

Abstract
Lowering elevated blood pressure (BP) with drug therapy reduces the risk for catastrophic fatal and nonfatal cardiovascular events such as stroke and myocardial infarction. Given the heterogeneity of hypertension as a disease, the marked variability in an individual patient’s BP response, and low response rates with monotherapy, expert groups such as the Joint National Committee (JNC) emphasize the value of combination antihypertensive regimens, noting that combinations, usually of different classes, have additive antihypertensive effects. Metoprolol succinate extended-release tablet is a beta-1 (cardio-selective) adrenoceptor-blocking agent formulated to provide controlled and predictable release of metoprolol. Hydrochlorothiazide (HCT) is a well-established diuretic and antihypertensive agent, which promotes natruresis by acting on the distal renal tubule. The pharmacokinetics, efficacy, and safety/tolerability of the antihypertensive combination tablet, metoprolol extended release hydrochlorothiazide, essentially reflect the well-described independent characteristics of each of the component agents. Not only is the combination product more effective than monotherapy with the individual components but the combination product allows a low-dose multidrug regimen as an alternative to high-dose monotherapy, thereby, minimizing the likelihood of dose-related side-effects.
Keywords: antihypertensive, blood pressure, cardiovascular disease, combination product
By treating hypertensive patients with metoprolol succinate extended release in combination with hydrochlorothiazide (metoprolol ER/HCT), the prescribing physician can expect additive antihypertensive effects. As will be illustrated in this review, the pharmacokinetics, safety, and tolerability of this antihypertensive combination essentially reflect the well-described independent characteristics of each of the component agents.
Background
For over a decade, developed counties have been facing a persistent cardiovascular public health dilemma – a substantial proportion of hypertensives remain unaware of their elevated blood pressure and of those diagnosed, many are not treated to optimal, cardiovascular risk lowering target blood pressure levels (Hajjar and Kotchen 2003; JNC-7 2003). Repeatedly, treatment guidelines and clinical trials underscore the fact that many patients require a multi-drug regimen (ALLHAT 2002; European Society of Hypertension 2003; JNC-7 2003; WHO 2003; Mourad et al 2004). Expert panels such as the Joint National Committee point out that when used in combination, antihypertensive drugs additively lower blood pressure and can often do so employing low doses of the individual agents, thereby minimizing dose-related adverse effects (JNC-7 2003; Ofili 2006). Furthermore, many antihypertensive agents complement the actions of others, particularly when they are of different classes, eg, calcium channel blockers (CCBs) and beta-blockers; and, some combinations exhibit an off-setting impact on adverse effects, eg, diuretic vs angiotensin receptor blocker effects on serum potassium (JNC-7 2003). Combination antihypertensive regimens can also “override” population-specific effects. For example, while Blacks tend to respond to renin-angiotensin system (RAS) blockade to a lesser degree than Whites, both Blacks and Whites respond equally well to diuretic/RAS inhibitor combinations (Holland and Fairchild 1982; Hawkins et al 1988; The Association of Black Cardiologists (ABC) Candesartan Study Group 2000; Papademetriou et al 2000). Moreover, the likelihood that a patient with more severely elevated blood pressure (>20/10 mmHg above goal) will attain goal with single agent treatment is so low that JNC-7 suggests initiating antihypertensive treatment for these patients with a drug-combination. The JNC panel also notes that combining anti-hypertensive drugs into a single fixed combination tablet can simplify multi-drug treatment regimens, an important consideration to facilitate patient compliance, and that fixed combinations can also be less expensive (JNC-7 2003).
Encouragingly, in recent years there has been some improvement in hypertension control rates and this has been paralleled by an increased reliance upon combination therapy. Using the National Health and Nutrition Examination Survey (NHANES), Gu et al (2006) reported that during the years 1999–2002, 62.9% of US hypertensive adults took a prescription antihypertensive medication, compared with 57.3% for the years 1988–1994. During this same time period, multiple drug use increased from 29.1% to 35.8%. Of those patients on multiple drug treatment, about one-fourth were taking a diuretic/beta-blocker combination and about one-fourth a diuretic/angiotensin converting enzyme inhibitor (ACEI) combination, while somewhat lesser proportions were taking other combinations (diuretics/CCBs, beta-blockers/CCBs, ACEIs/CCBs, etc.) (Gu et al 2006). The relatively popular use of a diuretic/beta-blocker combination is not too surprising given the established benefit of thiazides in averting the cardiovascular complications of hypertension and the potential benefit of including a beta blocker in antihypertensive regimens for patients with important comorbid illnesses such as coronary artery disease (ALLHAT 2002; JNC-7 2003; Psaty et al 2003; Turnbull et al 2003).
