

Abstract
Urinary exosomes are excreted from all nephron segments, and may serve as biomarkers for classifying renal diseases. Isolation of urinary exosomes by the established ultracentrifugation method has some limitations for use in a clinical laboratory. We sought a rapid and simple way to obtain urinary exosomes. We used a commercially available nanomembrane concentrator to enrich exosomes from urine by centrifugation at 3000 × g for 10–30 min. Urinary exosomal markers, TSG101, AQP2, NES, Annexin V, ACE, and podocalyxin (PODXL) were recovered from the nanomembrane concentrator and detected by western blotting, and typical features of urinary vesicles were found by electron microscopy. Exosomal markers were detected in as little as 0.5 ml of urine. By the nanomembrane method exosomal proteins could be recovered from urine samples frozen at −80°C or refrigerated overnight at 4°C then stored at −80°C. By enriching exosomes we could detect PODXL, a podocyte marker, which decreased by 71% in 5 male patients with focal segmental glomerulosclerosis (FSGS) and abundant proteinuria. We conclude that 1) use of a nanomembrane concentrator simplifies and accelerates the enrichment of urinary exosomes; 2) the nanomembrane concentrator can concentrate exosomal proteins from clinical urine samples. This enhanced method may accelerate the translation of urinary exosomal biomarkers from bench to bedside for the diagnosis, classification, and prognostication of renal diseases.
Keywords: urinary exosomes, nanomembrane concentrator, ultracentrifugation, biomarkers
New urinary biomarkers will likely speed up the development of new treatments for renal diseases(2). Exosomes containing membrane and cytosolic proteins are shed into the urine from all nephron segments, and may be altered in abundance or physical properties in association with various kidney diseases. Pisitkun et al. isolated exosomes from fresh human urine by ultracentrifugation(5). Our previous studies demonstrated optimal collection, storage, and preservation conditions for exosomes from human urine(7). Urinary exosomal Fetuin-A and Na+/H+ exchanger isoform 3 (NHE3) are increased in patients with acute kidney injury (AKI)(1, 6). Thus, urinary exosomes may provide an avenue for the discovery and/or validation of biomarkers for early diagnosis, classification, and monitoring treatment of kidney diseases(4). However, the ultracentrifugation step limits the assay throughput because of a prolonged 1–2 hr of ultracentrifugation and a small number of slots in the rotor. Therefore, we sought an exosome isolation method that would be more suitable for a typical clinical laboratory. Commercially available Nanomembrane concentrators are manufactured with a narrow, well-defined molecular pore size distribution and therefore the molecular size cutoffs are relatively precise. Proteins can be concentrated in excess of 100-fold, soluble protein recoveries can approach 95%, and samples are typically concentrated within 10–30 min. We evaluated a nanomembrane concentrator with a polyethersulfone membrane and a uniform pore size of 13 nm. The aim of this study was to determine whether nanomembranes can efficiently isolate urinary exosomes with <100 nm diameter rapidly from human urine and whether this method can be applied to patients with chronic kidney diseases (CKD) with abundant proteinuria.
MATERIALS AND METHODS
Urine collection
All human urine samples were collected and processed as described previously (Research Study No. 00-DK-0107 & 06-DK-0020)(7), except that freshly voided spot urine samples (15 ml) from patients with FSGS were centrifuged at 1000 × g for 10 min then stored at −80°C for 1–13 month/s until use, and protease inhibitors were added immediately after thawing. Some urine samples from the healthy volunteer were stored at three different conditions: 4°C for 1 hr, −80°C for 1 week, and refrigerated at 4°C for 24 hr and then stored at −80°C for 1 week. Urine creatinine was measured by creatinine companion (Exocell Inc., PA, USA).
