

Abstract
Background
Major depression (MD) and posttraumatic stress disorder (PTSD) are highly comorbid. The degree to which a common genetic liability explains the etiology of the MD-PTSD association has not been quantified and has important implications for research and prevention.
Methods
This paper presents an analysis of data from 6,744 members of the Vietnam Era Twin Registry. MD and PTSD were assessed using the Diagnostic Interview Schedule-III-R in 1991–92. Bivariate twin modeling was conducted to determine the genetic and environmental etiology of the MD-PTSD association.
Results
The best-fitting model for the MD-PTSD association included a substantial genetic correlation(r=.77; 95% CI,.50–1.00) and a modest individual-specific environmental correlation(r=.34; 95% CI,.19–.48). Common genetic liability explained 62.5% of MD-PTSD comorbidity. Genetic influences common to MD explained 15% of the total variance in risk for PTSD and 58% of the genetic variance in PTSD. Individual-specific environmental influences common to MD explained only 11% of the individual-specific environmental variance in PTSD.
Limitations
Our participants were male Vietnam era veterans and our findings may not generalize to civilians, females or other cohorts.
Conclusions
MD – PTSD comorbidity is largely explained by common genetic influences. Substantial genetic overlap between MD and PTSD implies that genes implicated in the etiology of MD are strong candidates for PTSD and vice versa. Environmental influences on MD and PTSD explain less of their covariation and appear to be largely disorder-specific. Research is needed to identify environmental factors that influence the development of MD versus PTSD in the context of common genetic liability.
INTRODUCTION
Major depression (MD) and posttraumatic stress disorder (PTSD) are highly comorbid in epidemiological and clinical samples (Kessler et al., 1995; Orsillo et al., 1996). Pre-existing depression increases risk for both exposure to potentially-traumatic events and for developing PTSD among individuals exposed to such events (Breslau et al., 1998). The incidence of first-onset depression is elevated among individuals who develop PTSD following trauma compared to the trauma-exposed who do not develop PTSD (Breslau et al., 2000). Thus, the relation between MD and PTSD is multifaceted; MD appears to increase risk for PTSD and vice versa. However, the MD-PTSD association could also be explained by a common genetic vulnerability.
The twin method exploits the different level of genetic relatedness between monozygotic (MZ) and dizygotic (DZ) twin pairs to estimate the contribution of genetic and environmental factors to individual differences in the relation between two phenotypes, such as MD and PTSD.(Plomin et al., 2001) Population covariance between MD and PTSD may be partitioned into an additive genetic component and two types of environmental components. The first is a shared environmental effect that is correlated between twins and has made siblings similar to each other. The second is an individual-specific environmental effect that is uncorrelated between siblings and includes measurement error.
This study is the first to use a twin design to quantify the degree to which a common genetic vulnerability explains the etiology of the association between MD and PTSD. Genetic influences explain a substantial proportion of the variance in MD (Lyons et al., 1998) and PTSD (True et al., 1993) individually and may explain their covariation. Moreover, emerging evidence supports a shared diathesis between anxiety and mood disorders. Dilsaver et al recently demonstrated that a familial loading for mood disorders was associated with increased risk of a range of anxiety disorders. The authors also found a dose-response relationship between the number of comorbid anxiety disorders and a familial loading for mood disorders(Dilsaver et al., 2006). Prior research on a small subset of the sample used in the present study suggested that the familial association between MD and combat-related PTSD was genetically mediated, but this study was unable to quantify the extent to which MD-PTSD comorbidity is explained by a common genetic liability.(Koenen et al., 2003) Genetic influences on both disorders overlap with those for generalized anxiety disorder (Chantarujikapong et al., 2001; Kendler, 1996) and with alcohol dependence (Fu et al., 2002; Xian et al., 2000). Given the attention and debate surrounding the etiology of the MD-PTSD association in the literature (Neria and Bromet, 2000), it is surprising the role of genetic influences on their comorbidity has not been quantified previously. The twin studies that have examined the genetic overlap between MD and anxiety disorders have not included PTSD (Hettema et al., 2006).
