe eccentric jets of regurgitations. A direct correlation between number of biopsies and severity of tricuspid regurgitation has been demonstrated: a number <31 EMBs significantly predicts a reduced risk of severe tricuspid regurgitation [28]. Regardless of cause, the persistence of tricuspid regurgitation is related to symptomatic right ventricular (RV) failure, impaired renal function and increased mortality [29].
The right ventricle
Because of the high prevalence of tricuspid valve regurgitation the assessment of RV systolic function is necessary in HT recipients. Although the majority of the cases of early RV dilation and associated hemodynamic change improve progressively in a matter of a week after HT [30], RV failure is a recognised cause of in-hospital death and some survivors have residual RV dilation. A relationship between the evidence of RV dysfunction and plasma B-type natriuretic peptide has also been observed [31]. In addition, even when RV systolic function appears normal, more subtle RV dysfunction can be unmasked by RV pulsed Tissue Doppler. In paediatric HT recipients, Sm velocity of the lateral tricuspid annulus has demonstrated to be lower than in controls, showing a trend to a further reduction during time [32]. In the experience of Suderaswaran et al, similar to LV filling pressure, mean right atrial pressure was related weakly to routine tricuspid inflow variables but strongly to tricuspid E/Em [r = 0.79; n = 38; right atrial pressure = 1.76(E/Em) - 3.7] after HT (18) (Figure 3). In addition, in 18 of these patients who repeated right-sided cardiac catheterizations during time, the changes in mean right atrial pressure were well detected by Doppler, with a mean difference of 0 ± 3.45 mm Hg (18). In this view, pulsed Tissue Doppler of the tricuspid annulus should be recommended in the follow-up of transplanted patients [33].
Pericardial effusion
Moderate to large pericardial effusions, due to a mismatch between recipient and donor hearts or to the presence of AAR or even to the effect of some immunosuppressive drugs, occurs frequently during the early phase after HT. However, the sensitivity (= 49%) and specificity (= 74%) for diagnosis of AAR are limited [34] The possibility of an infective cause for a pericardial effusion should always been taken into account in these patients who are often immuno-depressed. Close echocardiographic monitoring is required in order to avoid heart tamponade. Pericardial effusion is not associated, however, with any adverse clinical outcomes and progressively disappears. If a large pericardial effusion accumulates slowly it may be of a little hemodynamic impact [35,36].
Potential role of high-technology ultrasound tools
Integrated backscatter (IBS) appears able to identify AAR by the decrease of cyclic variation signal [37] and the increase of 2-D derived end-diastolic IBS signal of either posterior or septal wall [38]. The off-line analysis of colour Tissue Doppler and strain rate imaging (SRI), a tool which quantifies myocardial wall deformation and distinguishes "true" active myocardial contraction from passive wall motion [39], has been experimented in HT recipient. "Healthy" HT patients may have normal global systolic function but altered regional systolic deformation compared to normal hearts [40]. SRI might be, therefore, an additional tool for detecting = IB grade of AAR [41] and reduce the number of EMBs. Despite promising, however, high-tech ultrasound technologies have been applied only on small number of HT recipients and their confirmation in larger population samples is needed.
Acute allograft rejection
Several attempts have been performed during time to take advantage by M-mode and 2-D echocardiography to diagnose AAR. The main echocardiographic variables proposed for diagnosis of AAR include increased wall thickness and wall echogenity, pericardial effusion, LV diastolic dysfunction and regional/global LV systolic dysfunction [42]. Table 2 sumarises the sensitivity and specificity of Doppler echocardiography in the main studies performed [23,38,43-46]. In general, the results are not encouraging and, when an echocardiographic parameter appears appropriate, confirmatory results are lacking. Although in the absence of key specific echo abnormalities the probability of AAR is relatively low, no single echocardiographic variable alone may be used for accurate detection of AAR. Of interest, an experience of Picano et al [47] showed that histologically verified rejection is accompanied by normal global wall motion during stress-induced ECG ST-segment depression. This recalls the well known stress-echo response pattern of microvascular angina, characterized by normal epicardial coronary arteries and reduced coronary flow reserve (CFR), which can, indeed, acutely and transiently reduced by AAR [48]. Despite these evidences, Doppler echocardiography is not routinely used to diagnose AAR. It is expectable that the effect of bicaval procedure on Doppler, the development of new high-tech ultrasound technique and the use of transthoracic CFR could produce some effect of improvement in the ultrasound diagnostic accuracy of AAR in the future time.
Table 2.
Main studies evaluating the accuracy of standard Doppler echocardiography in detecting AAR
| Authors | N. of patients | Method/Parameter | Sensitivity | Specificity |
| Desruennes M, J Am Coll Cardiol 1988 | 55 | Standard Doppler, PHT decrease (20%) | 88% | 87% |
| Simmonds MB, Circulation 1992 | 30 | Standard Doppler, superior vena caval SFFV ≤ 17 cm/s | 100% | 80% |
| Morocutti G, J Heart Lung Transplant 1995 | 18 | Standard Doppler, PHT ≤ 55 ms PHT ≤ 60 ms |
69% 62% |
76% 83% |
| Mouly-Bandini A, Transpl Int 1996 | 23 | Standard Doppler, IVRT decrease ≥ 20% | 45% | - |
| Angermann GE, Circulation 1997 | 52 | M-mode and 2D parameters | 40–55% | 84–87% |
| Stengel SM, Heart 2001 | 141 | Pulsed Tissue Doppler. Am of mitral annulus < 8.7 cm/s | 82% | 53% |
| Vivekananthan K, Am J Cardiol 2002 | 20 | Standard Doppler, MPI | 90% | 90% |
| Sun JP, J Heart Lung Transplant 2005 | 223 183 |
Standard Doppler echo ≥ 2 among PE, IVRT > 90 ms, E/A > 1.7 post HT ≤ 6 months post HT > 6 months |
57% 60% |
54% 93% |
IVRT = isovolumic relaxation time, MPI = Myocardial performance index, PE = pericardial effusion, PHT = Mitral pressure half-time, SFFV = inferior vena caval systolic forward flow velocity.
