

Abstract
From 1990 to 2005 our department treated nine patients with chronic radial head dislocation by an ulnar osteotomy and indirect reduction by interosseous membrane. The patients varied in age from 2 years and 8 months to 10 years, and the time from the injury to operation ranged from 40 days to 3 years. The range of functional motion and carrying angle was restored in all nine patients, and no complications, such as recurrent dislocation, infection, or neurovascular injury were observed. This technique has proven to be a successful approach to treating such cases, with a low range of complications and good functional results.
Résumé
De 1990 à 2005 nous avons traité 9 patients, agés de 2 ans 8 mois à 10 ans, d’une luxation permanente de la tête radiale par une ostéotomie cubitale avec réduction indirecte par la membrane inter-osseuse. Le délai entre le traumatisme et la chirurgie était de 40 jours à 3 ans. L’amplitude de mobilité et l’axe du coude étaient restaurés dans tous les cas sans complication à déplorer. Les auteurs sont satisfaits de cette technique.
Introduction
Bado, in 1967, classified Monteggia fracture-dislocations into four types according to location, direction of ulna angulation, and position of the dislocated radial head [1]. Type I fracture-dislocation with anterior radial head and ulna angulation is the most frequently seen type in children [10]. In the acute phase conservative treatment is the best choice, as long as ulna length is restored and maintained so that a stable reduction of the radial head dislocation is indirectly acquired. This may be achieved by immobilisation in a cast or intramedullary percutaneous osteosynthesis of the ulna. However, controversy exists with respect to treatment in the late phase, that is, 30 days after the initial lesion [3, 10, 16]. While some experts advocate that the radial head be maintained in the dislocated state [14, 15], or that it be removed at skeletal maturity, in the event of pain and functional limitation [4, 17], others propose open reduction, as over time flexion deformity and progressive valgus of the elbow, pain and limitation of elbow and forearm movement may occur [3, 12]. Several open reduction techniques have been proposed for the treatment of neglected Monteggia fractures-dislocations, including reduction of radial head dislocation with reconstruction of the annular ligament [3, 12], reduction of radial head dislocation accompanied by osteotomy of radial shortening [13], reduction of the radial head with ulna osteotomy at the initial deformity location [10], or at the proximal metaphysis of the ulna [4, 8].
In our department, we believe that correction of the shortening and angular deformity of the ulna is fundamental to obtaining stable reduction of the dislocation of the radial head. In support of this, we present nine patients treated by this procedure Fig. 1.
Fig. 1.

(Case number 09): preoperative and final postoperative X–rays
Patients and methods
Nine patients – seven girls and two boys, with ages ranging from 2 to 10 years – were treated in our department between 1990–2005 following diagnoses of neglected Monteggia’s fracture dislocation (eight cases) and radial head dislocation due an proximal ulnar osteochondroma (one case) (Table 1). None of the patients required immediate attention due to pain but rather as a consequence of limitation of flexion and deformity of the elbow due to valgus and anterior radial head prominence. All of the patients were treated surgically using the same technique, as described below.
Table 1.
Presentation of the patients
| Case/patient | Age | Interval between the trauma and the surgery | Classificationa |
|---|---|---|---|
| 1 | 5 years | 1 year, 5 months | I |
| 2 | 4 years, 5 months | 1 year | I |
| 3 | 2 years, 8 months | 2 months | I |
| 4 | 10 years | 40 days | I |
| 5 | 4 years | 3 years | Anterior dislocation due to an ulnar osteocondroma |
| 6 | 2 years, 9 months | 1 year, 2 months | I |
| 7 | 8 years | 60 days | I |
| 8 | 3 years | 10 months | I |
| 9 | 6 years | 18 months | I |
aBado, J.L. [1]
The patients were placed in a supine position with the elbow semi-flexed and the forearm pronated on a conventional surgical table. Tourniquet use was optional. The elbow joint was first accessed using the Boyd approach [6] (cases 1 and 2) and the Kocher approach [11] (cases 3–9), and all dense fibrous tissue interposed between the radial head and the capitulum of humerus was removed Fig. 2. A transverse osteotomy of the proximal metaphysis of the ulna was then performed using the same incision; this was posteriorly displaced to achieve reduction of the radial head through traction of the interosseous membrane. The magnitude of the triangular wedge to be opened in the dorsal aspect of the ulna was determined by the surgeon as that required to obtain and maintain radial head reduction Fig. 3. The angulation produced was in the opposite direction of the radial head displacement, and the gap was maintained using a molded semi-tubular plate AO-ASIF and fixed with screws. In none of the patients was it necessary to reconstruct the annular ligament [16]. A 2.0-mm smooth Kirschner wire was inserted in a transcapitellar manner to maintain the radial head reduction for 3 weeks Figs. 4 and 5.
Fig. 2.

