

Abstract
In spite of serious under-financing during the Pinochet years, Chile's public health system remains the backbone of health provision, responsible for the impressive public health status.
Summary Points.
The Chilean health system underwent a drastic neoliberal reform in the 1980s, with the creation of a dual system: public and private health insurance and public and private provision of health services.
This reform served as a model for later World Bank–inspired reforms in countries like Colombia.
The private part of the Chilean health system, including private insurers and private providers, is highly inefficient and has decreased solidarity between rich and poor, sick and healthy, and young and old.
In spite of serious underfinancing during the Pinochet years, the public health component remains the backbone of the system and is responsible for the good health status of the Chilean population.
The Chilean health reform has lessons for other countries in Latin America and elsewhere: privatisation of health insurance services may not have the expected results according to neoliberal doctrine. On the contrary, it may increase unfairness in financing and inequitable access to quality care.
The Chilean health system has been studied extensively [1]. Its current form is the result of a major reform undertaken by the Pinochet government following the coup d'état in 1973. Pinochet's reform established competition between public and private health insurers and promoted private health services, following neoliberal principles. Neoliberalism is an economic and political movement that gained consensus in the 1980s among international organisations like the International Monetary Fund and the World Bank. This movement demands reforms such as free trade, privatisation of previously public-owned enterprises, goods, and services, undistorted market prices, and limited government intervention. After the publication of the World Bank's 1993 report, “Investing in Health” [2], Chile became a model for neoliberal reforms to health services.
In this Policy Forum, we assess the effects of the Chilean reform from Pinochet until 2005, and including the transition to democracy in 1990. We suggest that the use of Chile as a model for other countries of the health benefits of neoliberalism is seriously misguided. We stress the dominant role of the public health system in Chile, while most other studies have assessed the introduction of a private insurance sector as part of the neoliberal reform. Revisiting the Chilean health reform after 25 years, we come to new conclusions that could be important for countries such as Ecuador and Bolivia, which are preparing health reforms, and even for the United States, with its current debate on universal health insurance.
Pinochet's Reform and Its Context
Chile has been a social laboratory, having experienced democratic liberalism (1958–1964), Christian Democratic reformism (1964–1970), democratic socialism (1970–1973), neoliberal authoritarianism (1973–1989), and three democratic coalition governments from 1990 to the present (see Glossary for definitions) [3]. The neoliberal reforms were not limited to the health system, but were also made to the pension system, in education, and through the privatisation of state industries. Many of the changes in the health system were later conceptualised in World Bank–supported documents [4].
Glossary.
Christian Democratic reformism: political parties based on Christian principles in a democratic regime; reformist as opposed to revolutionary. In many European countries, Christian democrats have alternated in government with socialists. In Chile, the Frei administration, from 1964 till 1970.
Democratic liberalism: in a democratic regime, a free or “liberal” market with little state intervention (in fact, orthodox conservative economics). Not to be confused with “liberal arts” or left-wing liberal democrats. In Chile, the Alessandri government from 1958 till 1964.
Democratic socialism: regimes based on democracy and socialist principles like equity and solidarity; found in many European countries, such as Sweden. In Chile, the Allende Popular Unity government from 1970 till 1973
Neoliberal authoritarianism: orthodox neoliberalism combined with dictatorship. Neoliberalism demands reforms such as free trade, privatisation of previously public-owned enterprises, goods, and services, undistorted market prices, and limited government intervention. In Chile, the Pinochet regime from 1973 till 1989.
In 1979, after having brutally repressed opposition to the 1973 coup against socialist president Salvador Allende, the Pinochet regime embarked on a sweeping health sector reform, based on neoliberal doctrines [5–7]. A private health insurance system, ISAPRES, was developed alongside the state system and was intended to be the dominant one. The two systems followed completely different rationales: the public system, a traditional “Bismarckian” social security system (members contribute a proportion of their wages to receive health services according to their need), promoted solidarity via risk-sharing and the internal redistribution of health care resources, while the private system offered health insurance policies corresponding to each individual's contributions.
A National Health Fund (FONASA) was created in 1979 as a public agency to collect and manage the financial resources coming from the compulsory contributions of employees who chose to remain in the public system (or who could not afford an adequate plan with an ISAPRES company), and from the national government's health budget. There are four categories of insured within FONASA; A, indigent; B, very low income; C, lower-middle income; and D, higher-middle income. Categories B, C, and D are entitled to choose health care outside the public provider system, with varying levels of co-payment. Category A members are limited to public services, both for primary care and hospital services.