Cardiac allograft vasculopathy
The development of progressive CAD in HT has been recognised increasingly as long-term recipient survival has improved. Because CAV remains the major cause of death during long-term follow-up, its diagnosis is very important. It is remained for years in the prevalent domain of invasive techniques. Serial coronary angiography permits the study of coronary arteries and also the visualisation of coronary arteries by intravascular ultrasound (IVUS), that represents the reference gold standard in this clinical setting. Rapidly progressive vasculopathy by IVUS, defined as an increase of ≥ 0.5 mm in intimal thickness within the first year after HT, is a powerful predictor of all-cause mortality, myocardial infarction and angiographic abnormalities [47]. However, an annual angiographic evaluation is difficult to perform and, with almost equal reliability when compared with IVUS, CAV can be identified combining information on donor age, 2-D echocardiographically determined wall motion score at rest and immuno-fluorescence staining against anti-thrombin III in EMBs late after HT [49]. In this view, coronary angiography should be limited to patients with a high probability score and not be used routinely for surveillance of CAV. Clinical manifestations of CAV are often silent because the lack of afferent sympathetic innervation of the transplanted heart. Moreover, exercise performance in HT recipients has a limited value since the donor heart is surgically denervated without afferent parasympathetic or sympathetic innervation. Abnormalities of the ventricular rate response include resting tachycardia (due to parasympathetic denervation), a slow heart rate during mild-moderate exercise, a more rapid response during more strenuous exercise, and a more prolonged time for the ventricular rate to return to baseline during recovery. The heart rate response during exercise and the diffuse nature of CAV coronary abnormalities limit the sensitivity of ECG effort tests to detect coronary artery vasculopathy. Pharmacological stress echocardiography, a tool prognostically validated in groups of patients at risk for coronary artery disease [50], is safe and well tolerated in HT recipients. A varieties of stressors (adrenergic agents, vasodilators, cold pressure test) are available but dobutamine is preferred [51-58], mainly because denervation of the transplanted heart increases the responsiveness to chronotropic stimulation [59]. Dobutamine stress echocardiography (DSE) identifies patients at risk for events and facilitates monitoring of CAV. A normal DSE predicts an uneventful clinical course and justifies postponement of invasive studies [53,54,56]. Its prognostic value is comparable to that of IVUS and angiography [57]. DSE has been successfully proposed in order to predict cardiac events in long-term follow-up (4 years) of HT recipients [58]. The use of atropine after dobutamine infusion is controversial since it is evident that the heart of recipients is completely denervated and there are conflicting evidence regarding parasympathetic re-innervation. However, it is recent the demonstration that the adjunctive use of atropine in HT patients during stress-echo aids in reaching 85% of maximum predicted heart rate [60]. Also dipyridamole stress echocardiography is able to identify patients with altered wall motion who need careful surveillance and probably an invasive assessment [61,62]. Although wall motion at rest and after dipyridamole administration and CAV are predictors for cardiac events, only a wall motion score index >1 after dipyridamole remains significant at multivariate analysis [63]. Adenosine has been used to evaluate TTE-derived coronary flow reserve of left anterior descending artery (CFR) in transplant recipient, it showing 82% sensitivity, 87% specificity and 85% accuracy for CAV detection (cut-off point value ≤ 2.7) [64]. A shorter diastolic flow velocity at rest (deceleration time of diastolic velocity of ≤ 840 ms: sensitivity = 86%, specificity = 75%, positive predictive value = 33%, negative predictive value = 97%, p = 0.002) and a reduction of CFR (cut-off point of CFR ≤ 2.6, sensitivity = 91%, specificity = 62%, positive predictive value = 32%, negative predictive value = 97%, p = 0.001) have demonstrated to be both reliable markers for CAV-related major cardiac adverse events [65]. Figure 4 shows an abnormal CFR in a HT recipient. Of interest, dipyridamole-derived CFR is related positively with Tissue Doppler derived Sm velocity and negatively with E/Em ratio in HT recipients: this findings indicates a possible association of impaired coronary microcirculation with both myocardial systolic dysfunction and increase of LV filling pressures in this clinical setting [66].
Figure 4.
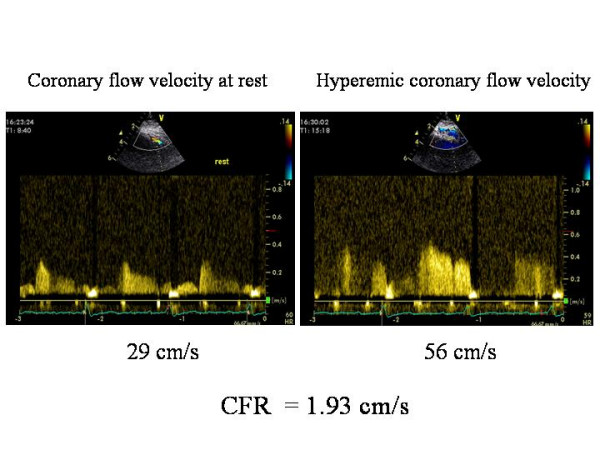
Reduced coronary flow reserve in a patient with coronary evidence of allograft vasculopathy.