Preparation of Urinary Exosomes by Nanomembrane Concentrator
Nanomembrane concentrators (Vivaspin 500, $3 for each 500 ul of tube; Vivaspin 4, $4 for each 4 ml of tube or Vivaspin 20, $8 for 20 ml of each tube; Sartorius Inc., Goettingen, Germany) were washed to remove glycerol and other preservatives by adding approximately one volume of PBS buffer then centrifugation at 3,000 × g at room temperature (RT) before processing urine samples. After centrifugation of urine samples at 17,000 × g at 4 ºC for 15 min, 0.5 ml, 1.5 ml or 10 ml of urine supernatant was added to a Vivaspin 500, 4, or 20, respectively, nanomembrane concentrator and then centrifuged at 3,000 × g at 20°C for 10–30 min. The urine proteins were recovered from the nanomembrane concentrator by two methods: 1) A combined retentate (CR) was recovered by adding an equal volume of unheated 2X solublizing buffer to the retentate while still in the concentrator and shaking at RT for 30 min, or 2) sequentially recovering the proteins not bound to the nanomembrane and adhering proteins: the retentate (R) was removed from the concentrator before adding an equal volume of the pre-heated (95°C) 2X solublizing buffer (2X Laemmli buffer with 400 mM dithiotheritol (DTT)); the nanomembrane was subsequently washed to remove remaining proteins that adhered to the nanomembrane by adding two volumes of pre-heated 1X solublizing buffer (HSW) into the concentrator and shaking the concentrator at RT for 10 min (Fig. 1). Urine exosomal proteins isolated by ultracentrifugation (200,000 × g pellets) described previously(7) were used as positive controls. The combined retentate (CR) method was used to isolate from the urine of 9 patients (male=5, female=4) with FSGS and 8 normal control volunteers (male=4, female=4). All of the urinary protein samples were stored at −80°C until use.
Figure 1. The isolation of urinary exosomes by nanomembrane concentrator.

Urinary exosomes were isolated from 10 ml, 1.5 ml or 0.5 ml urine samples by the nanomembrane concentrator as described in methods.
Gel electrophoresis and Western blotting
An equal proportion of the original urine volume was loaded onto gels, except for patient urine samples, which were first normalized by urine creatinine (Ucr). The protein samples were analyzed using gel electrophoresis and detected by Coommasie-Blue staining or western blotting as described previously (7). Specific antibodies were used in western blot analysis: tumor susceptibility gene (TSG101), aquaporin 2 (AQP2), neuron specific enolase (NES) (7); polyclonal antibodies to angiotensin-converting enzyme (ACE) (1:1000); monoclonal antibodies to annexin V (1:250) (Abcam, Cambridge, MA, USA) and podocalyxin (PODXL) (1:100) (Alpha Diagnostics, San Antonio, TX, USA). The density of the bands was quantified by NIH ImageJ software.
Electron Microscopy
Exosomal suspensions were mixed 1:1 with 4% paraformaldehyde. This mixture was applied to a 200-mesh nickel grid and washed in 1X PBS solution followed by sterile H2O. The nickel mesh was negatively stained with 0.5% uranyl acetate and visualized using a JEOL 1200 EX electron microscope operated between 60 kV.
Statistical analysis
All data are expressed as mean ± SEM. Differences between groups were analyzed for statistical significance by t-test. A P-value <0.05 was accepted as statistically significant.
RESULTS
Isolation of urinary exosomes by nanomembrane concentrator
To test whether a nanomembrane concentrator can isolate the exosomes from human urine, we compared the efficiency of the nanomembrane concentrator with the standard ultracentrifugation method. Starting with 10 ml of fresh human urine, “fractions” from two recovery protocols (see Methods) were recovered from the concentrator, and 5 typical urinary exosome markers (TSG101, AQP2, NES, Annexin V, and PODXL) were detected by western blotting. The recovery of TSG101 and AQP2 from the retentate alone (R) was poor, consistent with some exosomes containing these proteins adhering to the nanomembrane. However, the recovery of TSG101 and AQP2 was improved by washing the nanomembrane with heated, SDS containing buffer (HSW). The recovery of NES, Annexin V, and PODXL in the combined retentate (CR) was the same as by ultracentrifugation. In addition, 5 exosomal proteins were not detected in the flow-through of the nanomembrane concentrator (Fig. 2), indicating that leakage of exosomes or exosome fragments through the device was insignificant.
Figure 2. Efficiency of urinary exosome isolation by nanomembrane concentrator.