The private system, ISAPRES, was created in 1981 to manage the payroll contributions allocated to health care for those opting out of the state system. The private companies purchased most care from the private sector [8], which received an intense boost. The ISAPRES market offered no fewer than 8,000 different individual plans, designed according to sex, age, health risk, supplementary premiums, and co-payments. The market concentrated on relatively affluent clients with lower health risks: the mean income of ISAPRES members in 2003 was more than four times higher than FONASA members [9]. The profit margins of ISAPRES exceeded 20% [10].
The National Health Service was decentralised into 26 autonomous territorial health authorities. These entities took over responsibility for hospital care, while primary health care facilities were transferred to municipalities. The funding of public health services was drastically reduced [11]. Consequently, the supply of health care in public facilities was restricted.
In March 1990, a coalition of centre and left-wing parties came to power and has won all the elections ever since. Its social policy has been broadly “social democratic”, seeking to attach a Western-style welfare state to a dynamic emerging market economy [12]. In the same year (1990), a government regulatory agency, known as the ISAPRES Superintendency, was created to establish some sort of regulation of ISAPRES. As Figures 1 and 2 show, public expenditure on health increased dramatically from 1990 [13], to almost three times more in constant pesos. While the proportion of public expenditure on health remained fairly stable at around 3%, from a low of 2% in 1976, economic growth explains the increase in absolute numbers. Private expenditure remained stable as a proportion of gross domestic product, but increased sharply in absolute numbers. To finance this increased public expenditure, a tax reform was approved that reversed the tax reductions of the Pinochet years [5,14,15].
Figure 1. Public Expenditure on Health in Chile, 1970–2000 (Pesos 2000).

As the graph shows, there was a sharp increase in public health expenditure (in 2000 Chilean pesos) in Chile after 1990, with social democratic governments. A short spike can be observed during the socialist Allende government. The lower darker line represents public expenditure, the upper lighter one public expenditure per person. From [13].
Figure 2. Health Expenditure in Chile, 1970–2004, as a Percentage of Gross Domestic Product.

As a percentage of gross domestic product, public health expenditure rose under the Allende government, then decreased sharply under the Pinochet neoliberal experiment, and is now stable at around 3%. From [13].
However, none of the main features of the Pinochet reforms described above were substantially modified [3]. More recently, President Lagos' government (2000–2006) initiated a new health reform plan (called Plan AUGE), aiming at better quality and shorter waiting times in the public sector and a minimum coverage plan in ISAPRES, but again, this policy remained broadly compatible with neoliberal reform.
The Main Features of Chile's Neoliberal Health Reform
The partial privatisation of social security.
The compulsory contributions made by workers and employees go either to the public social insurer FONASA or to one of the private health insurers of ISAPRES. During Pinochet's regime, employers were relieved of the requirement to contribute on behalf of their employees. Table 1 presents the sources of health expenditure financing for the year 2003 [11].
Table 1. Sources of Health Expenditure in Chile, 2003 (Millions of Chilean Pesos).

Out of Chile's population of some 16 million, 2.5 million of its more affluent citizens were members of private ISAPRES insurance companies in the year 1995 (this was the year in which membership in ISAPRES reached its peak, after which there was a decline). ISAPRES was legally entitled to set premiums based on individual risk factors. Although control over ISAPRES was strengthened by the creation of the Superintendency, problems remained with regard to catastrophic health expenditure for lower-income ISAPRES members. Under pressure from the Superintendency, ISAPRES decided in 2001 to cover some catastrophic conditions, but the level of the “deductible” (the amount to be paid by the patient) remained very high.
ISAPRES membership reached 26% of the population in 1995 and declined to only 16% in 2006—a small proportion of the population, and not the one most in need of health care. The decline was due to improved performance by the public sector, unemployment caused by the Asian crisis in the 1990s, the AUGE plan, and the rising cost of private health plans. Some experts estimate that by 2010, ISAPRES may cover only 10% of the population [16].
Segmentation and lack of solidarity between two parallel health insurance systems.
The ISAPRES system attracts the affluent, male, young, and urban. In the poorest quintile of the population only 1.6% are members of ISAPRES, compared with 50.5% in the richest [11]. Adult women pay up to four times more than men for their health plans, and the proportion of ISAPRES members over 60 drops dramatically since they face premiums of up to eight times as much as those of young adults. Adults over 60 are forced to enter FONASA. Some ISAPRES companies are in an oligopoly position: the main three firms share close to 80% of the market [6].