Table 2 sumarises the main studies reporting sensitivity and specificity of pharmacological stress in detecting CAV and coronary artery stenosis > 50% in HT recipients (26). In general, stress echocardiography appears as a very important tool to identify CAV in HT recipients.
Echocardiography during endomyocardial byopsies
Another use of transthoracic echocardiography is the monitorisation and the visualisation of the catheter during the performance of endomyocardial biopsy [67]. The use of the ecocardiography is important to avoid an useless and dangerous exposition to X-ray and permits to follow adequately the movement of the catheter in the right ventricle and to select the site for biopsy (Figure 5). Echocardiography gives also the possibility to avoid damaging of tricuspid valve, papillary muscles or chords and to promptly identify the eventual presence of other complications like pericardial effusion. Real time 3-D echocardiography seems very promising in improving the ability to see the location of the bioptome during EMBs compared with 2-D echocardiography and fluoroscopy [68,69].
Figure 5.
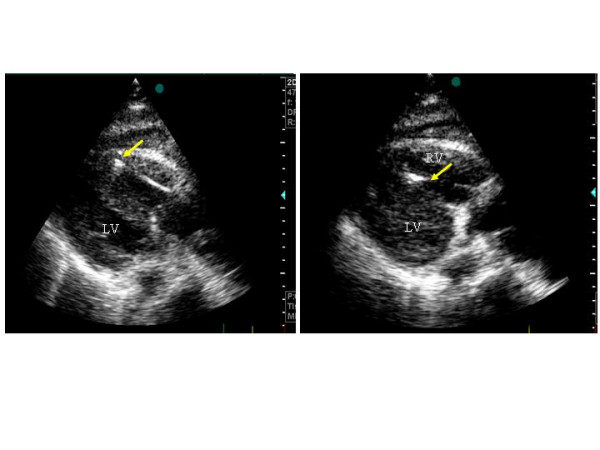
Use of 2-D echocardiography for monitoring the performance of endomyocardial biopsy in a HT recipient. The arrow indicates the site of the biopsy. Left panel: at the apex of right ventricle, right panel: al the level of the right side of the interventricular septum.
Heart donor storage
Heart donor storage is a main problem since patients in HT waiting list have a 7.3% death rate and the average waiting time is 2 to 3 years. In addition, there is a large amount of ''marginal'' recipients, it being due to either advanced age (> 65 years) or co-morbidity. Of consequence, a gradual trend toward liberalizing donor selection criteria has been developed and an expansion of the cardiac donor pool has involved accepting hearts of older donors, tolerating longer organ ischemic times and accepting hearts with structural and/or functional abnormalities, such as mild LV hypertrophy and mild valvular abnormalities [70-72]. In this view, although it is fair to recognize that transthoracic ultrasound imaging can be suboptimal in several patients on ventilators, the role of echocardiography has became crucial in order to detect adequate LV function and lack of significant valvular heart disease in the potential donors. Donors with echocardiographic functional abnormalities at the time of donation present an excellent 4 years survival rates [73]. The most important problem for an adequate selection is, however, the need of excluding donors with more than mild coronary artery disease. Coronary angiography is recommended for the majority of male donors older than 45 years and female donors older than 50 years, in order to exclude significant coronary artery stenosis. A simpler approach should be represented by bedside, pharmacological stress echocardiography, whose feasibility has been recently validated in potential heart donors with brain death: an aged donor with normal resting and stress echo, without regional wall motion abnormalities or with an hyperkinetic global response to the stress, can be judged as a good candidate for an uneventful HT [74]. The identification of hearts ''too good to die'' on the basis of bedside resting and stress echo can be a critical way to solve the mismatch between donor need and supply. Comparison between pre-transplant donor stress-echo and post-transplant recipient stress-echo could be performed to assess normal or abnormal function of the graft.
Table 3.
Main studies evaluating the accuracy of pharmacological stress echocardiography in detecting CAV and coronary artery stenosis > 50% in HT recipients (Mod from Thorn EM et al, Heart Fail Clin 2007)
| Authors | N. of pts | Time post-HT (years) | Sensitivity for CV | Specificity for CAV | Sensitivity for cor. stenosis | Sensitivity for cor. stenosis |
| Dobutamine | ||||||
| Akosah KO, 1994 | 41 | 4.8 (0.25–10) | 95% | 50% | 100% | 41% |
| Herregods, J Heart Lung Tr1994 | 28 | 3.2 ± 1.3 | 50% | 71% | - | - |
| Derumeaux G, JACC 1995 | 41 | 3.3 ± 1.7 | 86% | 91% | 100% | 77% |
| Derumeaux G, Arch Mal Coeur 1996 | 64 | 3.3 ± 1.2 | 85% | 97% | 100% | - |
| Akosah KO, JACC 1998 | 22 | 0.17 (0.04–0.3) | 100% | 73% | 100% | 59% |
| Derumeaux G, J Heart Lung Tr 1998 | 37 | 3.1 ± 1.7 4.7 ± 1.8 |
65% 92% |
95% 73% |
- - |
- - |
| Spes GH, Circulation 1999 | 109 | 3.2 ± 3.1 | 72% | 88% | - | - |
| Bacal F, J Heart Lung Tr 2004 | 38 | > 4 | - | - | 64% | 91% |
| Dipyridamole | ||||||
| Ciliberto GR, Eur Heart J 1993 | 80 | 2.3 ± 0.5 | 80% | 85% | 100% | 72% |
| Ciliberto GR. J Heart Lung Tr 2003 | 68 | 2.9 ± 1.9 | 80% | 79% | 100% | 87% |
| Adenosine | ||||||
| Tona F J Heart Lung Tr 2006 | 73 | 8.0 ± 4.5 | 82% | 87% | - | - |
CFR = Coronary flow reserve
Conclusion
Transthoracic Doppler echocardiography is a primary non-invasive modality for investigation of cardiac transplant recipients. It is a versatile tool which provides comprehensive information about cardiac structure and function. Echocardiographic examinations can be easily performed at the bedside and serially repeated without any patient's discomfort. Although sustained efforts to develop and echocardiographic technique able to predict the biopsy state have been performed, it has fair to recognise that EMBs are still regarded as the gold standard for detection of acute allograft rejection. Conversely, stress echocardiography is able to identify accurately CAV and has recognised prognostic value, which is comparable to that of IVUS or angiography. A normal stress-echo justifies postponement of invasive studies. Bedside stress echocardiography is even useful to select appropriately heart donors with brain death. Finally, echocardiographic monitoring is simple and effective for monitoring a safe performance of biopsy procedures.