Ten ml of normal human fresh urine samples processed by nanomembrane concentrator. An equal proportion was loaded in each lane, and western blots were performed for TSG101, AQP-2, NSE, Annexin V, and PODXL. Lane 1: 200,000 × g pellets as exosome positive controls; lane 2: combined retentate (CR); lane 3: nanomembrane flowthrough was ultracentrifuged (200,000 × g 1 hr); lane 4: retentate (R); lane 5: proteins remaining on the nanomembrane after retentate was removed and washed with heated SDS-containing wash (HSW) buffer.
Electron microscopy verified a typical saucer shape with bi-layer morphology of urinary vesicles retained by the nanomembrane concentrator (Fig. 3A). The feature and size distribution were very similar to vesicles isolated using ultracentrifugation (Fig. 3B).
Figure 3. Electron microscopy of urinary vesicles.
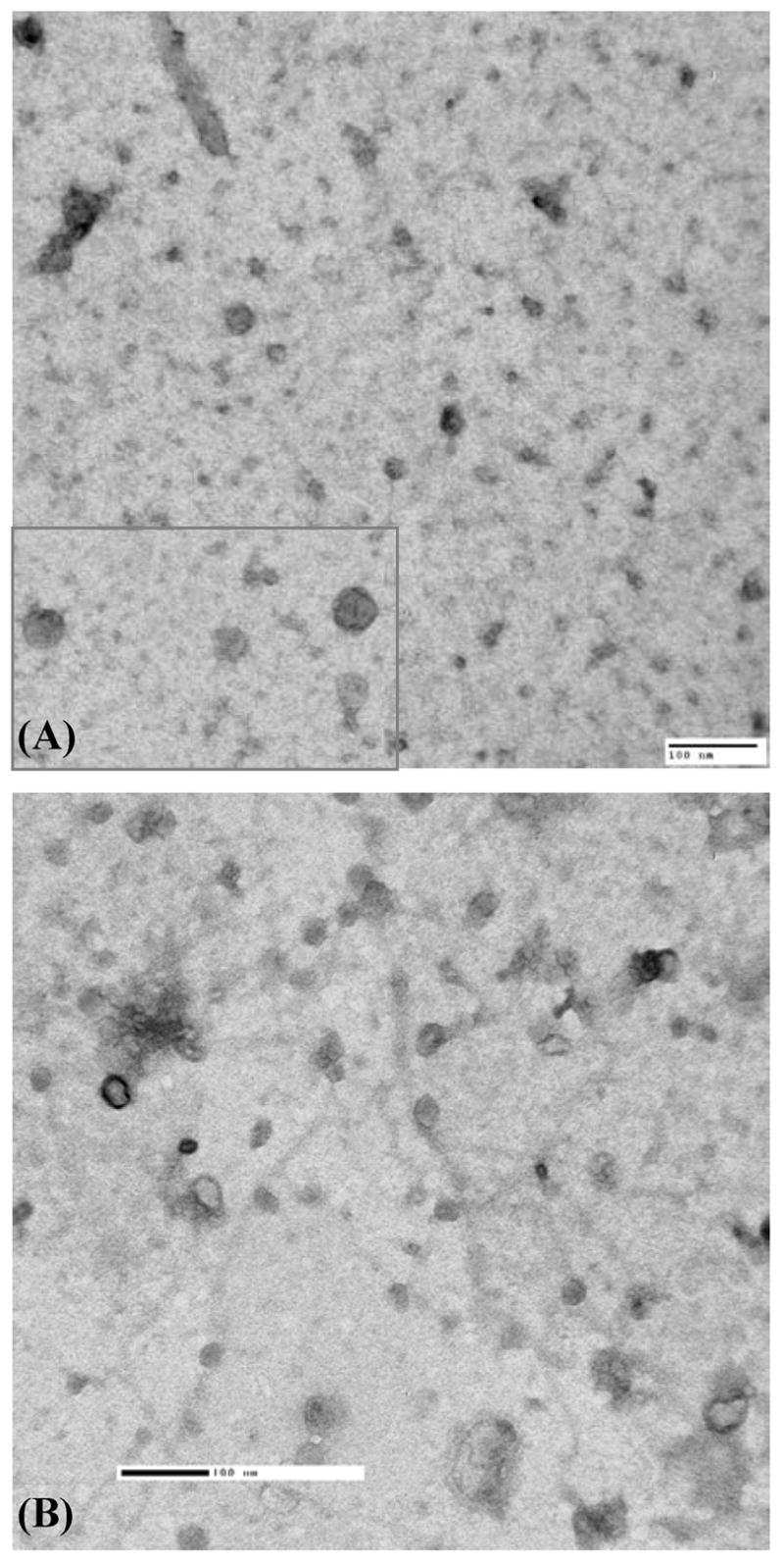
Urinary vesicles obtained by nanomembrane concentrator (A) and differential ultracentrifugation (B). Black bar denotes 100 nm.