The state has subsidised ISAPRES in several ways. First, until recently it subsidised ISAPRES to the tune of 2% of the salary of those who switched from FONASA to ISAPRES. Second, it pays for maternity leave for ISAPRES members. Third, 25% of patients covered by ISAPRES receive services in public facilities because they cannot afford the co-payments [17,18]. Almost half of all catastrophic events among children of ISAPRES members are treated in public hospitals [19].
Moreover, FONASA finances the private health care sector (category B, C, and D patients can choose to be treated by private providers via a voucher system). The money transferred to the private sector in this way is substantial, greater than what is spent on municipal primary health care [20].
The return of democracy: restoring an underfinanced public sector.
The transition government inherited a series of problems with public health services from the Pinochet regime, including a major deterioration in the public infrastructure and inefficient management in the decentralised organisations [17]. Primary care services suffered from poor coordination between the regional health services and the municipal authorities. Working conditions and wages had deteriorated. Rural areas and poor urban districts were worst affected in the quantity and quality of the services provided, introducing regional differences unseen before.
From 1990 to 2002, however, tax revenues doubled and allowed for an increase in social expenditure of 240% over the same period. In 2000, expenditure on health care accounted for 7.3% of gross domestic product, 3.1% on publicly provided care and 4.2% on private care. In 2004, out-of-pocket expenditures amounted to 27% of total health expenditure.
We turn now to an assessment of the impact of the reform, focusing on equity–in terms of finance, access, and health status—and efficiency.
The Impact of the Reform: Equity
Financial equity.
Chile shares with Brazil the dubious distinction of having one of the most regressive patterns of income distribution in Latin America, and the distribution of spending on health is no exception. The private sector accounts for a disproportionate share of total health expenditure (38% of the total health expenditure was spent on 21% of the population in 2004) [9]. This is a basic unfairness, and represents a lack of solidarity, since FONASA and ISAPRES have separate financing [15].
Within the FONASA system, there is some internal redistribution between categories A–B and C-D, the latter helping to finance the health care of the former [21]. Between FONASA and ISAPRES there is some limited and indirect redistribution: ISAPRES members contribute directly to their individual health plans, but indirectly they make some contribution to the health care of the poor through the tax money received by FONASA [22], which accounts for half of its income.
Other dimensions of equity are also problematic. The ISAPRES system discriminates against women, whose participation in 2001 was only 34.4%, with lower-quality health plans than those of men [6]. Access to ISAPRES health plans depends on income, and women generally have lower incomes or are outside the remunerated workforce. Insurance policies for women of childbearing age may cost four times more than men's policies [23].
Equity of access to care.
Considering the basic inequality of Chilean society and the unfairness of its health sector financing, one would expect access to care by the poor to be unequal as well. In fact the evidence is mixed: access to care is somewhat equitable, but quality of care is not.
Some data suggest relatively equitable access. In 1999, the utilisation rate (consultations per person per year) for FONASA patients was 3.85% and for ISAPRES patients 4.12% [20]. A 2003 national health survey [24] showed that among those who reported having felt sick in the last month, 73.9% from the poorest quintile consulted with medical staff, compared with 79.7% from the richest.
But inequity may arise in the quality of health services. Frequency of surgeries and laboratory tests was positively correlated with income; more importantly, consultations with specialists were almost three times more frequent for patients in decile 10 than those in decile 1 [24]. Access to specialists appeared deficient in the public service: there were waiting lists of up to four years in some specialties, such as ophthalmology. Conversely, emergency visits were twice as frequent in the lowest income group.
There are other reasons to believe that access is inequitable. Utilisation rates differ greatly between poor and rich municipalities: for primary care, by a factor of 2.8, for emergencies by a factor of 3.9, and for inpatients, by a factor of 2.0 [25].
The 2003 CASEN survey mentioned earlier [24] indicated that only 57.5% of FONASA members described their health as good or very good, compared with 80.6% of ISAPRES members. This should be reflected in higher utilisation rates for FONASA members, but as we have seen, the reverse is the case.
Equity of health status.
The Chilean model of development has been associated with rapid economic growth: gross national product increased 7.9% per annum in the 1990s [17]. The country is ranked 22nd on the Global Competitiveness Index [26], far ahead of any other Latin American country, and 37th in the 2003 Human Development Report, although its development model has created high social inequality. In fact, inequality continued to increase even under the democratic post-Pinochet regime (Table 2).
Table 2. Percentage of Total Income per Decile, 1969–2000.
