

Introduction
Although heightened throughout childhood and adolescence, sweet taste preference declines during late adolescence (Desor et al., 1977; Desor and Beauchamp, 1987). Despite such age-related changes in sweet preferences, individual variation, due to both genetics (Bartoshuk, 2000) and experience (Beauchamp and Moran, 1982, 1984), exists at both ends of the age spectrum (Desor et al., 1977; Beauchamp and Moran, 1982). For example, infants and teenagers of African descent preferred significantly higher levels of sucrose when compared to similarly aged Caucasians (Desor et al., 1977; Bacon et al., 1994). Moreover, experience with sugar water during infancy results in greater preference for sweet tastes during the second year of life (Beauchamp and Moran, 1984). The goal of the present study was twofold. First, we determined whether racial and ethnic differences in sweet preference are present during childhood and adulthood. Secondly, we explored whether early exposure to sweetened water modifies sweet preferences during childhood.
Materials and methods
Subjects
We tested 62 children and 55 mothers of African-American, non-Hispanic descent and 66 children and 56 mothers of non-Hispanic, European descent, hereafter referred to as Black and White, respectively. Included in this sample were 17 sibling pairs. The children ranged in age from 6 to 10 years (mean = 7.8 ± 0.1 years) and the mothers were, on average, 36.0 ± 0.6 years. Each child’s race/ethnicity was defined by mother’s report of the racial background of both herself and the biological father, according to standard US Census categories. All children and parents were racially concordant. We use the term race/ethnicity herein when describing our groups because it best represents both the genetic and cultural components of the sample (Sankar and Cho, 2002). All testing procedures were approved by the Office of Regulatory Affairs at the University of Pennsylvania and informed consent was obtained from each mother and assent from each child 7 years of age or older.
Procedures
Children and their mothers were individually tested with identical procedures to allow for comparisons. A forced-choice, paired comparison, tracking technique which avoids response bias was used to assess sucrose preferences (Cowart and Beauchamp, 1990). In brief, subjects were presented with pairs of solutions differing in sucrose concentration (0.09, 0.18, 0.35, 0.70 and 1.05M). They were asked to taste the solutions without swallowing and point to which of the pair they liked better. Each subsequent pair was then determined by the subject’s preceding preference choice. The entire task was then repeated with stimulus pairs presented in reverse order. The most preferred solution for each subject was the geometric mean of the sucrose concentrations chosen during the two trials.
Demographics, anthropometry and experience with sugar water
Mothers were queried about several socio-demographic variables and all but 20 answered questions regarding the practice of feeding sweetened water to their children when they were infants. From these latter data, two groups were formed: those who were frequently fed sweetened water and those who were never or rarely (<10 times) fed sweetened water. Children were weighed and measured for height (Detecto Model 439, Physician Scale; Webb City, MO) and body mass index (BMI, kg/m2) was computed.
Results
Demographics and anthropometry
Black mothers were significantly younger (33.6 ± 0.8 versus 38.4 ± 0.7 years) and more likely to be single (71% versus 2%), with lower household incomes and fewer years of education (13.4 ± 0.2 versus 14.8 ± 0.3 years) when compared to White mothers (all Ps < 0.001). There were significant effects of race/ethnicity on children’s age (P < 0.025); Black children were older (8.1 ± 0.2 years) than White children (7.4 ± 0.1 years). No statistical differences were observed between the two groups in the children’s BMI categories, however. Despite the various demographic and age differences between the two racial/ethnic groups, further analyses revealed that none of these measured demographic factors were significantly related to the level of sucrose preferred by either children or adults.
Sweet preferences and practice of feeding sugar water
As a group, children preferred significantly higher concentrations of sucrose than mothers [t(237 df) = 4.07, P < 0.0001]. Black children (P < 0.001) and mothers (P < 0.001) preferred significantly higher concentrations of sucrose than White children and mothers, respectively (see Figure 1). Although 38% of the Black children were routinely fed sugar water as babies, this custom was experienced by only 6% of the White children [χ2(df = 1) = 16.50, P < 0.0001]. However, regardless of race/ethinicity, early exposure to sugar water was related to the level of sucrose preferred during childhood [t(106 df) = 2.20; P = 0.03]. Children who were routinely fed sugar water during infancy preferred significantly higher levels of sucrose (0.66 ±0.07 M) when compared to those who were rarely or minimally exposed (0.48 ± 0.04 M).