Formulation
Metoprolol is a beta-1 (cardioselective) adrenoreceptor-blocking agent. It was first introduced as a tartrate salt and had pharmacokinetic/pharmacodynamic properties that necessitated twice- to thrice-daily dosing. This formulation is commonly referred to as “immediate release”. Metoprolol was subsequently formulated as an extended release tablet (metoprolol ER) using the succinate salt such that 95 mg is equivalent to 100 mg of the metoprolol tartrate salt (TOPROL-XL® 2005; Sandberg et al 1988). This formulation difference resulting in different pharmacokinetic and pharmacodynamic characteristics and dosing regimens is an important distinction, as many research reports fail to specify the metoprolol formulation studied; approved indications for the formulations differ in some countries and clinical study findings have differed, depending on the formulation (TOPROL-XL® 2005).
The metoprolol ER properties are achieved by encapsulation of the succinate salt with a polymeric coating to form micro-beads, which are then embedded in a tablet matrix. In the gastrointestinal tract the beads are released from the matrix and each bead, upon exposure to fluid, allows outward diffusion of metoprolol over a period of about 20 hours (Plosker and Clissold 1992; Sandberg et al 1988; TOPROL-XL® 2005). Hydrochlorothiazide is a thiazide diuretic, typically available as a tablet formulation (Beermann et al 1976). By modifying the matrix of the metoprolol ER tablet to incorporate HCT it has been possible to develop a fixed combination tablet that allows immediate release of HCT from the matrix while retaining the extended release properties for metoprolol (data on file; Sunzel Study D4026C00005 2004).
Pharmacokinetic/pharmacodynamic properties
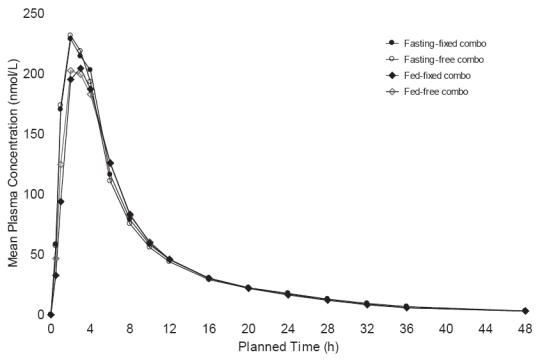
The metoprolol ER/HCT fixed combination tablet proved bioequivalent to the concomitant administration of the individual agents in single dose, cross-over studies at both metoprolol ER/HCT; 23.75/6.25 mg (low dose) and 95/12.5 mg (high dose) based both on Cmax and AUC (90% confidence intervals for the ratios within 80%–125%) (data on file: Sunzel Study D4026C00006 2005; Sunzel Study D4026C00005 2004). The high dose study was conducted with subjects fasting and fed; the pharmacokinetic parameters were nearly identical under both conditions (Figure 1 and Figure 2). The fixed tablet bioequivalence with concomitantly administered components was confirmed in a multiple dose (once daily for 5 days) study with a 100/12.5 mg tablet (data on file: Abrahamsson and Häggström Study 895 1987). In addition, the absence of a metoprolol/HCT pharmacokinetic interaction was demonstrated in a multiple dose study in which a 50/12.5 mg tablet was compared with each component administered individually, a finding that was consistent with older studies conducted with metoprolol tartrate (Jordo et al 1979). Relative to immediate release metoprolol, the extended release formulation gives plasma metoprolol concentrations that tend to be smoother, exhibiting less peak-to-trough variation. This is reflected in less variability in inhibition of exercise-induced increase in heart rate, a measure of beta-1 blockade (Darmansjah et al 1990; Sandberg et al 1990; Polsker and Clissold 1992). These extended release properties are maintained in the combination as illustrated by a study that compared the metoprolol ER/HCT combination with an immediate release combination (100/12.5 mg), ie, there was less peak to trough variability in metoprolol plasma levels with the extended release combination and the extended release formulation elicited a smoother and more sustained beta-blockade over the inter-dosing interval (90% confidence interval for the ratio of the area under the 24 hour effect curve: 105%–129%) (data on file: Abrahamsson and Häggström Study 896 1987).
Figure 1.

Mean metoprolol plasma concentration versus time curve after administration of the fixed combination tablet and the free combination of metoprolol succinate ER (1 × 95 mg) and HCT (1 × 12.5 mg) in a fasting (n = 48) and fed state (fixed; n = 48, free; n = 47): Study D4026C00005.
Figure 2.
Mean HCT plasma concentration versus time curve after administration of the fixed combination tablet and the free combination of metoprolol succinate ER (1 × 95 mg) and HCT (1 × 12.5 mg) in a fasting (n = 48) and fed state (fixed; n = 48, free; n = 47): Study D4026C00005.