We determined the reproducibility by analyzing a single urine sample in 6 individual nanomembrane concentrators. TSG101, AQP2, ACE and PODXL were reproducibly detected with an average coefficient of variation of 7% (Supplementary Fig. 1).
The lower limit of urine sample volume to isolate urinary exosomes by nanomembrane
To determine whether nanomembrane concentrators can be used for small sample volumes typically collected from oliguric patients or stored in clinical archives, we processed 0.5 ml or 1.5 ml of urine. TSG101, AQP2, and NES were detected by western blotting from 0.5 ml or 1.5 ml urine samples (Fig. 4).
Figure 4. Isolation of exosomal proteins from a small urine volume by nanomembrane concentrator.
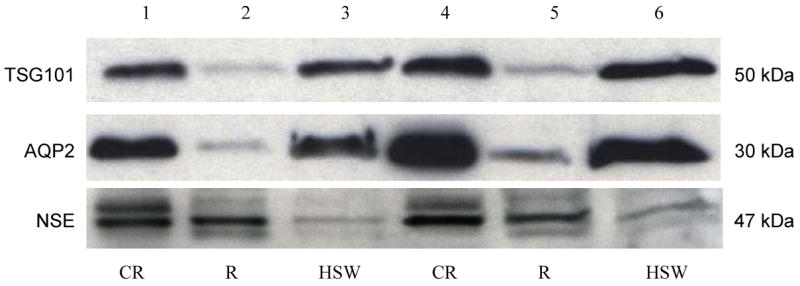
Fresh urine samples (0.5 or 1.5 ml) were processed by nanomembrane, proteins were recovered (CR, R, and HSW indicated in Figure 1), and western blots were performed for TSG101, AQP2, and NSE. Lane 1–3: 0.5 ml of urine and lane 4–6:1.5 ml of urine.
Effect of initial storage conditions on exosome recovery by nanomembrane
We next determined whether nanomembrane concentrators can be used on urine samples that were stored frozen or shipped on ice from a distant clinic to a central analysis laboratory and then stored at −80°C. We compared the effects of our nanomembrane method on urinary exosomes under three storage conditions (see Methods) after urine collection. We found that four exosomal proteins TSG101, AQP2, ACE and PODXL were detected by western blotting in each urine sample, whether stored at −80°C or placed on wet ice for 24 hr and then stored at −80°C. The recoveries were not significantly different from fresh urine processed within 1 hr (Fig. 5). Total protein patterns were similar in all three conditions (Supplementary Fig. 2).
Figure 5. Effect of storage on urinary exosomal proteins isolated by nanomembrane concentrator.

Urine sample from one healthy volunteer was processed in three storage conditions, within 1 hr (lane 1–3); stored at −80°C (lane 4–6); refrigerated at 4°C for 24 hr and then stored at −80°C (lane 7–9) after collection. Urinary proteins (CR, R, and HSW indicated in Figure 1) were analyzed by western blotting of TSG 101, AQP2, ACE, and PODXL. High molecular weight (HMW) and low molecular weight (LMW) isoforms of ACE are shown.
Detection of a candidate biomarker in the urine of FSGS patients
To verify whether nanomembrane concentrators could help detect potential biomarkers of urinary exosomal proteins for specific kidney diseases, we isolated exosomal proteins from urine samples from patients with focal segmental glomerulosclerosis (FSGS) and normal control volunteers to isolate urinary exosomal proteins. Urinary podocalyxin (PODXL), a known apical membrane protein marker for podocytes, decreased significantly from 24 ± 7 to 7 ± 2 density units (p<0.05) in male FSGS patients compared to normal, age-matched males. Female FSGS patients also had lower levels of urinary PODXL compared to age-matched female volunteers (29 ± 11 vs 22 ± 8), but the difference was not statistically significant (Fig. 6).