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
SM conceived the study, participated in its design and drafted the manuscript, MM and MG reviewed the manuscript and participated in the design of the study, All the authors read and approved the final manuscript.
Contributor Information
Sergio Mondillo, Email: mondillo@unisi.it.
Massimo Maccherini, Email: maccherini2@unisi.it.
Maurizio Galderisi, Email: mgalderi@unina.it.
References
- Billingham ME, Cary NRB, Hammond EH, Kemnitz J, Marboe C, McCallister HA, Snovar DC, Winters GL, Zerbe A. A working formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection study group. J Heart Transplant. 1990;9:587–593. [PubMed] [Google Scholar]
- Stewart S, Winters GL, Fishbein MC, Tazelaar HD, Kobashigawa J, Abrams J, Andersen CB, Angelini A, Berry GJ, Burke MM, Demetris AJ, Hammond E, Itescu S, Marboe CC, McManus B, Reed EF, Reinsmoen NL, Rodriguez ER, Rose AG, Rose M, Suciu-Focia N, Zeevi A, Billingham ME. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant. 2005;24:1710–1720. doi: 10.1016/j.healun.2005.03.019. [DOI] [PubMed] [Google Scholar]
- Hornick P, Rose M. Chronic rejection in the heart. Methods Mol Biol. 2006;333:131–144. doi: 10.1385/1-59745-049-9:131. [DOI] [PubMed] [Google Scholar]
- Kirlin JK. Heart Transplantation. Churcill Livingstone edition; 2002. [Google Scholar]
- Peteiro J, Redondo F, Calviño R. Differences in heart transplant physiology according to surgical technique. J Thorac Cardiovasc Surg. 1996;112:584–589. doi: 10.1016/S0022-5223(96)70039-9. [DOI] [PubMed] [Google Scholar]
- El Gamel A, Yonan NA, Grant S. Orthotopic cardiac transplantation: a comparison of standard and bicaval Wythenshawe techniques. J Thorac Cardiovasc Surg. 1995;109:721–729. doi: 10.1016/S0022-5223(95)70354-3. [DOI] [PubMed] [Google Scholar]
- Riberi A, Ambrosi P, Habib G, Kreitmann B, Yao JG, Gaudart J, Ghez O, Metras D. Systemic embolism: a serious complication after cardiac transplantation avoidable by bicaval technique. Eur J Cardiothorac Surg. 2001;19:307–311. doi: 10.1016/S1010-7940(00)00653-9. [DOI] [PubMed] [Google Scholar]
- Kaye DM, Bergin P, Buckland M, Esmore D. Value of postoperative assessment of cardiac allograft function by transesophageal echocardiography. J Heart Lung Transplant. 1994;13:165–172. [PubMed] [Google Scholar]
- Bolad IA, Robinson DR, Webb C, Hamour I, Burke MM, Banner NR. Impaired left ventricular systolic function early after heart transplantation is associated with cardiac allograft vasculopathy. Am J Transplant. 2006;6:161–168. doi: 10.1111/j.1600-6143.2005.01138.x. [DOI] [PubMed] [Google Scholar]
- Wilhelmi M, Pethig K, Wilhelmi M, Nguyen H, Strüber M, Haverich A. Heart transplantation: echocardiographic assessment of morphology and function after more than 10 years of follow-up. Ann Thor Surg. 2002;74:1075–1079. doi: 10.1016/S0003-4975(02)03833-X. [DOI] [PubMed] [Google Scholar]
- Dandel M, Hummel M, Müller J, Wellnhofer E, Meyer R, Solowjowa N, Ewert R, Hetzer R. Reliability of tissue Doppler wall motion monitoring after heart transplantation for replacement of invasive routine screenings by optimally timed cardiac biopsies and catheterizations. Circulation. 2001;104:I184–I191. doi: 10.1161/hc37t1.094855. [DOI] [PubMed] [Google Scholar]
- Mena C, Wencker D, Krumholz HM, McNamara RL. Detection of heart transplant rejection in adults by echocardiographic diastolic indices: a systematic review of the literature. J Am Soc Echocardiogr. 2006;19:1295–300. doi: 10.1016/j.echo.2006.04.029. [DOI] [PubMed] [Google Scholar]
- Pellicelli AM, Cosial JB, Ferranti E, Gomez A, Borgia MC. Alteration of left ventricular filling evaluated by Doppler echocardiography as a potential marker of acute rejection in orthotopic heart transplant. Angiology. 1996;47:35–41. doi: 10.1177/000331979604700105. [DOI] [PubMed] [Google Scholar]
- Aranda JM, Jr, Weston MW, Puleo JA, Fontanet HL. Effect of loading conditions on myocardial relaxation velocities determined by Doppler tissue imaging in heart transplant recipients. J Heart Lung Transplant. 1998;17:693–697. [PubMed] [Google Scholar]
- Puleo JA, Aranda JM, Weston MW, Cintrón G, French M, Clark L, Fontanet HL. Noninvasive detection of allograft rejection in heart transplant recipients by use of Doppler tissue imaging. J Heart Lung Transplant. 1998;17:176–184. [PubMed] [Google Scholar]