Antihypertensive effects
Although first introduced as a fixed combination tablet of 100/12.5 mg (metoprolol succinate ER/HCT) in 1989 (Denmark), the antihypertensive activity of the combination over a wide dose range was only subsequently detailed in the Assessment of Toprol-XL Taken in Combination with Hydrochlorothiazide (ATTACH) trial. This was a US multicenter, randomized, double-blind, placebo-controlled, parallel group, unbalanced factorial study of 3 dose levels of hydrochlorothiazide (6.25, 12.5, and 25 mg), 4 dose levels of metoprolol ER (25, 50, 100, and 200 mg), and 9 of the 12 potential combinations (metoprolol ER/HCT: 200/6.25 mg, 25/25 mg, and 50/25 mg were not included). The design was structured to test the hypothesis that at least 1 metoprolol ER/HCT combination was superior to its components with regard to change from baseline in trough (24 hours post dosing) sitting diastolic blood pressure (SiDBP). The study enrolled men and women 18–80 years of age with SiDBP 95–114 mmHg and SiSBP <180 mm Hg (following a placebo run-in period).
The trial randomized a total of 1571 patients and met its primary objective, illustrating that the combination represented contributions from both components for both SiDBP and SiSBP, ie, the antihypertensive effects were additive. Blood pressure declined with the combination in a dose-related fashion as it did with the component agents and these declines were well described, fitted to quadratic regression dose-response surface models (Figure 3 and Figure 4). The model-derived, placebo-corrected reductions with blood pressure ranged from (SiSBP/SiDBP) 5.5/3.3 mmHg to 14.7/10.4 mmHg for the combinations (Table 1). As is also apparent in Table 1, blood pressure reductions achieved with the highest doses of the individual agents can be attained with much lower doses in combination, eg, metoprolol ER 50/HCT 6.25 mg or 12.5 mg (Papademetriou et al 2006).
Figure 3.
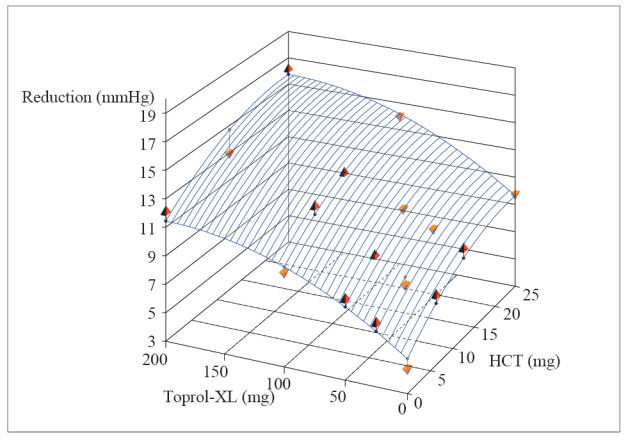
Dose response surface from polynomial regression of changes from baseline to week 8/LOCF in trough sitting diastolic blood pressure (intent-to-treat population) (ATTACH Trial).
Note: Pyramids represent the treatment group mean values. Upward pyramids are above the surface, and downward pyramids are below the surface. Lines connect the pyramids with the corresponding fitted value on the regression surface.
Regression equation: DBP: y = −5.34392 −0.06023*Toprol-XL −0.34772*HCT + 0.00015*Toprol-XL2 + 0.00703*HCT2.
Reprinted with permission from Papademetriou V, Hainer JW, Sugg J, et al, and ATTACH Study Group. 2006. Factorial antihypertensive study of an extended-release metoprolol and hydrochlorothiazide combination. Am J Hypertens, 19:1217–25. Copyright © 2006 American Journal of Hypertension, Ltd.
Figure 4.
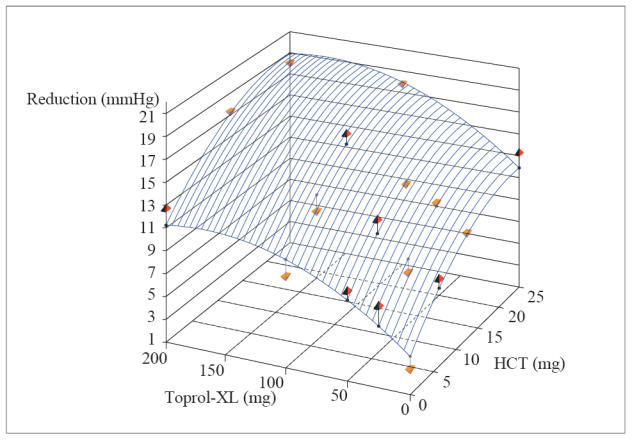
Dose response surface from polynomial regression of changes from baseline to Week 8/LOCF in trough sitting diastolic blood pressure (intent-to-treat population) (ATTACH Trial).
Note: Pyramids represent the treatment group mean values. Upward pyramids are above the surface, and downward pyramids are below the surface. Lines connect the pyramids with the corresponding fitted value on the regression surface.
Regression equation: SBP: y = −4.20691 −0.08645*Toprol-XL −0.63844*HCT + 0.00026*Toprol-XL2 + 0.01324*HCT2.