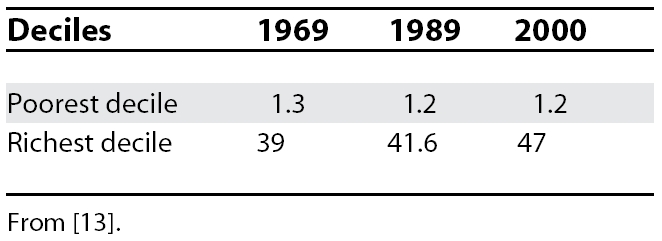
Poverty (defined as being below the poverty line, determined annually for individuals and families) was sharply reduced under the democratic governments, declining from 45% in 1985 to 21.7% in 1998 [27] and 13.7 % in 2006 [28]. But income inequality rose, making Chile “the paladin [champion] of inequality” in the harsh words of Parada [29]. Before 1970, Chile's GINI index (a measure of income inequality on a scale of 0 to 100, where 0 is complete income equality and 100 is complete inequality) was under 45; in the 1980s, it jumped to 65. In 2003 it was 57.5, a very unfavourable figure compared with, for instance, Costa Rica's figure of 45.9. The richest 20% received 17 times more income than the poorest 20% [27]; for comparison, in the US this group received 8.9 times more and in Peru 10.5 times more than the poorest 20%.
In spite of this inequality, Chile's average health indicators are good, with high life expectancy and low infant and maternal mortality, even with 27.3% of children under 10 living in poverty in 2003 [24]. The relatively equitable access to health care probably played a significant role in this achievement, as did maternal and child protection programmes, carried out by the public sector. Still, the number of potential productive years of life lost is much higher in the poorest quintile of 20–79-year-olds in Santiago, 35% higher than in the richest quintile [30].
Another study suggests health inequities between municipalities: the tuberculosis incidence maximum/minimum ratio between municipalities was 5.53, and for child malnutrition it was 5.00 [25]. The national department of epidemiology states that adjusted mortality for the poorest decile is 6.0 out of 1,000, versus 4.8 for the richest [31].
The Impact of the Reform: Efficiency
Here the evidence is clearer. ISAPRES has hardly contained costs, and the ISAPRES companies never intended to do so: they have few incentives to be efficient buyers of health services for their clients. Instead, they work hard to be efficient in the selection of their clients (they are allowed to refuse clients). Their focus is on low-risk, high-income patients, with the goal of making a profit. They spend ten times as much on administration per member [9] and about two times as much on health care per member than FONASA (Figure 3), even though ISAPRES members are in better health and need less care [4]. To deliver care, ISAPRES companies rely on a burgeoning private sector, reimbursed on a fee-for-service basis, which induces an increased supply of unnecessary but profitable services.
Figure 3. Expenditure per Member, FONASA and ISAPRES, 1984–2002.

The graph shows that per capita expenditure was always much higher in ISAPRES than in FONASA, and the difference has expanded in the past years. From [13].
Discussion
Chile's health indicators are good, compared with countries with a similar gross national product, such as Colombia and Argentina. These results are due in part to Chile's high economic growth rate and a spectacular reduction in poverty [12,28,32]. Further significant factors are the high proportion of the population with access to drinking water and sanitation, and the high adult literacy rate and education level. But relatively equitable access to health care, mainly through public health insurance and public health services, which cover 80% of the population, played a major role in this achievement, as did maternity and child health protection programmes implemented through the public health network.
The democratic regime did not modify the essence of Pinochet's health reform. Key features such as social security privatisation and the purchaser–provider split persisted. But public health expenditure was sharply increased to improve infrastructure, hire more personnel, and provide better equipment and salaries. The ISAPRES companies were placed under the control of a government regulatory agency to avoid commercial excesses.
As for the role that health care has played in achieving Chile's favourable health indicators, a key conclusion from the foregoing analysis must be that results rested on the backbone of the public health system, which the neoliberal reforms were willing, but not able, to break. It is absolutely clear that the country's health indicators are not due to the superior access to health care enjoyed by the better-off minority, who in any case continued to rely significantly on the public system for many conditions and services. ISAPRES private health insurance never covered more than 25% of the population, and this proportion is now declining, thanks to a remarkable improvement in public health services. Even during the Pinochet regime the Chilean system was basically a public system, accessible to the 75% of Chileans who could not afford private insurance with ISAPRES. The effects of the neoliberal health reform in Chile remain marginal.