- Fyfe DA, Ketchum D, Lewis R, Sabatier J, Kanter K, Mahle W, Vincent R. Tissue Doppler imaging detects severely abnormal myocardial velocities that identify children with pre-terminal cardiac graft failure after heart transplantation. J Heart Lung Transplant. 2006;25:510–517. doi: 10.1016/j.healun.2005.11.453. [DOI] [PubMed] [Google Scholar]
- Stengel SM, Allemann Y, Zimmerli M, Lipp E, Kucher N, Mohacsi P, Seiler C. Doppler tissue imaging for assessing left ventricular diastolic dysfunction in heart transplant rejection. Heart. 2001;86:432–437. doi: 10.1136/heart.86.4.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sundereswaran L, Nagueh SF, Vardan S, Middleton KJ, Zoghbi WA, Quiñones MA, Torre-Amione G. Estimation of left and right ventricular filling pressures after heart transplantation by tissue Doppler imaging. Am J Cardiol. 1998;83:352–357. doi: 10.1016/S0002-9149(98)00346-4. [DOI] [PubMed] [Google Scholar]
- Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation. 2000;102:1788–1794. doi: 10.1161/01.cir.102.15.1788. [DOI] [PubMed] [Google Scholar]
- Tei C, Ling LH, Hodge DO, Bailey KR, Oh JK, Rodeheffer RJ, Tajik AJ, Seward JB. New index of combined systolic and diastolic myocardial performance: a simple and reproducible measure of cardiac function – a study in normals and dilated cardiomyopathy. J Cardiol. 1995;26:357–366. [PubMed] [Google Scholar]
- Mooradian SJ, Goldberg CS, Crowley DC, Ludomirsky A. Evaluation of a noninvasive index of global ventricular function to predict rejection after pediatric cardiac transplantation. Am J Cardiol. 2000;86:358–360. doi: 10.1016/S0002-9149(00)00935-8. [DOI] [PubMed] [Google Scholar]
- Leonard GT, Fricker FJ, Pruett D, Harker K, Williams B, Schowengerdt KO., Jr Increased myocardial performance index correlates with biopsy-proven rejection in paediatric heart transplant recipients. J Heart Lung Transplant. 2006;25:61–66. doi: 10.1016/j.healun.2005.01.006. [DOI] [PubMed] [Google Scholar]
- Vivekananthan K, Kalapura T, Mehra M, Lavie C, Milani R, Scott R, Park M. Usefulness of the combined index of systolic and diastolic myocardial performance to identify cardiac allograft rejection. Am J Cardiol. 2002;90:517–520. doi: 10.1016/S0002-9149(02)02525-0. [DOI] [PubMed] [Google Scholar]
- Burgess MI, Bright-Thomas RJ, Yonan N, Ray SG. Can the index of myocardial performance be used to detect acute cellular rejection after heart transplantation? Am J Cardiol. 2003;92:308–311. doi: 10.1016/S0002-9149(03)00634-9. [DOI] [PubMed] [Google Scholar]
- Schwitter J, De Marco T, Globits S, Sakuma H, Klinski C, Chatterjee K, Parmley WW, Higgins CB. Influence of felodipine on left ventricular hypertrophy and systolic function in orthotopic heart transplant recipients: possible interaction with cyclosporine medication. J Heart Lung Transplant. 1999;18:1033–1113. doi: 10.1016/S1053-2498(99)00059-5. [DOI] [PubMed] [Google Scholar]
- Goodroe R, Bonnema DD, Lunsford S, Anderson P, Ryan-Baille B, Uber W, Ikonomidis J, Crumbley AJ, VanBakel A, Zile MR, Pereira N. Severe left ventricular hypertrophy 1 year after transplant predicts mortality in cardiac transplant recipients. J Heart Lung Transplant. 2007;26:145–151. doi: 10.1016/j.healun.2006.11.003. [DOI] [PubMed] [Google Scholar]
- Thorn EM, de Filippi CR. Echocardiography in the cardiac transplant recipient. Heart Failure Clin. 2007;3:51–67. doi: 10.1016/j.hfc.2007.02.008. [DOI] [PubMed] [Google Scholar]
- Nguyen V, Cantarovich M, Cecere R, Giannetti N. Tricuspid regurgitation after cardiac transplantation: how many biopsies are too many? J Heart Lung Transplant. 2005;24:S227–S231. doi: 10.1016/j.healun.2004.07.007. [DOI] [PubMed] [Google Scholar]
- Aziz TM, Burgess MI, Rahman AN, Campbell CS, Deiraniya AK, Yonan NA. Risk factors for tricuspid valve regurgitation after orthotopic cardiac transplantation. Ann Thorac Surg. 1999;68:1247–1251. doi: 10.1016/S0003-4975(99)00768-7. [DOI] [PubMed] [Google Scholar]
- Bhatia SJ, Kirshenbaum JM, Shemin RJ, Cohn LH, Collins JJ, Di Sesa VJ, Young PJ, Mudge GH, Jr, Sutton MG. Time course of resolution of pulmonary hypertension and right ventricular remodeling after orthotopic cardiac transplantation. Circulation. 1987;76:819–826. doi: 10.1161/01.cir.76.4.819. [DOI] [PubMed] [Google Scholar]