Reprinted with permission from Papademetriou V, Hainer JW, Sugg J, et al, and ATTACH Study Group. 2006. Factorial antihypertensive study of an extended-release metoprolol and hydrochlorothiazide combination. Am J Hypertens, 19:1217–25. Copyright © 2006 American Journal of Hypertension, Ltd.
Table 1.
Placebo-corrected predicted valuesafor change from baseline in SBP/DBP
| TOPROL-XL® dosage | |||||
|---|---|---|---|---|---|
| HCT dosage | 0 mg SBP/DBP |
25 mg SBP/DBP |
50 mg SBP/DBP |
100 mg SBP/DBP |
200 mg SBP/DBP |
| 0 mg | 0/0 | −2.0/−1.4 | −3.7/−2.6 | −6.1/−4.5 | −7.0/−6.1 |
| 6.25 mg | −3.5/−1.9 | −5.5/−3.3 | −7.2/−4.5 | −9.6/−6.4 | −10.5/−8.0b |
| 12.5 mg | −5.9/−3.3 | −7.9/−4.7 | −9.6/−5.9 | −12.0/−7.8 | −12.9/−9.3 |
| 25 mg | −7.7/−4.3 | −9.7/−5.7b | −11.4/−6.9b | −13.8/−8.8 | −14.7/−10.4 |
Predicted values from a least-squares quadratic regression model.
These doses were not studied.
Abbreviations: HCT, hydrochlorothiazide; SBP/DBP, systolic blood pressure/diastolic blood pressure.
When translated into hypertension control rates (<140/90 mmHg or 130/80 mmHg if diabetic) the combination rendered 31%–65% (based on dose) of patients controlled. The highest control rates attainable with the monotherapies at their highest doses were 38% for HCT and 47% for metoprolol ER. It is noted that about half the patients entered the trial with a baseline blood pressure >20/10 mmHg above their JNC goal (<140/90 mmHg or 130/80 mmHg if diabetic) and that 15%–50% of these Stage 2 hypertensive patients attained their goal with a combination regimen (Papademetriou et al 2006).
Subgroup analyses in ATTACH based on age (≥65 vs <65 years), sex, and ethnicity (Blacks vs others) identified little difference in overall antihypertensive responsiveness. Consistent with other reports, in ATTACH Blacks tended to respond to a lesser degree to metoprolol ER, and their response to diuretics was more pronounced, so that the combination was effective in both ethnic groups (Holland and Fairchild 1982; Hawkins et al 1988; Papademetriou et al 2006).
In ATTACH all patients received treatment as “initial” therapy. The effect of the metoprolol ER/HCT combination employed as an “add-on” treatment was evaluated in a smaller (n = 47) study of patients who remained hypertensive in spite of receiving HCT 12.5 mg per day. In this crossover study once daily metoprolol ER/HCT 100/12.5 mg was compared with an older metoprolol tartrate/HCT combination tablet. Blood pressure declined by approximately 10/10 mmHg with the metoprolol ER combination and 8/8 mmHg with the tartrate combination (differences not statistically significant) (data on file: Stenström Study S902 1988).
In addition to these controlled clinical trials, a number of large clinical experience trials evaluated metoprolol ER in combination with HCT (Table 2). Furthermore, 2 large hypertension clinical outcome trials (HOT and STOP-hypertension 2) allowed for the use of metoprolol ER in combination with diuretics (Table 3). In general, the experience described in these programs is consistent with the findings in the ATTACH trial and support the use of diuretic/beta-blocker combination treatment to avert the cardiovascular consequences of hypertension.
Table 2.