The neoliberal health reform in Chile has created an unfair dual health system: FONASA and public services for the poor, ISAPRES and private services for the more affluent section of the population. ISAPRES now accounts for 40% of total health expenditure, on behalf of 16% of the population. The reform increased the incomes of private sector providers and decreased health system efficiency (through the incentive to over-treat inherent to fee-for-service payment, through much higher administration and marketing costs, and through the fragmentation of service provision).
To present the Chilean reform as a model to be followed by other countries, as has been done by the World Bank and other international bodies, is to disregard the evidence, which tends to show that Chile's relatively successful health care provision has been achieved in spite of the reform, not because of it, or in fact because the intended neoliberal reform could not be implemented as foreseen. Another neoliberal reform, modified to avoid the segmentation that occurred in Chile, can be observed in Colombia, and the results are not encouraging [10,33].
A logical recommendation for a health system counter-reform in Chile would be to move from a multi-insurer scheme to a single public insurer scheme, as in Costa Rica. This single payer (and its members) would then still be able to choose between public and private providers, but with strengthened bargaining power. This would put an end to the unfairness of ISAPRES spending twice as much on their members than FONASA, although FONASA's members are a higher-risk population.
Acknowledgments
The authors wish to thank the Belgian Directorate-General for Development Cooperation for financing this research.
Footnotes
Jean-Pierre Unger and Pierre De Paepe are in the Department of Public Health, Institute of Tropical Medicine, Antwerp, Belgium. Giorgio Solimano Cantuarias and Oscar Arteaga Herrera are in the School of Public Health–Faculty of Medicine, University of Chile, Santiago, Chile.
Funding: This paper is based upon research financed by the Belgian Directorate-General for Development Cooperation (http://www.dgcd.be/). The funder played no role in the decision to submit the article or in its preparation.
Competing Interests: The authors have declared that no competing interests exist.
References
- Jack W. The evolution of health insurance institutions: theory and four examples from Latin America. 2000. Available: http://wbln0018.worldbank.org/LAC/lacinfoclient.nsf/27cc98c623e2d29b8525694c007202d7/5e9fe5ff76cd8f218525694b0065ce68?OpenDocument. Accessed 26 February 2008.
- World Bank. World Development Report 1993—Investing in health. 1993. Available: http://www-wds.worldbank.org/external/default/main?pagePK=64193027&piPK=64187937&theSitePK=523679&menuPK=64187510&searchMenuPK=64187283&siteName=WDS&entityID=000009265_3970716142319. Accessed 26 February 2008.
- Silva P. Intellectuals, technocrats and social change in Chile: past, present and future perspectives. In: Angell A, Pollack B, . The legacy of dictatorship: political, economic and social change in Pinochet's Chile. Liverpool: Institute of Latin American Studies; 2005. pp. 198–223. editors. [Google Scholar]
- Titelman D, Uthoff A. Ensayos sobre el financiamiento de la seguridad social en salud. Los casos de Estados Unidos, Canadá, Argentina, Chile, Colombia. Santiago: CEPAL-ECLAC. Fondo de Cultura Económica. Comisión Económica para América Latina y el Caribe; 2000. [Google Scholar]
- Reichard S. Ideology drives health care reforms in Chile. J Public Health Policy. 1996;17:83–98. [PubMed] [Google Scholar]
- Arteaga AM. The brutal rationale of privatisation. The Third World Institute Social Watch 2003.
- Borzutzky S. Social security privatisation: the lessons from the Chilean experience for other Latin American countries and the USA. Int J Soc Welfare. 2003;12:86–96. [Google Scholar]
- Barrientos A. Health policy in Chile: The return of the public sector. Bull Lat Am Res. 2002;21:442–459. [Google Scholar]
- Cid C, Muñoz A, Riesco X, Inostroza M. Equidad en el financiamiento de la salud y protección financiera en Chile: una descripción general. Cuadernos Médico Sociales. 2006;46:5–12. [Google Scholar]
- Homedes N, Ugalde A. Privatización de los servicios de salud: las experiencias de Chile y Costa Rica. Gaceta Sanitaria. 2002;16:54–62. doi: 10.1016/s0213-9111(02)71633-6. [DOI] [PubMed] [Google Scholar]
- Vergara Iturriaga M, Martínez Gutiérrez MS. Financiamiento del sistema de salud Chileno. Salud Publica Mex. 2005;48:1–36. doi: 10.1590/s0036-36342006000600010. [DOI] [PubMed] [Google Scholar]
- Hiscock J, Hojman D. Social policy in a fast-growing economy: the case of Chile. Soc Pol Adm. 1997;31:354–370. [Google Scholar]
- United Nations Development Programme. Chile: 20 años de esquemas liberales en protección social. 2002. Taller Interregional.