- Park MH, Scott RL, Uber PA, Harris BC, Chambers R, Mehra MR. Usefulness of B-type natriuretic peptide levels in predicting hemodynamic perturbations after heart transplantation despite preserved left ventricular systolic function. Am J Cardiol. 2002;90:1326–1329. doi: 10.1016/S0002-9149(02)02871-0. [DOI] [PubMed] [Google Scholar]
- Fyfe DA, Mahle WT, Kanter KR, Wu G, Vincent RN, Ketchum DL. Reduction of tricuspid annular Doppler tissue velocities in pediatric heart transplant patients. J Heart Lung Transplant. 2003;22:553–559. doi: 10.1016/S1053-2498(02)00653-8. [DOI] [PubMed] [Google Scholar]
- Galderisi M, Severino S, Cicala S, Caso P. The usefulness of pulsed tissue Doppler for the clinical assessment of right ventricular function. It Heart J. 2002;3:241–247. [PubMed] [Google Scholar]
- Sun JP, Abdalla IA, Asher CR, Greenberg NL, Popoviæ ZB, Taylor DO, Starling RC, Thomas JD, Garcia MJ. Non-invasive evaluation of orthotopic heart transplant rejection by echocardiography. J Heart Lung Transplant. 2005;24:160–165. doi: 10.1016/j.healun.2003.11.400. [DOI] [PubMed] [Google Scholar]
- Valantine HA, Hunt SA, Gibbons R, Billingham ME, Stinson EB, Popp RL. Increasing pericardial effusion in cardiac transplant recipients. Circulation. 1989;79:603–609. doi: 10.1161/01.cir.79.3.603. [DOI] [PubMed] [Google Scholar]
- Al-Dadah AS, Guthrie TJ, Pasque MK, Moon MR, Ewald GA, Moazami N. Clinical course and predictors of pericardial effusion following cardiac transplantation. Transplant Proc. 2007;39:1589–1592. doi: 10.1016/j.transproceed.2006.11.014. [DOI] [PubMed] [Google Scholar]
- Masuyama T, Valantine HA, Gibbons R, Schnittger I, Popp RL. Serial measurement of integrated ultrasonic backscatter in human cardiac allografts for the recognition of acute rejection. Circulation. 1990;81:829–839. doi: 10.1161/01.cir.81.3.829. [DOI] [PubMed] [Google Scholar]
- Angermann CE, Nassau K, Stempfle HU, Krüger TM, Drewello R, Junge R, Uberfuhr P, Weiss M, Theisen K. Recognition of acute cardiac allograft rejection from serial integrated backscatter analyses in human orthotopic heart transplant recipients. Comparison with conventional echocardiography. Circulation. 1997;95:140–150. doi: 10.1161/01.cir.95.1.140. [DOI] [PubMed] [Google Scholar]
- Heimdal A, Steylen A, Torp H, Skiaerpe T. Real time strain rate imaging of the left ventricle by ultrasound. J Am Soc Echocardiogr. 1998;11:1013–1019. doi: 10.1016/S0894-7317(98)70151-8. [DOI] [PubMed] [Google Scholar]
- Eroglu E, Herbots L, Van Cleemput J, Droogne W, Claus P, D'hooge J, Bijnens B, Vanhaecke J, Sutherland GR. Ultrasonic strain/strain rate imaging – a new clinical tool to evaluate the transplanted heart. Eur J Echocardiogr. 2005;6:186–195. doi: 10.1016/j.euje.2004.09.002. [DOI] [PubMed] [Google Scholar]
- Marciniak A, Eroglu E, Marciniak M, Sirbu C, Herbots L, Droogne W, Claus P, D'hooge J, Bijnens B, Vanhaecke J, Sutherland GR. The potential clinical role of ultrasonic strain and strain rate imaging in diagnosing acute rejection after heart transplantation. Eur J Echocardiogr. 2007;8:213–221. doi: 10.1016/j.euje.2006.03.014. [DOI] [PubMed] [Google Scholar]
- Frigerio M, Pedrazzini G, Merli M, Vitali E. Heart Transplantation. In: Savonitto S, editor. Niguarda Cardiovascular Therapy. Il Pensiero Scientifico Editore, Roma; 2006. pp. 437–475. [Google Scholar]
- Desruennes M, Corcos T, Cabrol A, Gandjbakhch I, Pavie A, Léger P, Eugène M, Bors V, Cabrol C. Doppler echocardiography for the diagnosis of acute allograft rejection. J Am Coll Cardiol. 1988;12:63–70. doi: 10.1016/0735-1097(88)90357-9. [DOI] [PubMed] [Google Scholar]
- Simmonds MB, Lythall DA, Slorach C, Ilsley CD, Mitchell AG, Yacoub MH. Doppler examination of superior vena caval flow for the detection of acute cardiac rejection. Circulation. 1992;86:II259–I266. [PubMed] [Google Scholar]
- Morocutti G, Di Chiara A, Proclemer A, Fontanelli A, Bernardi G, Morocutti A, Earle K, Albanese MC, Feruglio GA. Signal-averaged echocardiography and Doppler echocardiographic study in predicting acute rejection in heart transplantation. J Heart Lung Transplant. 1995;14:1065–1072. [PubMed] [Google Scholar]
- Mouly-Bandini A, Vion-Dury J, Viout P, Mesana T, Cozzone PJ, Montiès JR. Value of Doppler echocardiography in the detection of low-grade rejection after cardiac transplantation. Transpl Int. 1996;9:131–136. doi: 10.1007/BF00336390. [DOI] [PubMed] [Google Scholar]