METHODS
Sample
Participants were from the Vietnam Era Twin (VET) Registry, a nationally distributed cohort consisting of male-male twin pairs born between 1939 and 1957 who served on active military duty during the Vietnam War era (Eisen et al., 1989; Henderson et al., 1990). Zygosity was determined using a questionnaire and blood group typing methodology that achieved 95% accuracy (Eisen et al., 1989). Data used in the present study were from the 1992 Harvard Twin Study of Drug Abuse and Dependence. The response rate for this study was 79.6% (Tsuang et al., 2001). Demographic characteristics of the sample in in 1992 were: mean age=44.6 years (SD=2.8); 90.4% non-Hispanic white, 4.9% African-American, 2.7% Hispanic, 2.0% Native American or other; >70% received at least a high school education; 92% employed full-time; 75% married, 11% never married; 55.6% were monozygotic twins.
MD and PTSD Diagnoses
Lifetime MD and PTSD diagnoses were obtained using the Mental Health Diagnostic Interview Schedule Version-III-revised (DIS-III-R;(Robins et al., 1988), a structured psychiatric interview for epidemiological research leading to clinical diagnoses based on Diagnostic and Statistical Manual Third Edition Revised(DSM-III-R). Details of the interview procedure, types of traumatic events reported, MD and PTSD diagnoses were reported previously (Koenen et al., 2002; Lyons et al., 1998).
Statistical Analysis
The bivariate twin method exploits the different level of genetic relatedness between monozygotic (MZ) and dizygotic (DZ) twin pairs to estimate the contribution of genetic and environmental factors to the association between phenotypes. If the cross-twin cross-phenotype MD-PTSD association is significantly stronger in MZ than DZ pairs, this suggests a common genetic liability contributes to their covariation (Plomin et al., 2001). To test this hypothesis, we first compared tetrachoric correlations separately for MZ and DZ pairs. The tetrachoric correlation estimates the correlation between the underlying liability distribution rather than the observed dichotomous variables.
Next, we examined the etiology of the MD-PTSD association using Mplus 3.11 which employs maximum-likelihood estimation techniques to fit different structural equations to raw data (Muthen and Muthen, 2004; Prescott, 2004). The univariate model fitting results for MD (Lyons et al., 1998) and PTSD (True et al., 1993) published previously included significant terms for additive genetic influences(A) and individual-specific environmental influences which include measurement error(E). Shared environmental influences(C) did not significantly contribute to the variance in MD or PTSD. In our bivariate twin analysis, we tested a series of nested models to determine whether the MD-PTSD association was best explained by genetic, shared environmental or individual-specific environmental influences. When models are nested (i.e., identical with the exception of constraints), the difference in fit between models is tested by the difference in the χ2 values (Δχ2) using as its degrees of freedom the df difference of the two models. If the Δχ2 is not statistically significant, the more parsimonious model is selected.
We hypothesized that the best-fitting model would include a significant genetic correlation(rA) between additive genetic influences on MD and those on PTSD. Model fit was evaluated using three model-selection statistics: χ2 goodness-of- fit statistic; the comparative fit index (CFI), values greater than .95 indicate good-fit(Hu and Bentler, 1999); root mean square error of approximation (RMSEA), values less then .05 indicate close fit to the data(Browne and Cudeck, 1993). Mplus 3.11 does not provide 95% confidence intervals for standardized parameter estimates. These were obtained for the best-fitting model using Mx 1.701 on raw data (Neale et al., 2002).
RESULTS
The lifetime prevalence of MD was 9.2% (n=633). The lifetime prevalence of trauma exposure was 45.4% (n=3,065); 21.1% (n=649) of the exposed received a lifetime diagnosis of PTSD. Trauma-exposed subjects with lifetime MD were much more likely to meet criteria for PTSD (49.5%) than those without MD (16.5%; OR=4.98, 95% CI:4.00–6.20).
Etiology of the association between MD and PTSD
The best estimate of the phenotypic correlation between liability to MD and PTSD was .46. Table 1 presents the tetrachoric correlations for MD and PTSD by zygosity. The higher cross-twin cross-phenotype correlations among MZ compared to DZ twins suggested genetic influences on the MD–PTSD association.