Figure 6. PODXL in patients with FSGS isolated by nanomembrane concentrator.

Urine samples were obtained from 9 patients with FSGS and 8 healthy normal volunteers. Urinary PODXL by western blotting in the urinary proteins from the combined retentate. The amount of proteins was normalized by urine creatinine before loading onto the gels.
DISCUSSION
This study demonstrates that 1) the nanomembrane concentrator can isolate urinary exosomes as effectively as the standard ultracentrifugation method; 2) can be used on very small urine samples (0.5 ml); 3) urinary exosomal proteins were stable when they were stored at −80°C or refrigerated at 4°C 24 hrs and then stored at −80°C; 4) some exosomal proteins adhered to the nanomembrane but could be recovered by washing with heated solublizing buffer; 5) nanomembrane concentrators can be used for urine samples from patients despite abundant proteinuria.
Urinary exosomes derive from all cell types that face the urinary space including glomerular podocytes, renal tubule cells, and cells lining the urinary drainage system(5). A previous study by Pisitkun et al.(5) detected distinct 295 proteins in normal human urinary exosomes, including multiple proteins associated with renal and systemic diseases. Our recent study verified that Fetuin-A increased in urinary exosomes in early phase of AKI in rats after nephrotoxin injection or ischemia and reperfusion and also increased in ICU patients with AKI(6). Du Cheyron et al.(1) reported that urinary membrane-associated NHE3, which was found in urinary exosomes in our previous study(7), increases in patients with AKI. These findings suggest that urinary exosomes can serve as a source for biomarker discovery to improve early diagnosis, classification, choice of therapeutic approach, and assessment of prognosis for kidney diseases. However, the need for ultracentrifugation, the current method of exosome isolation, limits the application of urinary exosomes in a clinical laboratory. The ultracentrifuge rotor limits the number and volume of urine samples that can be processed; and several hours are needed to process each large volume of urine sample. A rapid and simple method to isolate urinary exosomes is necessary for exosomal markers to be routinely detected in a clinical laboratory.
Exosomes are small internal vesicles (<100 nm) of multivesicular bodies (MVB) that are delivered to the extracellular fluid by fusion of the outer membrane of MVB with the apical plasma membrane (3, 5). Exosomes can be isolated from solid phase components by differential ultracentrifugation based on their very low density. The nanomembrane concentrator is made of the polyethersulfone membrane with a uniform pore size of 13 nm and an approximate 100kDa molecular weight cut off. The concentrator is designed with two opposing membranes in a “V-shape” to minimize the effect of shearing forces during the centrifugation. We hypothesized that the concentrator should retain the majority of urinary exosomes and allow most of soluble urine proteins (<100 kDa), such as albumin, globulin and microglobulin to pass through the nanomembrane. The concentration procedure can be performed within 30 min using a common tabletop centrifuge. For typical clinical urine samples (<8 ml), the processing time is almost the same for both nanomembrane concentrator and ultracentrifugation methods. Preparation of exosomes from large volume urine samples (100 ml, for example) take 4 hrs to prepare by ultracentrifugation compared to 30 mins using nanomembrane concentrators (assuming the samples is processed with 5 nanomembrane concentrators, then the retenates are pooled). Using typical rotors, the maximum ultrafiltration rate is 960 ml/hour for the nanomembrane concentrator and 96 ml/hour by ultracentrifugation. However, the final volume of the concentrated protein can be set by the investigator with the ultracentrifugation method, but is fixed at about 0.2 ml per nanomembrane concentrator.
We selected several exosome markers including integral membrane proteins (AQP2, ACE, and PODXL), soluble cytoplasmic proteins (NES and Annexin V), and a peripheral membrane protein TSG101. These proteins were detected after concentration from fresh urine samples ranging in size from 0.5 to 10 ml, but also from the urine samples frozen at −80 ºC or refrigerated at 4 ºC for 24 hrs and then stored at −80 ºC. None of the exosomal proteins were detected in the flowthrough fraction, indicating quantitative retention. These findings suggest that nanomembrane concentrators may be used for urinary exosome studies using urine samples with very small volumes (oliguric AKI), small urine aliquots (0.5–1.0 ml) stored at −80 ºC or samples shipped on wet ice from a distant clinical site.