- Picano E, De Pieri G, Salerno JA, Arbustini E, Distante A, Martinelli L, Pucci A, Montemartini C, Viganò M, Donato L. Electrocardiographic changes suggestive of myocardial ischemia elicited by dipyridamole infusion in acute rejection early after heart transplantation. Circulation. 1990;81:72–77. doi: 10.1161/01.cir.81.1.72. [DOI] [PubMed] [Google Scholar]
- Nitenberg A, Tavolaro O, Benvenuti C, Loisance D, Foult JM, Hittinger L, Castaigne A, Cachera JP, Vernant P. Recovery of a normal coronary vascular reserve after rejection therapy in acute human cardiac allograft rejection. Circulation. 1990;81:1312–1318. doi: 10.1161/01.cir.81.4.1312. [DOI] [PubMed] [Google Scholar]
- Tuzcu EM, Kapadia SR, Sachar R, Ziada KM, Crowe TD, Feng J, Magyar WA, Hobbs RE, Starling RC, Young JB, McCarthy P, Nissen SE. Intravascular ultrasound evidence of angiographically silent progression in coronary atherosclerosis predicts long-term morbidity and mortality after cardiac transplantation. J Am Coll Cardiol. 2005;45:1538–1542. doi: 10.1016/j.jacc.2004.12.076. [DOI] [PubMed] [Google Scholar]
- Störk S, Behr TM, Birk M, Uberfuhr P, Klauss V, Spes CH, Angermann CE. Assessment of cardiac allograft vasculopathy late after heart transplantation: when is coronary angiography necessary? J Heart Lung Transplant. 2006;25:1104–1008. doi: 10.1016/j.healun.2006.05.009. [DOI] [PubMed] [Google Scholar]
- Sicari R, Ripoli A, Picano E, Di Giovanbattista R, Minardi G, Matskeplishvili S, Ambatiello S, Pulignano G, Accarino M, Lusa AM, Del Rosso GF, Pedrinelli R, Buziashvili Y. Perioperative prognostic value of dipyridamole echocardiography in vascular surgery: A large-scale multicenter study in 509 patients. EPIC (Echo Persantine International Cooperative) Study Group. Circulation. 1999;100:II269–II274. doi: 10.1161/01.cir.100.suppl_2.ii-269. [DOI] [PubMed] [Google Scholar]
- Akosah KO, Mohanty PK, Funai JT, Jesse RL, Minisi AJ, Crandall CW, Kirchberg D, Guerraty A, Salter D. Noninvasive detection of transplant coronary artery disease by dobutamine stress echocardiography. J Heart Lung Transplant. 1994;13:1024–1038. [PubMed] [Google Scholar]
- Herregods MC, Anastassiou I, Van Cleemput J, Bijnens B, De Geest H, Daenen W, Vanhaecke J. Dobutamine stress echocardiography after heart transplantation. J Heart Lung Transplant. 1994;13:1039–1044. [PubMed] [Google Scholar]
- Derumeaux G, Redonnet M, Mouton-Schleifer D, Bessou JP, Cribier A, Saoudi N, Koning R, Soyer R, Letac B. Dobutamine stress echocardiography in orthotopic heart transplant recipients. VACOMED Research Group. J Am Coll Cardiol. 1995;25:1665–1672. doi: 10.1016/0735-1097(95)00084-H. [DOI] [PubMed] [Google Scholar]
- Derumeaux G, Redonnet M, Mouton-Schleifer D, Cribier A, Soyer R, Letac B. Value of dobutamine echocardiography in the detection of coronary disease in heart transplant patient. Groupe de Recherche VACOMED. Arch Mal Coeur Vaiss. 1996;89:687–694. [PubMed] [Google Scholar]
- Akosah KO, McDaniel S, Hanrahan JS, Mohanty PK. Dobutamine stress echocardiography early after heart transplantation predicts development of allograft coronary artery disease and outcome. J Am Coll Cardiol. 1998;31:1607–1614. doi: 10.1016/S0735-1097(98)00169-7. [DOI] [PubMed] [Google Scholar]
- Derumeaux G, Redonnet M, Soyer R, Cribier A, Letac B. Assessment of the progression of cardiac allograft vasculopathy by dobutamine stress echocardiography. J Heart Lung Transplant. 1998;17:259–267. [PubMed] [Google Scholar]
- Spes CH, Klauss V, Mudra H, Schnaack SD, Tammen AR, Rieber J, Siebert U, Henneke KH, Uberfuhr P, Reichart B, Theisen K, Angermann CE. Diagnostic and prognostic value of serial dobutamine stress echocardiography for noninvasive assessment of cardiac allograft vasculopathy: a comparison with coronary angiography and intravascular ultrasound. Circulation. 1999;100:509–515. doi: 10.1161/01.cir.100.5.509. [DOI] [PubMed] [Google Scholar]
- Bacal F, Moreira L, Souza G, Rodrigues AC, Fiorelli A, Stolf N, Bocchi E, Bellotti G, Ramires JA. Dobutamine stress echocardiography predicts cardiac events or death in asymptomatic patients long-term after heart transplantation: 4-year prospective evaluation. J Heart Lung Transplant. 2004;23:1238–1244. doi: 10.1016/j.healun.2003.09.007. [DOI] [PubMed] [Google Scholar]