Table 1.
Tetrachoric correlation matrix for major depression (MD) and posttraumatic stress disorder (PTSD)
| MZ (n=1874) | MD Twin 1 | PTSD Twin 1 | MD Twin 2 | PTSD Twin 2 |
|---|---|---|---|---|
| MD twin 1 | 1.00 | |||
| PTSD twin 1 | .42 | 1.00 | ||
| MD twin 2 | .42 | .27 | 1.00 | |
| PTSD twin 2 | .25 | .34 | .44 | 1.00 |
|
| ||||
| DZ (n= 1498) | ||||
|
| ||||
| MD twin 1 | 1.00 | |||
| PTSD twin 1 | .48 | 1.00 | ||
| MD twin 2 | .13 | .07 | 1.00 | |
| PTSD twin 2 | .04 | .22 | .52 | 1.00 |
Abbreviations: MD, major depression; PTSD, posttraumatic stress disorder; MZ, monozygotic; DZ, dizygotic. Bold text, cross twin, same phenotype correlations; Italic text, cross twin, cross phenotype correlations.
p<.05 all.
Bivariate twin modeling was used to quantify the degree to which a common genetic liability contributed to the MD-PTSD association. The best-fitting bivariate model (Figure 1) consisted of significant genetic and individual-specific environment factors influencing the covariation between phenotypes and provided excellent fit to the data (χ2(14)=14.70, ns; CFI=1.00; RMSEA=.005). Model fit did not deteriorate significantly if the shared environmental influences specific to MD and PTSD and those influencing their covariation were fixed to zero (Δχ2[3]=0.00, ns). However, model fit deteriorated significantly if additive genetic (Δχ2[1]=30.83, p<.001; CFI=.90; RMSEA=.04) or individual-specific environmental influences (Δχ2[1]=16.05, p<.001; CFI=.95; RMSEA=.03) were hypothesized to have no effect on the MD-PTSD association. A model where the genetic correlation between MD and PTSD was constrained to unity (rA=1.00; χ2(15)=17.94, ns; CFI=.99; RMSEA=.01) did not fit as well as one in which the genetic correlation was freely estimated.
Figure 1. Standardized variance estimates for the bivariate model of association between major depression (MD) and posttraumatic stress disorder (PTSD) in male twins.
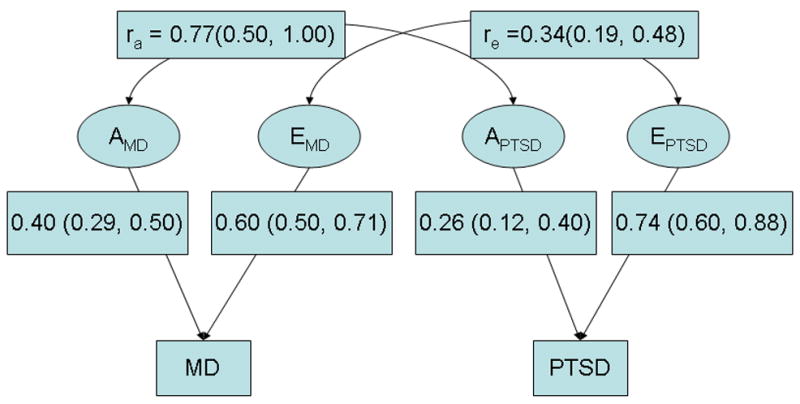
The model presents the standardized variance estimates of the AE model for MD and PTSD and their genetic (rA) and individual-specific environmental correlation (re). Amd and Emd refer to additive genetic and individual-specific environmental (including error) influences on major depression. Aptsd and Eptsd refer to additive genetic and individual-specific environmental (including error) influences on posttraumatic stress disorder. The model is displayed for twin 1 only; the model for twin 2 would look identical. The variances of the latent variables are fixed at 1. The parameter estimates were squared to determine how much of the variation in each phenotype is accounted for by latent factors. All parameter estimates are statistically significant p < .05.