Fibrous tissue between radial head and capitellum (arrow)
Fig. 3.
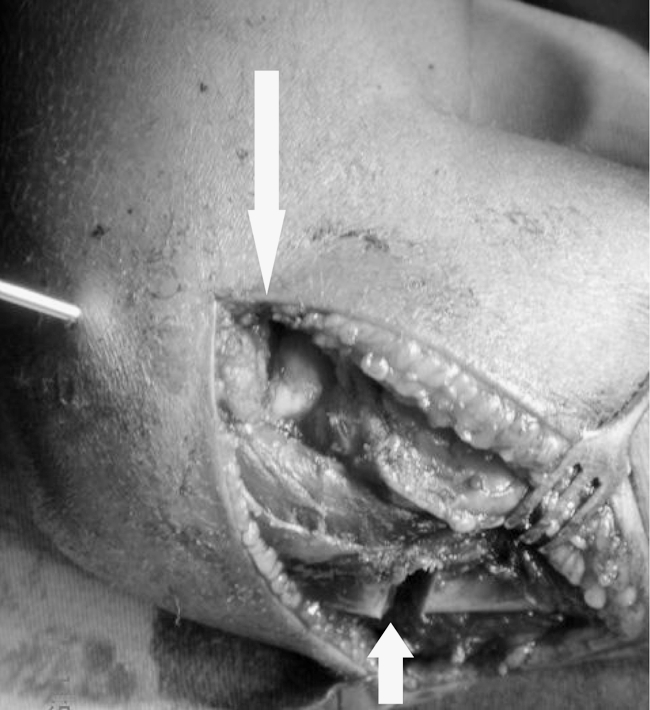
Ulnar open wedge osteotomy (short arrow) after radial head reduction (long arrow)
Fig. 4.

Radial head reduction and transcapitellar fixation (image intensifier control)
Fig. 5.