Clinical studies of metoprolol/hydrochlorothiazide combination tablets
| Reference | Study design/population | Number of patients | Principal findings |
|---|---|---|---|
| Hildemann et al 2002 | Prospective, open-label, 8-week, observational study/hypertensive adults | 14,964 | Mean BP reduction from baseline to week 8 was 24.5/13.6 mmHg. The reduction in BP was consistent whether or not patients were receiving other antihypertensive drugs, which included ACEIs, aldosterone antagonists, alpha-blockers, other beta-blockers, calcium antagonists, and other diuretics. Tolerability was excellent. |
| Geisler 1981 | Open-label study in patients treated with metoprolol/HCT 100/12.5 mg, 1–2 tablets daily for 6 weeks/hypertensive patients. | 12,336 | BP was significantly reduced across all age groups in this large patient population. SBP decreased by 29–30 mmHg and DBP by 13–15 mmHg after 6 weeks treatment. The incidence of AEs was low and similar in all age groups. |
| Goodfellow and Westberg 1981 | Post-marketing surveillance for 3 months of hypertensive patients in general practice. Treatment: metoprolol/HCT 100/12.5 mg, 1–2 tablets daily | 1,446 | After 3 months treatment mean BP was reduced from 181/108 mmHg to 153/91mmHg. Previously untreated patients showed a more marked reduction in BP (33/20 mmHg) than patients previously treated (23/15 mmHg). All age groups showed a similar reduction in SBP and DBP although older patients had a higher BP on entry. The incidence of AEs was similar in all age groups. Treatment was withdrawn in 117 patients due to AEs. The rate of withdrawal was somewhat higher in patients aged over 65 years. Conclusion: The fixed dose combination of HCT and metoprolol constitutes a simple once daily regimen, which is effective, produces few side-effects and is well tolerated by patients of all ages. |
| LaPalio et al 1992 | Prospective, open-label surveillance study. Multicenter outpatient. Patients with mild to moderate hypertension aged 50–75 years. Patients were treated with 100 mg of metoprolol once daily for 4 weeks. If BP was controlled, therapy continued. If not controlled, 25 mg of HCT was added. | 21,692 (approx. 6000 on metoprolol /HCT | After 4 weeks of therapy, mean SBP and DBP decreased from 162/95 to 148/87 mmHg (p < 0.001). 58% of the patients had satisfactory BP control. At 4 weeks 28% were requested to add HCT 25 mg to metoprolol 100 mg. At the end of 8 weeks, mean SBP and DBP decreased to 143/84 mmHg. BP response was similar in all age groups. At the termination of the study, 50% of the patients were continued on monotherapy, and 27% were continued on combined therapy. Overall, there was <5% incidence of medical problems, tolerability was good-excellent for 94% of the patients. Conclusion: Metoprolol administered as monotherapy or in combination with HCT was effective in normalizing BP in a majority of elderly hypertensive patients. Both regimens were well tolerated. |
| Wikstrand et al 1986 | Randomized, double-blind parallel group study of patients with untreated essential hypertension. Patients were treated with either metoprolol 100 mg or HCT 25 mg for 4 weeks. Patients with controlled DBP were treated for a further 4 weeks at the same doses. If DBP remained >95 mmHg then HCT 12.5 mg was added to metoprolol and HCT dose was doubled to 50 mg for another 4 weeks. | 562 Aged 60–75 years | A significant reduction in BP was recorded on both treatment regimens. Both treatment regimens were well tolerated. The dropout rate due to serious side-effects was similar in the 2 groups, 2% in the metoprolol group and 3% in the HCT group. Conclusion: Beginning treatment with metoprolol 100 mg bd and adding HCT 12.5 mg in patients not responding to metoprolol alone appears to be effective and safe in elderly hypertensive patients. |
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; BP, blood pressure; HCT, hydrochlorothiazide; SBP, systolic blood pressure; DBP, diastolic blood pressure; AE adverse event.
Table 3.
Clinical outcome trials in support of safety and tolerability with combination treatment
| Reference | Study design | Population and number of patients | Principal findings |
|---|---|---|---|
| Dahlof et al 1991 | This was a double-blind, multicenter, randomized study to compare antihypertensive treatment with placebo. Initial drug therapy consisted of a once-daily diuretic (25 mg HCT and 2.5 mg of amiloride), a beta-blocker (50 mg of atenolol, 100 mg of metoprolol succinate ER, or 5 mg of pindolol), or matching placebo after a 1- to 6-month washout period. Active treatment drugs could be combined if BP exceeded 160/95 mmHg after 2 months. For the placebo group, antihypertensive therapy could be added if the BP exceeded 230/120 mmHg. The primary outcome was MI, stroke, and other CV death. |
Patients had a SBP between 180 and 230 mmHg and a DBP of 90 mmHg or higher, OR a DBP of 105–129 mmHg. 1627 patients aged 70–84 years |
Average follow-up time was 25 months. At 12 months, the placebo-corrected changes in BP were greatest when the beta-blocker was combined with a diuretic. Less than 1/3 of the active treatment patients were on monotherapy. Treatment reduced total mortality by 43% (p = 0.0079) and strokes by 47% (p = 0.0081). The rate of all MIs was not reduced over this short duration of follow-up. |
| Hansson et al 1999 | This was a double-blind, multicenter, randomized study to compare older antihypertensive agents with newer agents. 1st group) Conventional treatment group, which consisted of once-daily diuretic, beta-blocker, or both: 50 mg of atenolol, 100 mg metoprolol succinate ER, 5 mg of pindolol, or the combination of 25 mg HCT and 2.5 mg of amiloride, which could be combined with the beta-blocker monotherapy if the target BP of 160/95 was not achieved. 2nd group) To achieve treatment goals, ACEI was supplemented with HCT. 3rd group) The calcium antagonists felodipine or isradipine were augmented with any of the above beta-blockers to achieve the target BP. The primary combined endpoint was fatal stroke, fatal MI, and other fatal CV diseases. |
Patients had a SBP of 180 mmHg or higher, DBP was 105 mmHg or higher, or both. Patients with isolated systolic hypertension were also included. A total of 6614 patients aged 70–84 years - 2213 patients received conventional treatment - 2205 received ACEI - 2196 received a calcium antagonists 33,249 patient-years were accumulated |
After 24 months, there was no difference in reduction of BP among the 3 treatment groups. After 60.3 months, there was no difference among the 3 groups for the primary endpoint of CV death. Major morbidity events were similar among the groups. The primary endpoint did not differ significantly among the 719 diabetic elderly patients. Combination therapy was used for 46% of patients. |
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HCT, hydrochlorothiazide; ER, extended release; CV, cardiovascular; MI, myocardial infarction.
