

Abstract
Objectives. We sought to outline an optimistic yet achievable goal for future US smoking prevalence rates based on empirical evidence reflecting the success of smoking control efforts in California.
Methods. Using a dynamic model and the smoking initiation and cessation rates achieved in California as a guide, we projected US adult smoking prevalence rates through the year 2020.
Results. If smoking initiation and cessation rates for the nation do not change, population dynamics will result in smoking prevalence rates falling to 19.1% in 2010 and 16.8% in 2020. If the country attains California’s initiation and cessation rates by 2010, adult smoking prevalence rates will be 18.5% in 2010 and 14.7% as of 2020.
Conclusions. If California’s smoking initiation and cessation rates are attained nationwide, the US smoking prevalence rate could be 5.9 percentage points lower than the 2005 rate by the year 2020, and there would be 10.2 million fewer smokers than in 2005. A target of 14% smoking prevalence by 2020 is aggressive yet feasible, given that it takes into account the constraints imposed by population demographics.
Adult smoking prevalence rates in the United States continue to decline, although painfully slowly. Despite enormous progress in smoking control during the past 40 years (the adult prevalence rate dropped from 42.4% in 1965 to 20.9% in 20051), cigarette smoking remains the leading cause of premature death among Americans, killing approximately 440 000 citizens annually.2 Currently, more than 44 million Americans smoke, and half of these individuals will die prematurely unless they abandon their addiction in time.3
The overall US smoking prevalence rate of 20.9% in 2005 (the most recent year for which data were available at the time this article was written) reflects a diverse combination of rates stemming from the differences between states in terms of demographic characteristics and implementation of tobacco control efforts. Rates vary from a low of 11.5% in Utah, commonly attributed to the state’s large Mormon population, to a high of 28.7% in Kentucky, where population demographics, the prominence of tobacco in the history and economy of the state, and limited tobacco control efforts contribute to the persistently high prevalence of smoking.4
We addressed the question of how much lower, and how much faster, overall US smoking prevalence rates would fall by the year 2020 if the initiation and cessation rates achieved as of 2005 in California, the state with the second lowest adult smoking prevalence in the country (15.2% in 2005), could be reproduced across the entire country. Assessing the degree to which there is a causal link between antismoking policies and declining smoking prevalence rates in California or any other state is challenging because it is plausible that regions with strong antitobacco attitudes are more likely to implement stringent smoking control measures.5
However, proof of causality is not necessary to make our intended point. If we assume, correctly or otherwise, that smoking control policies are solely responsible for California’s smoking initiation and cessation rates—and therefore its low smoking prevalence—replicating those rates across the country would allow us to derive an optimistic scenario for smoking trends in the United States in the immediate future given the effectiveness of currently available tobacco control programs. Given that the government is currently initiating the process of setting objectives for its Healthy People 2020 program, an analysis of these trends could assist the nation in selecting a challenging yet potentially reachable smoking prevalence target for the year 2020 based on best-case effects of tobacco control programming.
SELECTION OF CALIFORNIA AS THE REFERENT STATE
Despite having the lowest smoking rate in the country, Utah was not a suitable candidate as a model in our analysis because the state’s unique demographic characteristics—rather than its tobacco control policies —are largely responsible for its low smoking prevalence. Other states, including California, Massachusetts, and New York, have been widely recognized as leaders in tobacco control.
New York has received a great deal of recent attention for its success in reducing smoking prevalence rates. A 2005 independent evaluation of the state’s antismoking and tobacco control program showed that smoking is on the decline in New York and that smoking among adolescents is being reduced at a pace that exceeds the national average. New York’s adult smoking prevalence rate declined from 21.6% in 2003 to 19.9% in 2004 (a decrease of 8%); by comparison, the rate for the country as a whole fell from 21.6% to 20.9% during the same period (a decrease of 3%). This success has been attributed to recent increases in cigarette taxes, strong clean indoor air laws, and the nearly $230 million that New York has committed since 2000 to fight tobacco use.6
However, as seemingly impressive as New York’s recent tobacco control accomplishments may be, California, as a result of its longer history of sustained tobacco control efforts and achievements, holds a more prominent place in most knowledgeable observers’ lists of tobacco control success stories. As such, it is frequently cited as a model for its implementation of highly successful tobacco control efforts. After California voters passed Proposition 99, the 1988 initiative that established the state’s antitobacco program, California’s adult smoking rate dropped 33% over the subsequent 17 years (from 22.8% in 1988 to 15.2% in 2005). By comparison, during the same period, the adult smoking prevalence rate in the United States as a whole dropped from 24.1% to 20.9%, a decrease of only 13%.
