

Mesothelioma, defined here to include all cancers specified as mesothelioma or with a primary-site pleura, is rare and has a high fatality rate (Box 1). Exposure to asbestos is the most common cause of mesothelioma: more than 80% of men with mesothelioma were likely exposed to asbestos in the workplace.1 Workplace exposure to asbestos continues in Canada, primarily in the mining and construction sectors.
Box 1.
The number of Canadian men who receive a diagnosis of mesothelioma each year has been steadily increasing over the past 20 years, from 153 cases in 1984 to 344 cases in 2003 (Figure 1). The number of cases is likely underestimated owing to diagnostic, coding and registration challenges specific to mesothelioma.5 The annual incidence rate has also risen from 1.4 to 2.1 per 100 000. Cases are not restricted to specific provinces but occur throughout the country. Mesothelioma is generally not diagnosed until 30 or more years after the first exposure; thus, cases are largely the result of asbestos exposure in the 1950s, 1960s and 1970s.
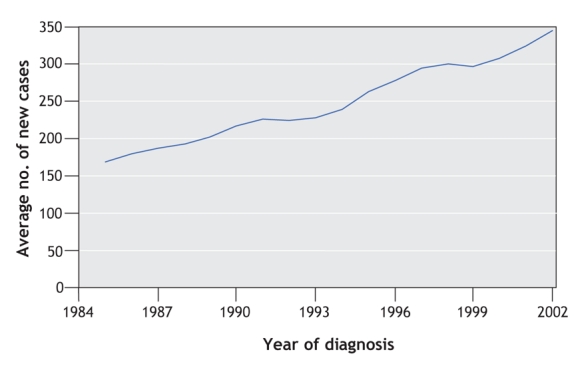
Figure 1: New cases of mesothelioma in men in Canada from 1984 to 2003. Sources: National Cancer Incidence Reporting System (1984–1991) and the Canadian Cancer Registry (1992–2003).
Mesothelioma is less common among women (78 diagnoses in Canada in 2003, representing 18% of all new cases of mesothelioma diagnosed in that year), and the percentage of women with recognized occupational exposure is smaller.1 Family members of people who work with asbestos and people exposed to asbestos-containing products in the home or who live close to asbestos facilities are at increased risk for mesothelioma.2
Asbestos is also a lung carcinogen, and there are about 2 asbestos-related cases of lung cancer for every mesothelioma.3 Recently, the Institute of Medicine in the United States concluded that asbestos is a risk factor for laryngeal cancer and that asbestos may increase the risk of pharynx, stomach and colorectal cancers.4 Thus, the true burden of asbestos-related cancer extends beyond mesothelioma.
Most asbestos exposure in Canada occurred in the mining and milling, manufacturing and construction sectors, although smaller numbers of workers may have been exposed in a wide variety of other industries. The decline in domestic production and consumption of asbestos in recent decades has meant that fewer mining and manufacturing workers have been exposed. Construction workers, however, have the potential for continued exposure during the maintenance, renovation and demolition of buildings that contain asbestos. Thus, it is not clear when the annual number of mesothelioma cases will begin to decline. Many developed countries have banned the use of asbestos, although construction workers may still be exposed. Incidence rates for pleural mesothelioma in Sweden, one of the first countries to institute a ban on asbestos, have plateaued.6 Canada continues to be a major exporter of asbestos to countries where adequate surveillance of exposure and disease may be lacking.
Mesothelioma and lung cancer are generally recognized as compensable by workers' compensation boards if workplace asbestos exposure can be documented, although there may be conditions around duration or latency. However, only about one-third of those with a diagnosis of mesothelioma receive compensation, probably because the majority do not file a claim.7–9 Adjudication of claims for other potentially asbestos-related cancers differs by province, and it is likely that a smaller proportion of these cancers result in a claim.
What can medical practitioners do?
• A workplace-exposure history should be taken for all patients with a diagnosis of mesothelioma or lung cancer to determine if they may have been exposed to asbestos. If so, patients should be encouraged to investigate their eligibility for compensation.
• Workers exposed to asbestos should be counselled to cease smoking in order to reduce their risk for lung cancer.
Loraine D. Marrett PhD Cancer Care Ontario Toronto, Ont. Larry F. Ellison MSc Statistics Canada Ottawa, Ont. Dagny Dryer MD PEI Cancer Treatment Centre and Cancer Registry Charlottetown, PEI
Key points of the article
• Mesothelioma is usually associated with workplace exposure to asbestos.
• Canada still produces asbestos and exports it to developing countries.
• In addition to miners, construction workers continue to be exposed today.
• The number of men diagnosed each year with mesothelioma is rising.
• Only about one-third of patients with mesothelioma receive workers' compensation.
• Physicians can help patients or their families determine if they may be eligible for compensation.
For more information:
• www.awcbc.org or your local workers' compensation board for policies and procedures
Acknowledgments
The following people assisted the steering committee in developing this material: Ms. Erin Pichora, Cancer Care Ontario; Dr. Paul Demers, University of British Columbia; Mr. Larry Stoffman, National Committee on Environmental and Occupational Exposures (Primary Prevention Action Group of the Canadian Partnership Against Cancer); Dr. Jim Brophy, Occupational Health Clinics for Ontario Workers Inc.
Footnotes
The steering committee for Canadian Cancer Statistics is a committee of the National Cancer Institute of Canada responsible for the annual production of Canadian Cancer Statistics. Membership is described in Canadian Cancer Statistics 2007 (available at www.cancer.ca).
Questions about the data provided in the Canadian Cancer Statistics at a Glance series should be addressed to the chair of the steering committee for Canadian Cancer Statistics by writing: stats@cancer.ca.
For the National Cancer Institute of Canada's steering committee for Canadian Cancer Statistics
Competing interests: None declared.
REFERENCES
- 1.Goldberg M, Ibernon E, Rolland P, et al. The French national mesothelioma surveillance program. Occup Environ Med 2006; 63:390-5. [DOI] [PMC free article] [PubMed]
- 2.Bourdes V, Boffetta P, Pisani P. Environmental exposure to asbestos and risk of pleural mesothelioma: review and meta-analysis. Eur J Epidemiol 2000; 16:411-7. [DOI] [PubMed]
- 3.Henderson DW, Rodelsperger K, Woitowitz HJ, et al. After Helsinki: a multidisciplinary review of the relationship between asbestos exposure and lung cancer, with emphasis on studies published during 1997–2004. Pathology 2004; 36:517-50. [DOI] [PubMed]
- 4.Institute of Medicine. Asbestos: selected cancers. Washington: National Academies Press; 2006. [PubMed]
- 5.Robinson BW, Musk AW, Lake RA. Malignant mesothelioma. Lancet 2005; 366:397-408. [DOI] [PubMed]
- 6.Hemminki K, Hussain S. Mesothelioma incidence has leveled off in Sweden. Int J Cancer 2008;122: 1200-1. [DOI] [PubMed]
- 7.Waller B, Marrett L. The occupational cancer research and surveillance project. Toronto: Cancer Care Ontario and the Workplace Safety & Insurance Board; 2006. Available: www.cancercare.on.ca/documents/Occupreport2006.pdf (accessed 2008 Feb 12).
- 8.Subcommittee on the Epidemiology of Asbestos-related Diseases in Quebec. The epidemiology of asbestos-related diseases in Quebec. Institut national de santé publique du Québec; 2004. p. 47–8.
- 9.Kirkham T, Demers P, McLeod C, et al. Factors related to compensation of mesothelioma in British Columbia [poster presentation]. Scientific Committee on Epidemiology in Occupational Health meeting; 2007 October 9-12: Banff, Alberta.