Figure 1.
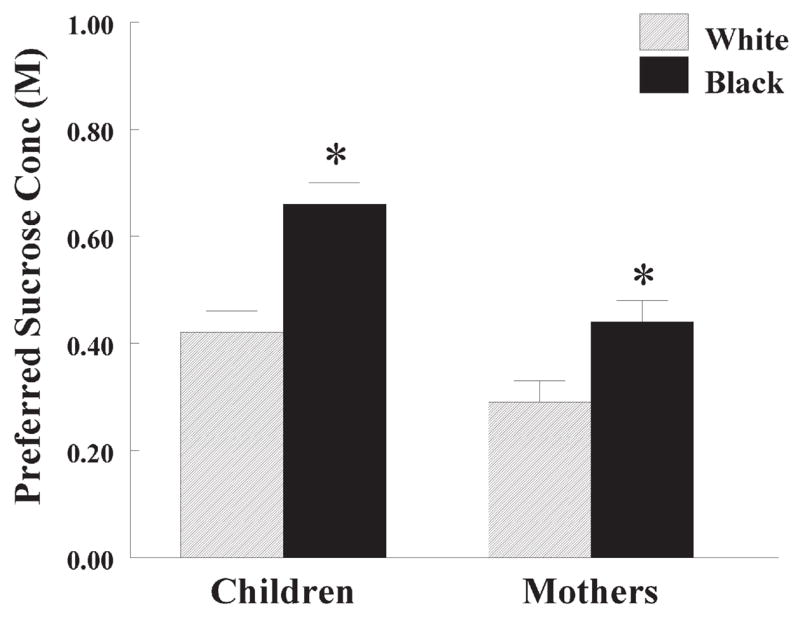
Mean (±SEM) preferred sucrose concentration (M) in Black and White children and their mothers. *Significantly different from White children and mothers, respectively.
Discussion
Consistent with previous findings in infants (Beauchamp and Moran, 1982) and adolescents (Desor et al., 1977; Bacon et al., 1994), Black children preferred significantly higher concentrations of sucrose when compared to White children. Although mothers preferred significantly lower levels of sucrose than children, similar race/ethnic differences were also observed in the adults. Several explanations, not mutually exclusive, may account for these differences.
First, demographic factors, such as income, can play a role in food availability (Drewnowski, 2003). Although the present study revealed significant socioeconomic differences between Black and White mothers, these differences were not related to the level of sucrose preferred by children or adults (see also Desor et al., 1977). However, we acknowledge that economic factors may contribute to consumer food choices since sugars, as well as fats, constitute one of the most palatable and low-priced nutrients (Drewnowski, 2003).
Secondly, experiential influences may contribute to ethnic differences in sweet preferences. The practice of feeding sugar water to infants, more evident in Black mothers, resulted in heightened sweet preferences during the second year of life (Beauchamp and Moran, 1984) and in children aged 6–10 years (present study). Likewise, the greater desire and liking for intensely sweet tasting foods and beverages in both young and elderly African-Americans (Schiffman et al., 2000) may play a role in differential exposure and ingestion to sweet tasting foods. Through familiarization, children develop a sense of what should, or should not, taste sweet (Beauchamp and Cowart, 1985).
Thirdly, the heightened preferences for sweets may be related to the physiological and analgesic properties of sugars (Blass and Hoffmeyer, 1991; Barr et al., 1994). Of interest is the recent finding that African-Americans experienced significantly higher levels of stress compared to non-Hispanic Whites (Turner and Avison, 2003). Higher levels of stress are associated with great desire for sweet tastes among young Black adults when compared to similarly aged White adults (Schiffman et al., 2000; Dallman et al., 2003). Whether African-Americans are more sensitive to the physiological effects of sweet tastes or are more likely to eat sweets to cope with stress is not yet known. Similarly, genetic variation may contribute to differences in sweet taste perception and preference (McDaniel and Reed, 2004) as well as differences in the brain mechanisms that underlie the rewarding and analgesic properties of sweet tastes.
Consistent with previous research (Desor et al., 1977; Desor and Beauchamp, 1987), children as a group preferred significantly higher levels of sucrose than adults. The study of the analgesic properties of sweet tastes and sweet taste preferences across the life span, and how it is affected by cultural practices, race/ethnicity and genetics is a research area that needs to be fully explored.