California’s success has been attributed to its cigarette tax policy, an aggressive antismoking media campaign, and its trend-setting smoke-free indoor air policies, as well as the state’s community tobacco education programs.7 California’s experience has been documented and discussed in several studies, some of them debating the extent of the antitobacco program’s effects.8,9 What cannot be contested, however, is that California has achieved the nation’s second lowest state adult smoking prevalence rate and is considered by many tobacco control advocates the gold standard for what can be achieved through a sustained and comprehensive smoking control program.
We do not claim that California’s tobacco control efforts are solely responsible for the drop in the state’s smoking rates. For example, California’s population demographics differ from those of the nation as a whole, and it is plausible that different racial/ethnic or socioeconomic population groups will have different initiation and cessation rates quite independent of the presence or absence of tobacco control programs and policies. (We are investigating this question in a study now in progress. Preliminary findings indicate that although demographic characteristics play a role in explaining California’s low smoking rates, the majority of the gap between national and California prevalence rates is because of the effectiveness of California’s tobacco control initiatives.)
California’s example presents an opportunity to determine an optimistic yet feasible trajectory for the nation’s smoking rates. Such a trajectory can be established by assuming that the entire country can achieve California’s lower-than-average smoking initiation rates and higher-than-average cessation rates. Beginning with the 2005 age- and gender-specific smoking prevalence rates in the national population, we used California’s experience to estimate an optimistic path for smoking prevalence rates nationwide, assuming a strong impact from tobacco control programming.
METHODS
We used a dynamic smoking prevalence model (described elsewhere10) to project future smoking prevalence rates under different smoking initiation and cessation rate scenarios. The model predicts future smoking prevalence rates by estimating future US population sizes by age and smoking status. For its baseline predictions, the model uses age-specific smoking initiation and cessation rates estimated from National Health Interview Survey data.
The model does not predict future smoking prevalence rates by simply extrapolating current smoking trends. Instead, it incorporates dynamic population structures that determine smoking rates. The model simulates, on the basis of best estimates of birth, mortality, and smoking initiation and cessation rates, the status of the adult smoking population in the United States at a given point in the future. The model has been used in previous policy analyses,11,12 and its predictions have been validated.13
In our analyses, we introduced several modifications to the smoking prevalence model. First, we updated age-specific population figures using data from the 2000 US census. Second, we updated death rates with figures from 2000.14 Finally, we set the national smoking prevalence rate for 2005 at 20.9% to conform to recent National Health Interview Survey prevalence estimates1 (in our analyses, we projected forward from 2005; at the time this article was written, the 2006 prevalence estimate was not yet available).
We used the smoking prevalence model to produce estimates of smoking rates among US adults from 2005 to 2020 under 3 alternative sets of assumptions:
2005 national initiation and cessation rates will continue indefinitely. We termed this set of conditions the “status quo” scenario.
The United States attains California’s initiation and cessation rates instantaneously in 2006.
The United States will attain California’s initiation and cessation rates gradually (linearly), by 2010.
We set the status quo smoking initiation rate for the nation at 25%, consistent with the prevalence rate for the 18- to 24-year age group observed in recent years.1 We set annual cessation rates for the status quo scenario as those we calculated previously10: 0.21% for the 18- to 30-year age group, 2.15% for the 31- to 50-year age group, and 5.97% for individuals aged 51 years or older. Using these age-specific cessation rates, we estimated that the overall US cessation rate for 2005 was 2.59%. We used age-specific Behavioral Risk Factor Surveillance System (BRFSS) estimates of adult smoking prevalence rates in California from 2000 to 2005 and age-specific estimates of the state’s population for 2000 to estimate California’s cessation rate in 2005 as 3.33%.4,14
We used age-specific death rates to calculate trends in the aging of the population from 2000 to 2005, and for every year, we computed adult smoking prevalence assuming a single cessation rate for the population. We estimated the single cessation rate as the value that best matched the calculated overall adult smoking prevalence rate and the rate reported in the BRFSS for the years 2000 to 2005. To obtain national age-specific cessation rates consistent with the aggregate quit rate achieved in California (3.33%), we multiplied status quo age-specific cessation rates by the ratio of California’s estimated cessation rate to the overall US cessation rate (1.28×[3.33/2.59]).