- Borow KM, Neumann A, Arensman FW, Yacoub MH. Cardiac and peripheral vascular responses to adrenoceptor stimulation and blockade after cardiac transplantation. J Am Coll Cardiol. 1989;14:1229–1238. doi: 10.1016/0735-1097(89)90421-X. [DOI] [PubMed] [Google Scholar]
- Kociolek LK, Bierig SM, Herrmann SC, Labovitz AJ. Efficacy of atropine as a chronotropic agent in heart transplant patients undergoing dobutamine stress echocardiography. Echocardiography. 2006;23:383–387. doi: 10.1111/j.1540-8175.2006.00223.x. [DOI] [PubMed] [Google Scholar]
- Ciliberto GR, Massa D, Mangiavacchi M, Danzi GB, Pirelli S, Faletra F, Frigerio M, Gronda E, De Vita C. High-dose dipyridamole echocardiography test in coronary artery disease after heart transplantation. Eur Heart J. 1993;14:48–52. doi: 10.1093/eurheartj/14.1.48. [DOI] [PubMed] [Google Scholar]
- Ciliberto GR, Parodi O, Cataldo G, Mangiavacchi M, Alberti A, Parolini M, Frigerio M. Prognostic value of contractile response during high-dose dipyridamole echocardiography test in heart transplant recipients. J Heart Lung Transplant. 2003;22:526–532. doi: 10.1016/S1053-2498(02)01238-X. [DOI] [PubMed] [Google Scholar]
- Tona F, Caforio AL, Montisci R, Angelini A, Ruscazio M, Gambino A, Ramondo A, Thiene G, Gerosa G, Iliceto S. Coronary flow reserve by contrast-enhanced echocardiography: a new noninvasive diagnostic tool for cardiac allograft vasculopathy. Am J Transplant. 2006;6:998–1003. doi: 10.1111/j.1600-6143.2006.01298.x. [DOI] [PubMed] [Google Scholar]
- Tona F, Caforio AL, Montisci R, Gambino A, Angelini A, Ruscazio M, Toscano G, Feltrin G, Ramondo A, Gerosa G, Iliceto S. Coronary flow velocity pattern and coronary flow reserve by contrast-enhanced transthoracic echocardiography predict long-term outcome in heart transplantation. Circulation. 2006;114:I49–I55. doi: 10.1161/CIRCULATIONAHA.105.001321. [DOI] [PubMed] [Google Scholar]
- Giacomin E, Gasperini S, Zacà V, Ballo P, Diciolla F, Bernazzali S, Maccherini M, Chiavarelli M, Galderisi M, Mondillo S. Relationship of coronary microcirculatory dysfunction and left ventricular longitudinal function in heart transplant recipients. J Heart Lung Transplant. 2008. [DOI] [PubMed]
- Mortensen SA, Egeblad H. Endomyocardial biopsy guided by cross-sectional echocardiography. Br Heart J. 1983;50:246–251. doi: 10.1136/hrt.50.3.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aggarwal M, Drachenberg C, Douglass L, de Filippi C. The efficacy of real-time 3-dimensional echocardiography for right ventricular biopsy. J Am Coll Cardiol. 2005;18:1208–1212. doi: 10.1016/j.echo.2005.04.009. [DOI] [PubMed] [Google Scholar]
- Amitai ME, Schnittger I, Popp RL, Chow J, Brown P, Liang DH. Comparison of three-dimensional echocardiography to two-dimensional echocardiography and fluoroscopy for monitoring of endomyocardial biopsy. Am J Cardiol. 2007;99:864–866. doi: 10.1016/j.amjcard.2006.10.050. [DOI] [PubMed] [Google Scholar]
- Marelli D, Laks H, Fazio D, Moore S, Moriguchi J, Kobashigawa J. The use of donor hearts with left ventricular hypertrophy. J Heart Lung Transplant. 2000;19:496–50. doi: 10.1016/S1053-2498(00)00076-0. [DOI] [PubMed] [Google Scholar]
- Brock MV, Salazar JD, Cameron DE, Baumgartner WA, Conte JV. The changing profile of the cardiac donor. J Heart Lung Transplant. 2001;20:1005–1009. doi: 10.1016/S1053-2498(01)00297-2. [DOI] [PubMed] [Google Scholar]
- Zaroff JG, Rosengard BR, Armstrong WF, Babcock WD, D'Alessandro A, Dec GW, Edwards NM, Higgins RS, Jeevanandum V, Kauffman M, Kirklin JK, Large SR, Marelli D, Peterson TS, Ring WS, Robbins RC, Russell SD, Taylor DO, Van Bakel A, Wallwork J, Young JB. Consensus conference report: maximizing use of organs recovered from the cadaver donor: cardiac recommendations, March 28–29, 2001, Crystal City, Va. Circulation. 2002;106:836–841. doi: 10.1161/01.CIR.0000025587.40373.75. [DOI] [PubMed] [Google Scholar]
- Sopko N, Shea KJ, Ludrosky K, Smedira N, Hoercher K, Taylor DD, Starling RR, Gonzalez-Stawinski GV. Survival is not compromised in donor hearts with echocardiographic abnormalities. J Surg Res. 2007;143:141–144. doi: 10.1016/j.jss.2007.04.026. [DOI] [PubMed] [Google Scholar]
- Arpesella G, Gherardi S, Bombardini T, Picano E. Recruitment of aged donor heart with pharmacological stress echo. A case report. Cardiovasc Ultrasound. 4:3. doi: 10.1186/1476-7120-4-3. 2006 Jan 24; [DOI] [PMC free article] [PubMed] [Google Scholar]