Acknowledgments
This work was supported by grant NIH AA09523 and Monell Institutional Funds.
References
- Bacon AW, Miles SJ, Schiffman SS. Effect of race on perception of fat alone and in combination with sugar. Physiol Behav. 1994;55:603–606. doi: 10.1016/0031-9384(94)90123-6. [DOI] [PubMed] [Google Scholar]
- Barr RG, Quek VS, Cousineau D, Oberlander TF, Brian JA, Young SN. Effects of intra-oral sucrose on crying, mouthing and hand–mouth contact in newborn and six-week-old infants. Dev Med Child Neurol. 1994;36:608–618. doi: 10.1111/j.1469-8749.1994.tb11898.x. [DOI] [PubMed] [Google Scholar]
- Bartoshuk LM. Comparing sensory experiences across individuals: recent psychophysical advances illuminate genetic variation in taste perception. Chem Senses. 2000;25:447–460. doi: 10.1093/chemse/25.4.447. [DOI] [PubMed] [Google Scholar]
- Beauchamp GK, Cowart BJ. Congenital and experiential factors in the development of human flavor preferences. Appetite. 1985;6:357–372. doi: 10.1016/s0195-6663(85)80004-0. [DOI] [PubMed] [Google Scholar]
- Beauchamp GK, Moran MM. Dietary experience and sweet taste preference in human infants. Appetite. 1982;3:139–152. doi: 10.1016/s0195-6663(82)80007-x. [DOI] [PubMed] [Google Scholar]
- Beauchamp GK, Moran MM. Acceptance of sweet and salty tastes in 2-year-old children. Appetite. 1984;5:291–305. doi: 10.1016/s0195-6663(84)80002-1. [DOI] [PubMed] [Google Scholar]
- Blass EM, Hoffmeyer LB. Sucrose as an analgesic for newborn infants. Pediatrics. 1991;87:215–218. [PubMed] [Google Scholar]
- Cowart BJ, Beauchamp GK. Early development of taste perception. In: McBride R, MacFie H, editors. Psychological Basis of Sensory Evaluation. Elsevier; London: 1990. pp. 1–17. [Google Scholar]
- Dallman MF, Pecoraro N, Akana SF, La Fleur SE, Gomez F, Houshyar H, Bell ME, Bhatnagar S, Laugero KD, Manalo S. Chronic stress and obesity: a new view of ‘comfort food’. Proc Natl Acad Sci USA. 2003;100:1696–1701. doi: 10.1073/pnas.1934666100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desor JA, Beauchamp GK. Longitudinal changes in sweet preferences in humans. Physiol Behav. 1987;39:639–641. doi: 10.1016/0031-9384(87)90166-1. [DOI] [PubMed] [Google Scholar]
- Desor JA, Maller O, Greene LS. Preference for sweet in humans: infants, children and adults. In: Weiffenbach JM, editor. Taste and Development: The Genesis of Sweet Preference. Government Printing Office; Washington, DC: 1977. pp. 161–173. [Google Scholar]
- Drewnowski A. Fat and sugar: An economic analysis. J Nutr. 2003;133:838S–840S. doi: 10.1093/jn/133.3.838S. [DOI] [PubMed] [Google Scholar]
- McDaniel AH, Reed DR. The human sweet tooth and its relationship to obesity. In: Moustaid-Moussa N, Berdanier C, editors. Genomics and Proteomics in Nutrition. Marcel Dekker; New York: 2004. pp. 49–67. [Google Scholar]
- Sankar P, Cho MK. Genetics. Toward a new vocabulary of human genetic variation. Science. 2002;298:1337–1338. doi: 10.1126/science.1074447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schiffman SS, Graham BG, Sattely-Miller EA, Peterson-Dancy M. Elevated and sustained desire for sweet taste in African-Americans: a potential factor in the development of obesity. Nutrition. 2000;16:886–893. doi: 10.1016/s0899-9007(00)00403-2. [DOI] [PubMed] [Google Scholar]
- Turner RJ, Avison WR. Status variations in stress exposure: implications for the interpretation of research on race, socioeconomic status, and gender. J Health Soc Behav. 2003;44:488–505. [PubMed] [Google Scholar]