Safety and tolerability
From a safety/tolerability perspective, prescribing physicians should view metoprolol ER/HCT as “inheriting” all the potential safety/tolerability characteristics of the individual agents, including the admonition (“black box warning”) that abrupt cessation of beta-blocker therapy can exacerbate angina pectoris or even precipitate acute myocardial infarction (TOPROL-XL® 2005). A key question for the combination is whether there are any safety/tolerability findings that are either unique to the combination or which represent an additive effect. Examples might include fatigue or metabolic abnormalities, both of which are common to each component agent. In the ATTACH trial of 1564 patients, the incidence of fatigue was 2.6% with metoprolol ER/HCT (across all doses) compared with 0.7% with placebo but at the highest dose (200/25 mg; metoprolol ER/HCT) the rate was 10.2% which compared with 2.0% and 6.3% for the individual agents, implying a possible additive effect for fatigue with high dose combinations. Relative to placebo, the rates for other common adverse effects were low: nasopharyngitis (3.4% vs 1.3%), dizziness (2.6% vs 2.6%), and nausea (1.4% vs 0.7%); adverse event discontinuation rates were 2.7% and 2.6% for combination and placebo, respectively (Papademetriou et al 2006).
The effects of thiazide diuretics and beta-blocking agents on glucose metabolism are also well described and the metoprolol ER/HCT combination would also be expected to induce similar metabolic effects (Dornhorst et al 1985; Samuelsson et al 1994; HydroDiuril 1998; TOPROL-XL® 2005). With regard to metoprolol, the large GEMENI trial noted an increase in hemoglobin A1C with immediate release metoprolol tartrate relative to the alpha-beta blocking drug, carvedilol in hypertensive type II diabetic patients already receiving a RAS blocking agent (ACE inhibitor or ARB). At the end of the trial, over 40% of the patients in both treatment groups were also receiving a thiazide diuretic (Bakris et al 2004). While the ATTACH trial noted no change in fasting glucose levels with metoprolol ER/HCT, the study was not of adequate size to critically assess an impact on glucose control in patients with diabetes as only 10% of the study subjects were diabetic (Papademetriou et al 2006). Falkner et al looked specifically at insulin sensitivity (insulin clamp method) and found that metoprolol ER did not alter insulin sensitivity when added to HCT treatment in hypertensive patients. On average, the patients were already “insulin resistant” prior to adding metoprolol ER (Falkner et al 2006). She repeated the experiment in hypertensive patients who also had diabetes but, again, found that metoprolol ER did not significantly alter insulin sensitivity (Falkner B pers comm 2007).
As one would expect, serum potassium declined with metoprolol ER/HCT in the ATTACH trial but somewhat less so than with HCT mono-therapy, perhaps attributable to renin-inhibition consequences of beta-adrenergic blockade (Figure 5) (Papademetriou et al 2006). Also as expected, the ATTACH trial noted changes in lipids with metoprolol ER. There was a small decline in mean HDL cholesterol. The combination treatments tended to reflect the influence of the effects of the individual agents: there was a small increase in total cholesterol with HCT as monotherapy and a small decline in total cholesterol with TOPROL-XL®, ie, no consistent change); and while generally small, the increases in triglyceride levels tended to be additive (Papademetriou et al 2006).
Figure 5.
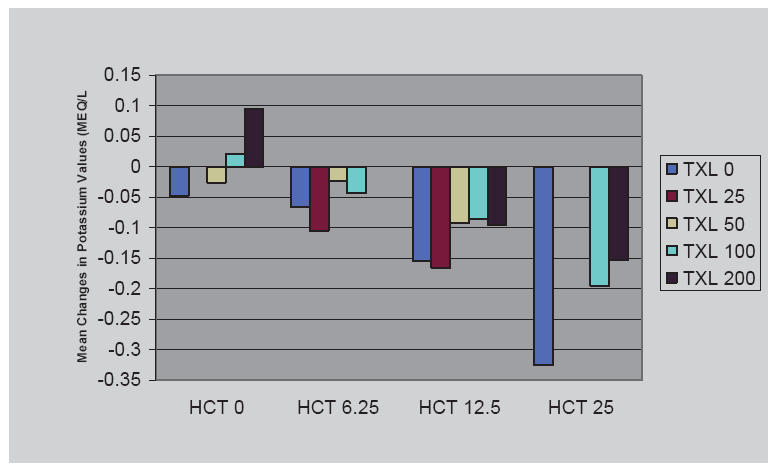
Potassium values: mean change from baseline to Visit 8 (safety population) (ATTACH Trial).