Additive genetic influences and individual-specific environmental influences explain 40% and 60% of the variance in MD and 26% and 74% if the variance in PTSD, respectively. 24% of the variance in PTSD is explained by genetic and environmental influences common to MD. We also computed the amount of genetic variance in risk for PTSD that is common to MD, where rA is the genetic correlation coefficient and hptsd is the total genetic variance in risk for PTSD. Thus, [rA*(hptsd)1/2]2=15% of the total variance in risk for PTSD overlaps with the genetic risk for MD. Additive genetic influences common to MD account for 58%(15%/26%) of the genetic variance in PTSD. Individual-specific environmental influences common to MD explain only 8.5% of the total variance and 11% of the individual-specific environmental variance in PTSD. In addition, we can use the data in Figure 1 to calculate the proportion of MD-PTSD covariance that is explained by a common genetic liability (15%/24%), 62.5%.
DISCUSSION
The overlap between MD and PTSD among middle-aged male twins was largely due to a common genetic liability that explained over 62% of the MD-PTSD covariance. In fact, genetic influences common to MD explained 15% of the total variation and 58% of the genetic variation in PTSD. Although it was not assessed in our study, the heritable personality trait of neuroticism may be a premorbid manifestation of this common genetic diathesis(Jang et al., 1996). Neuroticism has been associated with increased risk of developing MD(Khan et al., 2005) and PTSD individually.(Breslau et al., 1995) Neurotism is moderately heritable and largely explains the genetic overlap between MD and other anxiety disorders such as generalized anxiety disorder and panic disorder (Hettema et al., 2006). The personality trait of neuroticism may also underlie MD-PTSD comorbidity.
The substantial genetic overlap between MD and PTSD implies that genes associated with MD are good candidates for PTSD and vice versa. Since PTSD requires exposure to a potentially-traumatic life event, genes shown to modify the effect of environmental adversity on risk of MD are particularly strong candidates for PTSD. Caspi et al (2006) were the first to demonstrate that the short-version (s-allele) of a functional polymorphism in the promoter region of the serotonin transporter gene (SLC6A4) moderated the effect of adverse life events on risk of MD (Caspi and Moffitt, 2006). The s-allele has been associated with PTSD in a Korean sample (Lee et al., 2005). A recent study by Kipatrick et al. (under review) of adults exposed to the 2004 Florida hurricanes provides particularly compelling evidence that genetic variants shown to modify risk of developing MD in response to environmental adversity also modify risk of developing PTSD following trauma exposure. They found this same polymorphism in SLC6A4 moderated risk of both post-disaster PTSD and MD, but only under the high stress conditions of conditions of high hurricane exposure and low social support(Kilpatrick et al., Under Review). In addition, polymorphisms in FKBP5, a glucocorticoid-regulating cochaperone of stress proteins, which were associated with recurrence of major depressive episodes and response to antidepressant treatment have also been associated with peri-traumatic dissociation, a risk factor for PTSD (Binder et al., 2004; Koenen et al., 2005). Further molecular genetic studies of PTSD are needed.
Although some of the same putative environmental risk factors have been linked to both MD and PTSD, our data indicate the majority of their covariation arises largely from a genetically-transmitted process. Moreover, individual-specific environmental influences were only modestly correlated for both disorders. This implies that the environmental factors implicated in the etiology of MD and PTSD are largely disorder specific. This result is consistent with previous research suggesting that life events involving threat are associated with anxiety disorders and those involving loss are more strongly associated with mood disorders (Eley and Stevenson, 2000). Further research is needed to identify environmentally-mediated risk factors that influence the development of MD versus PTSD.
This study has several limitations. Our participants were male Vietnam era veterans and our findings may not generalize to civilians, females or other cohorts. Our study relied on retrospective self-reported lifetime psychiatric diagnoses. Misclassification of MD and PTSD contributes to measurement error, resulting in an underestimate of the role of additive genetic factors and an overestimate of the role of individual-specific environmental factors in etiology. Thus, the contribution of genetic influences to the association between MD and PTSD in this study is likely to be an underestimate. Finally, our data are based on the DSM-III-R and results may not be the same under DMS-IV.