Our analysis showed that the initiation and cessation rates we estimated for California for 2000 to 2005 indeed captured the decline in prevalence rates observed in the state during that period. In particular, the BRFSS data showed that, between 2000 and 2005, the prevalence rate in California dropped from 17.2% to 15.2%, a reduction of 2 percentage points. For the same period, our model showed a drop from 17.4% to 15.5%, a reduction of 1.9 percentage points. A graph contrasting our model’s results and the actual BRFSS-reported prevalence rates for 2000 to 2005 is shown in Figure 1 ▶.
FIGURE 1—
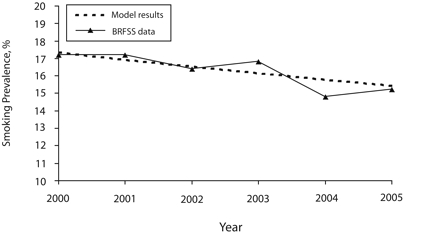
Comparison of Behavioral Risk Factor Surveillance System (BRFSS) annual smoking initiation and cessation rates and rates estimated from the present model: California, 2000–2005.
RESULTS
The status quo scenario depicted in Figure 2 ▶ indicates our projection for US smoking prevalence rates under the assumption that the 2005 national initiation and cessation rates (25% and 2.59%, respectively) will continue at least until the year 2020. Table 1 ▶ presents specific estimates of national prevalence rates and the size of the smoking population under each alternative scenario for 2010 and 2020.
FIGURE 2—
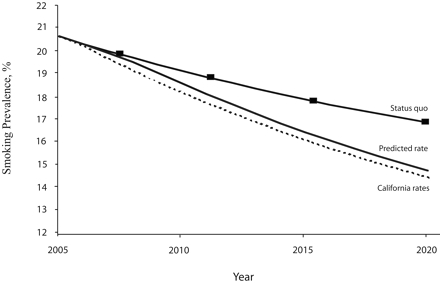
Projections of US adult smoking prevalence rates under status quo scenario and California rate scenarios: 2005–2020.
Note. The bottom 2 lines depict corresponding scenarios assuming that the United States as a whole achieves California’s 2005 rates (20% initiation rate and 3.33% cessation rate). The dotted line reflects the assumption that such rates are attained instantaneously (in 2006), whereas the solid line reflects the more plausible scenario that such rates will be achieved gradually (by 2010). The status quo initiation rate is 25% and the cessation rate is 2.59%.
TABLE 1—
Estimates of Adult Smoking Prevalence Rates and Number of Smokers Under Different Scenarios: United States, 2005, 2010, and 2020
| 2005 | 2010 | 2020 | ||||
| Scenario | Prevalence, % | No. of Smokers (Millions) | Prevalence, % | No. of Smokers (Millions) | Prevalence, % | No. of Smokers (Millions) |
| Status quo | 20.9 | 44.6 | 19.1 | 42.8 | 16.8 | 39.3 |
| California rates achieved in 2006 | 20.9 | 44.6 | 18.1 | 40.7 | 14.4 | 33.7 |
| California rates achieved by 2010 | 20.9 | 44.6 | 18.5 | 41.6 | 14.7 | 34.4 |
Our status quo scenario predicted that adult smoking prevalence rates would continue to decline for the foreseeable future. The results showed an expected decline, under 2005 initiation and cessation rates, from a 20.9% prevalence rate in 2005 to a rate of 16.8% in 2020, a drop of 4.1 percentage points (or 19.6%) in 15 years. This drop translates into a decline from 44.6 million smokers in 2005 to 39.3 million in 2020, or 5.3 million fewer smokers over the 15-year period (note that the 2020 figure incorporates population growth as well as smoking declines).
If the country could achieve California’s initiation and cessation rates, smoking prevalence rates would drop at an accelerated pace in comparison with the status quo scenario. By the year 2020, this scenario would lead to an adult smoking prevalence rate of 14.7%, a drop of 6.2 percentage points (29.7%) from the 2005 national prevalence of 20.9%, if California rates were achieved by 2010. This represents a decline from 44.6 million smokers in 2005 to 34.4 million in 2020, or 10.2 million fewer smokers. Relative to the status quo, this scenario would lead to a reduction in prevalence of 2.1 percentage points (from 16.8% to 14.7%) and a corresponding 4.9 million fewer smokers (from 39.3 million to 34.4 million) by 2020.