Dosing and administration
A combination metoprolol succinate ER/HCT tablet has been available in a number of countries (first approved in Denmark in 1989) as Selocomb ZOK® prolonged release tablet. In the US the FDA granted approval for the combination on 28 August 2006 as Dutoprol® – indicated for the management of hypertension. The fixed-dose combination is not indicated for initial therapy. The dosing and administration labeling cites the findings from the ATTACH trial, noting that HCT was effective in doses of 6.25–25 mg and metoprolol ER in doses of 25–200 mg and recommends that dosing be individualized considering baseline and target blood pressure as well as experience with the individual agents. Dutoprol tablet strengths (metoprolol ER/HCT) are 25/12.5 mg, 50/12.5 mg, and 100/12.5 mg, which can be divided to give half tablets of 50/6.25 mg (FDA website: http://clinicaltrials.gov).
Summary
Metoprolol succinate extended release/hydrochlorothiazide (metoprolol ER/HCT) tablets lower blood pressure in hypertensive patients. The blood pressure reductions are dose related and represent additive antihypertensive contributions from the component agents. The likelihood of controlling elevated blood pressure with the combination product is greater than with the component agents employed as monotherapies, even in patients with more severe levels of hypertension. The combination also provides an option to treat with lower doses of the individual agents. Metoprolol ER/HCT is generally well tolerated, reflecting the characteristics of the components, but it also reflects the same safety profiles including the admonition to avoid abrupt cessation of treatment in patients with or at risk for underlying coronary artery disease.
Physicians might also consider that low dose combination products provide an option to intervene with well-tolerated treatments early in the course of hypertension and might well help patients avert more intractable hypertension (Julius et al 2006). Certainly, this combination approach expands the population likely to respond to antihypertensive therapy compared with single agent treatment.
Acknowledgments
We gratefully acknowledge the assistance of Judith Borak, MS, MBA with manuscript preparation.
References
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. JAMA. 2002;288:2981–97. doi: 10.1001/jama.288.23.2981. [DOI] [PubMed] [Google Scholar]
- Bakris GL, Fonseca V, Katholi RE, et al. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension. JAMA. 2004;292:2227–36. doi: 10.1001/jama.292.18.2227. [DOI] [PubMed] [Google Scholar]
- Beermann B, Groschinsky-Grind M, Rosen A. Absorption, metabolism, and excretion of hydrochlorothiazide. Clin Pharmacol and Thera. 1976;19:531–7. doi: 10.1002/cpt1976195part1531. [DOI] [PubMed] [Google Scholar]
- Dahlof B, Lindholm LH, Hansson L, et al. Morbidity and mortality in the Swedish trial in old patients with hypertension (STOP-hypertension) Lancet. 1991;338:1281–5. doi: 10.1016/0140-6736(91)92589-t. [DOI] [PubMed] [Google Scholar]
- Darmansjah I, Wong E, Setiawati A, et al. Pharmacokinetic and pharmacodynamic properties of controlled release (CR/ZOK) metoprolol in healthy Oriental subjects: a comparison with conventional formulations of metoprolol and atenolol. J Clin Pharmacol. 1990;30:S39–S45. doi: 10.1002/j.1552-4604.1990.tb03494.x. [DOI] [PubMed] [Google Scholar]
- Dornhorst A, Powell SH, Pensky J. Aggravation by propranolol of hyperglycaemic effect of hydrochlorothiazide in type II diabetics without alteration of insulin secretion. Lancet. 1985;1:123–6. doi: 10.1016/s0140-6736(85)91900-2. [DOI] [PubMed] [Google Scholar]
- European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertension. 2003;21:1011–53. doi: 10.1097/00004872-200306000-00001. [DOI] [PubMed] [Google Scholar]
- Falkner B, Francos G, Kushner H. Metoprolol succinate, a selective ß-adrenergic blocker, has no effect on insulin sensitivity. J Clin Hypertension. 2006;8:336–43. doi: 10.1111/j.1524-6175.2006.05247.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geisler LS. Hypertension therapy in the elderly. MedWelt. 1981;32:910–14. [PubMed] [Google Scholar]
- Goodfellow R, Westberg B. The treatment of high blood pressure in the elderly: a multi-center evaluation of a fixed combination of metoprolol and hydrochlorothiazide (Co-Betaloc) in general practice. Curr Med Res Opin. 1981;7:536–42. doi: 10.1185/03007998109112370. [DOI] [PubMed] [Google Scholar]