Our finding of a substantial common genetic liability to MD and PTSD has implications for theory, research, and practice. A common genetic liability to MD and PTSD is consistent with proposals for a quantitative-hierarchical approach to classification in DSM-V whereby PTSD is grouped with MD (and GAD) under the subcategory of internalizing-distress disorders(Watson, 2005). These findings also support R. Krueger’s view that research on the etiology of psychiatric disorders will benefit from focusing on core processes underlying multiple forms of psychopathology rather than on discrete disorders.(Krueger, 1999; Krueger et al., 2005) In practical terms, this means investigators interested in identifying causal genetic risk factors for common psychiatric disorders may benefit from using comorbidity to identify subtypes of disorder with a common etiology. Gene-hunters focused on PTSD need to carefully consider comorbidity in selecting controls for genetic studies. Given the MD-PTSD genetic overlap, the presence of MD in controls will attenuate an investigator’s ability to detect a gene-PTSD association. Gene-hunting studies may benefit from distinguishing between comorbid MD-PTSD versus PTSD or MD-only in trauma-exposed samples. Finally, our data suggest that most of the environmental risk factors for MD and PTSD are disorder-specific. Prevention efforts will benefit from research aimed at identifying the environmental conditions that differentially shape their development in the context of common genetic liability.
Acknowledgments
Numerous organizations have provided invaluable assistance in the conduct of this study, including: Department of Defense; National Personnel Records Center, National Archives and Records Administration; the Internal Revenue Service; National Opinion Research Center; National Research Council, National Academy of Sciences; the Institute for Survey Research, Temple University. Most importantly, the authors gratefully acknowledge the continued cooperation and participation of the members of the VET Registry and their families. Without their contribution this research would not have been possible.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Binder EB, Salyakina D, Lichtner P, Wochnik GM, Ising M, Putz B, Papiol S, Seaman S, Lucae S, Kohli MA, Nickel T, Kunzel HE, Fuchs B, Majer M, Pfennig A, Kern N, Brunner J, Modell S, Baghai T, Deiml T, Zill P, Bondy B, Rupprecht R, Messer T, Kohnlein O, Dabitz H, Bruckl T, Muller N, Pfister H, Lieb R, Mueller JC, Lohmussaar E, Strom TM, Bettecken T, Meitinger T, Uhr M, Rein T, Holsboer F, Muller-Myhsok B. Polymorphisms in FKBP5 are associated with increased recurrence of depressive episodes and rapid response to antidepressant treatment. Nat Genet. 2004;36:1319–1325. doi: 10.1038/ng1479. [DOI] [PubMed] [Google Scholar]
- Breslau N, Davis G, Andreski P, Federman B, Anthony JC. Adversity, stress, and psychopathology. University Press; London, Oxford: 1998. Epidemiological findings on posttraumatic stress disorder and co-morbid disorders in the general population; pp. 319–328. [Google Scholar]
- Breslau N, Davis GC, Andreski P. Risk factors for PTSD-related traumatic events: A prospective analysis. Am J Psychiatry. 1995;152:529–535. doi: 10.1176/ajp.152.4.529. [DOI] [PubMed] [Google Scholar]
- Breslau N, Davis GC, Peterson EL, Schultz LR. A second look at comorbidity in victims of trauma: The posttraumatic stress disorder-major depression connection. Biol Psychiatry. 2000;48:902–909. doi: 10.1016/s0006-3223(00)00933-1. [DOI] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Sage Publications; Newbury Park: 1993. [Google Scholar]