DISCUSSION
Our results suggest that, under a best-case scenario (assuming a strong causality effect between smoking control policies and smoking rates), nationwide adoption of strong antismoking measures, as has occurred in California, would substantially increase the rate of decline in smoking relative to the decline that would be achieved if the nation’s current initiation and cessation rates persisted. If the nation achieves California’s 2005 initiation and cessation rates, there will be nearly 5 million fewer smokers in 2020 than under the status quo scenario, a difference with dramatic implications for the mortality toll associated with smoking.
Our analysis offers a guide for selecting challenging yet feasible future national goals for US smoking prevalence rates. For example, our results indicate that, under current conditions, the adult prevalence rate will be slightly below 17% in the year 2020. If the country replicates the initiation and cessation achievements obtained by California, however, the prevalence would drop below 15%. Considering the possibility that sympathetic political leaders and advances in social policy or cessation technology during the next 13 years may result in improvements in California initiation and cessation rates, a target of 14% for the year 2020 is ambitious but potentially reachable; such an effort may well meet with success, but it demands the best performance from the nation as a whole.
A word of analytic caution is necessary. Some of our estimates are imprecise. For example, our failure to incorporate population in-migration and out-migration rates in our analysis of cessation rates may have had a minor effect on our specific estimates. Clearly, however, that effect would not have been sufficiently large to substantially influence our conclusions.
We do not discount the possibility that more-effective means of reducing tobacco use than those implemented in California may be identified in the near future, and if so, smoking prevalence rates could decline faster than would be the case with our predictions. However, as a guide to what might be attainable in the years to come, California’s experience with tobacco control highlights an optimistic but feasible scenario for future smoking prevalence rates in the United States.
Acknowledgments
This work was commissioned by the Institute of Medicine of the National Academy of Sciences for the institute’s Reducing Tobacco Use: Strategies, Barriers, and Consequences project.
Human Participant Protection No protocol approval was needed for this study.
Peer Reviewed
Contributors Both authors were involved in the design and analysis phases of the study and in the writing of the article.
The Institute of Medicine’s Committee on Reducing Tobacco Use reviewed the analysis and portions of the results presented in this article. We thank the committee for its helpful suggestions. We alone are responsible for any errors.
References
- 1.Centers for Disease Control and Prevention. Smoking prevalence among adults. Available at: http://www.dhs.ca.gov/tobacco/documents/press/PressRelease05-22-05.pdf. Accessed November 24, 2006.
- 2.Centers for Disease Control and Prevention. Annual smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 1999–2001. MMWR Morb Mortal Wkly Rep. 2005;54: 625–628. [PubMed] [Google Scholar]
- 3.Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System (BRFSS). Available at: http://www.cdc.gov/brfss. Accessed November 24, 2006.
- 5.Chaloupka FJ, Warner KE. The economics of smoking. In: Culyer AJ, Newhouse JP, eds. Handbook of Health Economics. Amsterdam, the Netherlands: Elsevier; 2000:1539–1627.
- 6.Governor announces NY’s antismoking successes outpace nation. Available at: http://www.ny.gov/governor/press/05/oct25_1_05.htm. Accessed November 24, 2006.
- 7.California smoking rates drop 33 percent since state’s antitobacco program began. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/adult/table_4.htm. Accessed September 26, 2007.
- 8.Pierce JP, Gilpin EA, Emery SL, et al. Has the California tobacco control program reduced smoking? JAMA. 1988;280:893–899. [DOI] [PubMed] [Google Scholar]
- 9.Pierce JP, Evans N, Farkas AJ, et al. Tobacco Use in California: An Evaluation of the Tobacco Control Program, 1989–1993. La Jolla, Calif: University of California, San Diego; 1994.
- 10.Mendez D, Warner KE, Courant PN. Has smoking cessation ceased? Expected trends in the prevalence of smoking in the United States. Am J Epidemiol. 1998; 148:249–258. [DOI] [PubMed] [Google Scholar]
- 11.Mendez D, Warner KE. Smoking prevalence in 2010: why the Healthy People goal is unattainable. Am J Public Health. 2000;90:401–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Warner KE, Mendez D, Smith DG. The financial implications of coverage of smoking cessation treatment by managed care organizations. Inquiry. 2004; 41:57–69. [DOI] [PubMed] [Google Scholar]
- 13.Mendez D, Warner KE. Adult cigarette smoking prevalence: declining as expected (not as desired). Am J Public Health. 2004;94:251–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Statistical Abstract of the United States: 2000. 120th ed. Washington, DC: US Census Bureau; 2001.