- Ffrench-Davis R. Distribución del ingreso y pobreza en Chile. In: Sáez JC, editor. Entre el neoliberalismo y el crecimiento con equidad: tres décadas de política económica en Chile. Santiago de Chile: 2003. editor. [Google Scholar]
- Vergara PO. In pursuit of “growth with equity”: the limits of Chile's free-market social reforms. Report series on the Americas. 1996. Available: http://www.hartford-hwp.com/archives/42a/030.html. Accessed 26 February 2008. [DOI] [PubMed]
- Altura Management–Diario Estrategia. 700 mil personas saldrán del sistema de Isapres en seis años. Diario Estrategia: 2004. [Google Scholar]
- Annick M. The Chilean health system: 20 years of reforms. Salud Publica Mex. 2002;44:60–68. doi: 10.1590/s0036-36342002000100009. [DOI] [PubMed] [Google Scholar]
- Larrañaga O. Eficiencia y equidad en el sistema de salud chileno. CEPAL. 1997;49:1–45. [Google Scholar]
- World Bank. Chile health insurance issues: old age and catastrophic health costs. 2000. Available: http://wbln0018.worldbank.org/lac/lacinfoclient.nsf/d29684951174975c85256735007fef12/725faf9bdb5f1c9f8525696000710527. Accessed 26 February 2008.
- Rodríguez C, Tokman MR. Resultados y rendimiento del gasto en el sector público de salud en Chile 1990-1999. Serie Financiamiento del Desarrollo, 106. Santiago de Chile: CEPAL; 2000. [Google Scholar]
- Bitrán R, Muñoz J, Aguad P, Navarrete M, Ubilla G. Equity in the financing of social security for health in Chile. Health Policy. 2000;50:171–196. doi: 10.1016/s0168-8510(99)00071-8. [DOI] [PubMed] [Google Scholar]
- Savedoff WD. Is anybody listening? Ignoring evidence in the Latin American health reform debates. Inter-American Development Bank. 2000. Available: http://www.iadb.org/sds/doc/AnyoneListening.pdf. Accessed 27 February 2008.
- Pollack M. Equidad de género en el sistema de salud chileno. Serie Financiamiento del Desarrollo, 123. Santiago de Chile: CEPAL; 2002. [Google Scholar]
- Mideplan—Gobierno de Chile. CASEN 2003, Encuesta de Caracterización socioeconómico nacional. Principales resultados en salud. Santiago de Chile: Gobierno de Chile; 2004. [Google Scholar]
- Pan American Health Organization. Información para la equidad en salud en Chile. 2001. [DOI] [PubMed]
- World Economic Forum. Global Competitiveness Index. 2005. Available: http://www.weforum.org/pdf/Global_Competitiveness_Reports/Reports/gcr_2006/gcr2006_rankings.pdf. Accessed 27 February 2008.
- Raczynski D, Serrano C. Nuevos y viejos problemas en la lucha contra la pobreza en Chile. Santiago de Chile: Asesorías para el Desarrollo; 2000. [Google Scholar]
- Mideplan—Gobierno de Chile. CASEN 2006, Encuesta de caracterización socioeconómico nacional. Principales resultados en salud. Santiago de Chile: Gobierno de Chile; 2006. [Google Scholar]
- Parada Lezcano M. Comment on book “La Transformación neoliberal del sistema de salud. Chile:1973–1990”. Cuadernos Médico Sociales. 2005;44:138–143. [Google Scholar]
- Sánchez HR, Albala CB, Lera LM. Anos de vida perdidos por muerte prematura (AVPP) en adultos del Gran Santiago. Hemos ganado con equidad. Revista Médica Chile. 2005;133:575–582. doi: 10.4067/s0034-98872005000500010. [DOI] [PubMed] [Google Scholar]
- Paz X. Mortalidad y pobreza, análisis de comunas seleccionadas. El Vigía - Boletín de Vigilancia Epidemiológica de Chile Ministerio de Salud de Chile. 1998;2:6–8. [Google Scholar]
- Arellano JPM. Políticas sociales para el crecimiento con equidad Chile 1990–2002. Serie de Estudios Socio/Económicos. 2004.
- De Groote T, De Paepe P, Unger JP. Colombia: in vivo test of health sector privatisation in the developing world. Int J Health Serv. 2005;35:125–141. doi: 10.2190/LH52-5FCB-4XDE-76CW. [DOI] [PubMed] [Google Scholar]