- Caspi A, Moffitt TE. Gene-environment interactions in psychiatry: joining forces with neuroscience. Nat Rev Neurosci. 2006;7:583–590. doi: 10.1038/nrn1925. [DOI] [PubMed] [Google Scholar]
- Chantarujikapong SI, Scherrer JF, Xian H, Eisen SA, Lyons MJ, Goldberg J, Tsuang M, True WR. A twin study of generalized anxiety disorder symptoms, panic disorder symptoms and post-traumatic stress disorder in men. Psychiatry Res. 2001;103:133–145. doi: 10.1016/s0165-1781(01)00285-2. [DOI] [PubMed] [Google Scholar]
- Dilsaver SC, Akiskal HS, Akiskal KK, Benazzi F. Dose-response relationship between number of comorbid anxiety disorders in adolescent bipolar/unipolar disorders, and psychosis, suicidality, substance abuse and familiality. J Affect Disord. 2006;96:249–258. doi: 10.1016/j.jad.2006.07.008. [DOI] [PubMed] [Google Scholar]
- Eisen S, Neuman R, Goldberg J, Rice J, True WR. Determining zygosity in the Vietnam Era Twin Registry: An approach using questionnaires. Clin Genet. 1989;35:423–432. doi: 10.1111/j.1399-0004.1989.tb02967.x. [DOI] [PubMed] [Google Scholar]
- Eley TC, Stevenson J. Specific life events and chronic experiences differentially associated with depression and anxiety in young twins. J Abnorm Child Psychol. 2000;28:383–394. doi: 10.1023/a:1005173127117. [DOI] [PubMed] [Google Scholar]
- Fu Q, Heath AC, Bucholz KK, Nelson E, Goldberg J, Lyons MJ, True WR, Jacob T, Tsuang MT, Eisen SA. Shared genetic risk of major depression, alcohol dependence, and marijuana dependence. Arch Gen Psychiatry. 2002;59:1125–1132. doi: 10.1001/archpsyc.59.12.1125. [DOI] [PubMed] [Google Scholar]
- Henderson W, Eisen S, Goldberg J, True WR, Barnes JT, Vitek ME. Vietnam Twin Registry: A resource for medical research. Public Health Report. 1990;105:368–373. [PMC free article] [PubMed] [Google Scholar]
- Hettema JM, Neale MC, Myers JM, Prescott CA, Kendler KS. A population-based twin study of the relationship between neuroticism and internalizing disorders. Am J Psychiatry. 2006;163:857–864. doi: 10.1176/ajp.2006.163.5.857. [DOI] [PubMed] [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indices in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Jang KL, Livesley WJ, Vernon PA. Heritability of the big five personality dimensions and their facets: a twin study. J Pers. 1996;64:577–591. doi: 10.1111/j.1467-6494.1996.tb00522.x. [DOI] [PubMed] [Google Scholar]
- Kendler KS. Major depression and generalized anxiety disorder. Same genes, (partly)different environments--revisited. Br J Psychiatry Suppl. 1996:68–75. [PubMed] [Google Scholar]
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52:1048–1060. doi: 10.1001/archpsyc.1995.03950240066012. [DOI] [PubMed] [Google Scholar]
- Khan AA, Jacobson KC, Gardner CO, Prescott CA, Kendler KS. Personality and comorbidity of common psychiatric disorders. Br J Psychiatry. 2005;186:190–196. doi: 10.1192/bjp.186.3.190. [DOI] [PubMed] [Google Scholar]
- Kilpatrick DG, Koenen KC, Ruggiero KJ, Acierno R, Galea S, Resnick HS, Roitzsch J, Boyle J, Gelernter J. Serotonin transporter gene and social support moderate PTSD and depression in hurricane-exposed adults. doi: 10.1176/appi.ajp.2007.06122007. Under Review. [DOI] [PubMed] [Google Scholar]
- Koenen KC, Harney R, Lyons MJ, Wolfe J, Simpson JC, Goldberg J, Eisen SA, Tsuang M. A twin registry study of familial and individual risk factors for trauma exposure and posttraumatic stress disorder. J Nerv Ment Dis. 2002;190:209–218. doi: 10.1097/00005053-200204000-00001. [DOI] [PubMed] [Google Scholar]
- Koenen KC, Lyons MJ, Goldberg J, Simpson J, Williams WM, Toomey R, Eisen SA, True W, Cloitre M, Wolfe J, Tsaung MT. A high risk twin study of combat-related PTSD comorbidity. Twin Res. 2003;6:218–226. doi: 10.1375/136905203765693870. [DOI] [PubMed] [Google Scholar]