Ulnar osteotomy fixed with plate and screws
In patient 5, the first step was resection of an osteochondroma; this was followed by open reduction of the radial head with ulnar osteotomy as described above.
During the postoperative period all of the patients were immobilised by means of a long-arm cast for 6 weeks, after which exercises to improve flexion, extension, pronation and supination were begun.
Results
No surgical problems were encountered, and the surgical and postoperative procedures were well tolerated by the nine patients. All patients are asymptomatic, with a reduced radial head and a good range of movement, after a minimum and maximum follow-up period of 22 months and 12 years, respectively (Table 2).
Table 2.
Postoperative outcome
| Case/patient | Follow-up | Carrying angle | Elbow flexo extension | Pronation-supination of the forearm |
|---|---|---|---|---|
| 1 | 8 years | 8° valgus | 135/0° | 70/90° |
| 2 | 12 years | 4° valgus | 135/0° | 80/90° |
| 3 | 5 years | 8° valgus | 135/0° | 90/90° |
| 4 | 3 years | 11° valgus | 135/0° | 60/90 |
| 5 | 3 years | 7° valgus | 135/0° | 60/90° |
| 6 | 2 years | 10° valgus | 135/0° | 70/90° |
| 7 | 2 years | 7° valgus | 135/0° | 80/90° |
| 8 | 2 years | 8° valgus | 135/0° | 90/90° |
| 9 | 22 months | 7° valgus | 135/0° | 70/80° |
Discussion
The technique described here is recommended for the treatment of chronic radial head dislocation in children. This may occur as a consequence of the greater bone plasticity of the ulna, which may be deformed without fractures or present late deformity in apparently reduced fractures [10, 18].
The treatment of neglegted Monteggia fracture-dislocation in children is still open to controversy. The first question often raised is for how long may a neglected dislocation be accepted as being reversible before the secondary adaptive changes disrupt the end result. This interval ranges – depending on the author – from 6 months to 6 years [5, 10]. Another important point with respect to achieving a good functional outcome is the maximum age of the patient undergoing potential bone remodelling. Three of the patients reported here were over 10 years at the time of surgery, with the oldest being 12 years of age [7, 9].
In our group of patients, the age at the time of the surgical procedure ranged from 2 years and 8 months to 10 years, while the time elapsed between the initial trauma, diagnosis and surgery ranged from 40 days to 3 years.
Another point that is often raised is the choice of surgical technique used in the treatment of these lesions. Some authors recommend an open reduction of the radial head either with or without reconstruction of the annular ligament, combined or not with osteotomy of the radius or ulna lengthening (at the apex of deformity or at proximal metaphysis) and with or without internal ulna fixation and transcapitellar fixation of radial head [2, 3, 10, 12, 16].
The results of this study support the use of surgical treatment of neglected radial head dislocation in children and accord with recent results published by other authors [3, 10, 16]. Indirect reduction of the radial head through ulna osteotomy is the treatment of choice for these lesions in children. Discussion about the location of the osteotomy, whether it is at the proximal metaphysis or at the place of deformity of the ulna, is irrelevant, as once some time has elapsed, it may not be possible to detect the initial location of the deformity. Internal fixation using a plate and screw is essential to maintain reduction until the full consolidation of ulna osteotomy. Resection of the radial head should be reserved only for symptomatic cases in patients more advanced in years as an absolute exception, following skeletal maturation.
Conclusions
Chronic radial head dislocation presents progressive flexion and valgus, and decreased range of motion. The treatment of this lesion should be done by indirect reduction of the radial head through the interosseous membrane with an ulnar osteotomy angled in the opposite direction of the initial radial head dislocation and fixed with plate and screws.
References
- 1.Bado JL (1967) The Monteggia lesion. Clin Orthop 50:71–86 [PubMed]
- 2.Bell Tawse AJS (1965) The treatment of Malunited Anterior Monteggia Fractures in children. J Bone Joint Surg 47B:718–723 [PubMed]
- 3.Best TN, Orth AF (1994) Management of old unreduced Monteggia fracture dislocations of the elbow in children. J Pediatr Orthop 2:193–198 [DOI] [PubMed]
- 4.Bouyala JM, Chestrian P, ramaherison P (1978) L’osteotomie haute du cubitus dans le traitment de la luxations anterieure residuelle après fracture de Monteggia. Chir Pediatr 19:201–203 [PubMed]
- 5.Blount WP (1954) Fractures in children. Baltimore, Williams and Wilkins
- 6.Boyd HS, Boals JC (1969) The Monteggia lesion: a review of 159 cases. Clin Orthop 66:94–100 [PubMed]
- 7.Freedman L, Luk K, Leong JCY (1988) Radial head reduction after a missed Monteggia fracture. J Bone Joint Surg 70B:846–847 [DOI] [PubMed]
- 8.Hirayama T, Takemitsu Y, Yagihara K, Mikita A (1987) Operation for chronic dislocation of the radial head in children. J Bone Joint Surg 69B 4:639–642 [DOI] [PubMed]
- 9.Hurst LC, Dubrow EN (1983) Surgical treatment of symptomatic chronic radial head dislocation: a neglected Monteggia fracture. J Pediatr Orthop 3:227–230 [DOI] [PubMed]
- 10.Kalamchi A (1986) Monteggia fracture-dislocation in children: late treatment in two cases. J Bone Joint 68A:615–619 [PubMed]
- 11.Kocher J (1987) Lateral approach. In: Campbell´s operative orthopaedics, 7th edn. St. Louis, Mosby, p 92
- 12.Lloyd-Roberts GC, Bucknill TM (1977) Anterior dislocation of the radial head in children. Aetiology, natural history and management. J Bone Joint Surg 59B 4:402–407 [DOI] [PubMed]
- 13.McFarland B (1936) Congenital dislocation of the head of the radius. Br J Surg 24:41–49 [DOI]
- 14.Pollen AG (1973) Fractures and dislocations in children. Churchill-Livingstone, Edinburgh
- 15.Stelling FH, Cote RH (1956) Traumatic dislocation of head of radius in children. J Am Med Assn 160:732–736 [DOI] [PubMed]
- 16.Stoll TM, Willis BR, Paterson DC (1992) Treatment of missed Monteggia fracture in the child. J Bone Joint Surg 74B:436–440 [DOI] [PubMed]
- 17.Watson-Jones R (1955) Fractures and joint injuries, vol 2, 4th edn. E and S Livingstone, Edinburgh
- 18.Wright PR (1963) Greenstick fracture of the upper end of the ulna with dislocation of the radio-humeral joint or displacement of the superior radial epiphysis. J Bone Joint Surg 45B:727–731 [PubMed]