Some proteins such as NSE, Annexin V, and PODXL did not adhere to the nanomembrane and were readily recovered. Other exosomal proteins, AQP2 and TSG101, adhered to the nanomembrane, as only a small proportion could be recovered from the retentate. However, we found that using the heated solubilizing buffer more effectively stripped AQP2 and TSG101 from the nanomembrane. We speculate that heterogeneity in the exosome population may account for the efficiency of extraction from the nanomembrane concentrator. It is also possible vesicles containing AQP2 and TSG101 have a smaller diameter that can be trapped in the nanomembrane pores during centrifugation. Alternatively, the composition (phosphorylated and/or glycosylated proteins) of some exosome subpopulations may promote adhesion to the nanomembrane. Therefore, isolation conditions must be optimized for maximal recovery of each exosomal protein. Prewashing of the nanomembrane is strongly recommended, as additives such as glycerol increase the variability of exosomal protein recovery (data not shown).
Finally, PODXL, a membrane protein marker for podocytes, was isolated from urine samples of FSGS patients using the nanomembrane concentrator. Exosomal PODXL was decreased significantly in FSGS patients with 2.2 to 15 g/day of proteinuria. This suggests that nanomembranes can enrich urinary exosomes from the urine samples from chronic kidney diseases with abundant proteinuria, such as diabetic nephropathy, lupus nephritis, and nephritic syndrome, etc.
CONCLUSION
Urinary exosomes can be rapidly enriched from human urine using a nanomembrane concentrator. This new approach can enrich exosomal proteins from small urine volumes (0.5 ml), samples stored at −80°C, or samples refrigerated first and then stored at −80°C. This makes it feasible to store urine samples or ship refrigerated urine from distant clinic sites. Nanomembranes may be useful to more rapidly isolate potential urinary exosomal biomarkers in clinical samples, accelerating the translation of urinary exosomal biomarkers from laboratory bench to clinical laboratory.
Supplementary Material
Acknowledgments
This research was supported by the Intramural Research Program of NIH, NIDDK and NHLBI.
References
- 1.du Cheyron D, Daubin C, Poggioli J, Ramakers M, Houillier P, Charbonneau P, Paillard M. Urinary measurement of Na+/H+ exchanger isoform 3 (NHE3) protein as new marker of tubule injury in critically ill patients with ARF. Am J Kidney Dis. 2003;42:497–506. doi: 10.1016/s0272-6386(03)00744-3. [DOI] [PubMed] [Google Scholar]
- 2.Hewitt SM, Dear J, Star RA. Discovery of protein biomarkers for renal diseases. J Am Soc Nephrol. 2004;15:1677–1689. doi: 10.1097/01.asn.0000129114.92265.32. [DOI] [PubMed] [Google Scholar]
- 3.Johnstone RM, Adam M, Hammond JR, Orr L, Turbide C. Vesicle formation during reticulocyte maturation. Association of plasma membrane activities with released vesicles (exosomes) J Biol Chem. 1987;262:9412–9420. [PubMed] [Google Scholar]
- 4.Pisitkun T, Johnstone R, Knepper MA. Discovery of urinary biomarkers. Mol Cell Proteomics. 2006 doi: 10.1074/mcp.R600004-MCP200. [DOI] [PubMed] [Google Scholar]
- 5.Pisitkun T, Shen RF, Knepper MA. Identification and proteomic profiling of exosomes in human urine. Proc Natl Acad Sci U S A. 2004;101:13368–13373. doi: 10.1073/pnas.0403453101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhou H, Pisitkun T, Aponte A, Yuen PS, Hoffert JD, Yasuda H, Hu X, Chawla L, Shen RF, Knepper MA, Star RA. Exosomal Fetuin-A identified by proteomics: a novel urinary biomarker for detecting acute kidney injury. Kidney Int. doi: 10.1038/sj.ki.5001874. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhou H, Yuen PS, Pisitkun T, Gonzales PA, Yasuda H, Dear JW, Gross P, Knepper MA, Star RA. Collection, storage, preservation, and normalization of human urinary exosomes for biomarker discovery. Kidney Int. 2006;69:1471–1476. doi: 10.1038/sj.ki.5000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.