- Koenen KC, Saxe G, Purcell S, Smoller JW, Bartholomew D, Miller A, Hall E, Kaplow J, Bosquet M, Moulton S, Baldwin C. Polymorphisms in FKBP5 are associated with peritraumatic dissociation in medically injured children. Mol Psychiatry. 2005 doi: 10.1038/sj.mp.4001727. [DOI] [PubMed] [Google Scholar]
- Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry. 1999;56:921–926. doi: 10.1001/archpsyc.56.10.921. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Watson D, Barlow DH. Introduction to the special section: toward a dimensionally based taxonomy of psychopathology. J Abnorm Psychol. 2005;114:491–493. doi: 10.1037/0021-843X.114.4.491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee HJ, Lee MS, Kang RH, Kim H, Kim SD, Kee BS, Kim YH, Kim YK, Kim JB, Yeon BK, Oh KS, Oh BH, Yoon JS, Lee C, Jung HY, Chee IS, Paik IH. Influence of the serotonin transporter promoter gene polymorphism on susceptibility to posttraumatic stress disorder. Depress Anxiety. 2005;21:135–139. doi: 10.1002/da.20064. [DOI] [PubMed] [Google Scholar]
- Lyons MJ, Eisen SA, Goldberg J, True W, Lin N, Meyer JM, Toomey R, Faraone SV, Merla-Ramos M, Tsuang MT. A registry-based twin study of depression in men. Arch Gen Psychiatry. 1998;55:468–472. doi: 10.1001/archpsyc.55.5.468. [DOI] [PubMed] [Google Scholar]
- Muthen LK, Muthen BO. Mplus Version 3.11. Muthen & Muthen; Los Angeles, CA: 2004. [Google Scholar]
- Neale MC, Boker SM, Xie G, Maes H. Mx: statistical modeling. Department of Psychiatry; VCU Box 900126, Richmond, VA 23298: 2002. [Google Scholar]
- Neria Y, Bromet EJ. Comorbidity of PTSD and depression: Linked or separate incidence. Biol Psychiatry. 2000;48:878–880. doi: 10.1016/s0006-3223(00)01012-x. [DOI] [PubMed] [Google Scholar]
- Orsillo SM, Weathers FW, Litz BT, Steinberg HR, Huska JA, Keane TM. Current and lifetime psychiatric disorders among veterans with war zone-related posttraumatic stress disorder. J Nerv Ment Dis. 1996;184:307–313. doi: 10.1097/00005053-199605000-00007. [DOI] [PubMed] [Google Scholar]
- Plomin R, DeFries JC, McClearn GE, McGuffin P. Behavioral Genetics. Worth Publishers; New York: 2001. [Google Scholar]
- Prescott CA. Using the Mplus computer program to estimate models for continuous and categorical data from twins. Behav Genet. 2004;34:17–40. doi: 10.1023/B:BEGE.0000009474.97649.2f. [DOI] [PubMed] [Google Scholar]
- Robins LN, Helzer JE, Cottler L, Golding E. National Institute of Mental Health Diagnostic Interview Schedule Version III - Revised. Department of Psychiatry; Washington University, St. Louis, MO: 1988. [Google Scholar]
- True WJ, Rice J, Eisen SA, Heath AC, Goldberg J, Lyons MJ, Nowak J. A twin study of genetic and environmental contributions to liability for posttraumatic stress symptoms. Arch Gen Psychiatry. 1993;50:257–264. doi: 10.1001/archpsyc.1993.01820160019002. [DOI] [PubMed] [Google Scholar]
- Tsuang MT, Bar JL, Harley RM, Lyons MJ. The Harvard Twin Study of Substance Abuse: what we have learned. Harv Rev Psychiatry. 2001;9:267–279. [PubMed] [Google Scholar]
- Watson D. Rethinking the mood and anxiety disorders: a quantitative hierarchical model for DSM-V. J Abnorm Psychol. 2005;114:522–536. doi: 10.1037/0021-843X.114.4.522. [DOI] [PubMed] [Google Scholar]
- Xian H, Chantarujikapong SI, Shrerrer JF, Eisen SA, Lyons MJ, Goldberg J, Tsuang M, True W. Genetic and environmental influences on posttraumatic stress disorder, alcohol, and drug dependence in twin pairs. Drug Alcohol Depend. 2000;61:95–102. doi: 10.1016/s0376-8716(00)00127-7. [DOI] [PubMed] [Google Scholar]