- Gu Q, Paulose-Ram R, Dillon C, Burt V. Antihypertensive medication use among US adults with hypertension. Circulation. 2006;113:213–21. doi: 10.1161/CIRCULATIONAHA.105.542290. [DOI] [PubMed] [Google Scholar]
- Hajjar I, Kotchen T. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA. 2003;290:199–206. doi: 10.1001/jama.290.2.199. [DOI] [PubMed] [Google Scholar]
- Hansson L, Lindholm LH, Ekbom T, et al. Randomized trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity the Swedish trial in old patients with hypertension-2 study. Lancet. 1999;354:1751–6. doi: 10.1016/s0140-6736(99)10327-1. [DOI] [PubMed] [Google Scholar]
- Hawkins DW, Dieckmann MR, Horner RD. Diuretics and hypertension in black adults. Arch Intern Med. 1988;148:803–5. [PubMed] [Google Scholar]
- Hildemann SK, Fischer H, Pittrow D, et al. Metoprolol succinate SR plus hydrochlorothiazide (Beloc-Zok® Comp) in patients with essential hypertension in general practice. A prospective, observational trial in 14,964 patients. Clin Drug Invest. 2002;22:719–29. [Google Scholar]
- Holland OB, Fairchild C. Renin classification for diuretic and beta-blocker treatment of black and hypertensive patients. J Chron Dis. 1982;35:179–82. doi: 10.1016/0021-9681(82)90138-2. [DOI] [PubMed] [Google Scholar]
- HydroDiuril® (hydrochlorothiazide) professional information brochure. Merck & Co., Inc; 1998. [Google Scholar]
- JNC 7 report. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA. 2003;289:2560–71. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- Jordo L, Johnsson G, Lundborg P, et al. Bioavailability and disposition of metoprolol and hydrochlorothiazide combined in one tablet and of separate doses of hydrochlorothiazide. Br J Clin Pharmacol. 1979;7:563–7. doi: 10.1111/j.1365-2125.1979.tb04643.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Julius S, Nesbitt SD, Eagan BM, et al. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N Engl J Med. 2006;354:1685–97. doi: 10.1056/NEJMoa060838. [DOI] [PubMed] [Google Scholar]
- LaPalio L, Schork A, Glasser S, et al. Safety and efficacy of metoprolol in the treatment of hypertension in the elderly. J Am Geriatr Soc. 1992;40:354–8. doi: 10.1111/j.1532-5415.1992.tb02134.x. [DOI] [PubMed] [Google Scholar]
- Mourad J-J, Waeber B, Zannad F, et al. on behalf of the investigators of the STRATHE trial. Comparison of different therapeutic strategies in hypertension: a low-dose combination of perindopril/indapamide versus a sequential monotherapy or a stepped-care approach. Journal of Hypertension. 2004;22:2379–86. doi: 10.1097/00004872-200412000-00021. [DOI] [PubMed] [Google Scholar]
- Ofili E. Dispelling the myth of “aggressive” antihypertensive therapy. J Clin Hypertens. 2006;8(Suppl 1):4–11. doi: 10.1111/j.1524-6175.2005.05293.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Papademetriou V, Hainer JW, Sugg J, et al. ATTACH Study Group. Factorial antihypertensive study of an extended-release metoprolol and hydrochlorothiazide combination. Am J Hypertens. 2006;19:1217–25. doi: 10.1016/j.amjhyper.2006.05.007. [DOI] [PubMed] [Google Scholar]
- Papademetriou V, Reif M, Henry D, et al. Combination therapy with candesartan cilexetil and hydrochlorothiazide in patients with systemic hypertension. J Clin Hypertens. 2000;2:372–8. [Google Scholar]
- Plosker GL, Clissold SP. Controlled release metoprolol formulations: a review of their pharmacodynamic and pharmacokinetic properties, and therapeutic use in hypertension and ischaemic heart disease. Drugs. 1992;43:382–414. doi: 10.2165/00003495-199243030-00006. [DOI] [PubMed] [Google Scholar]
- Psaty BM, Lumley T, Furberg C, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents. JAMA. 2003;289:2534–44. doi: 10.1001/jama.289.19.2534. [DOI] [PubMed] [Google Scholar]
- Samuelsson O, Hedner T, Berglund G, et al. Diabetes mellitus in treated hypertension: incidence, predictive factors and the impact of non-selective beta-blockers and thiazide diuretics during 15 years treatment of middle-aged hypertensive men in the primary prevention trial Goteborg, Sweden. J Hum Hypertens. 1994;8:257–63. [PubMed] [Google Scholar]
- Sandberg A, Ragnarsson G, Jonsson UE, et al. Design of a new multiple-unit controlled-release formulation of metoprolol – metoprolol CR. Eur J Clin Pharmacol. 1988;33:S3–S7. doi: 10.1007/BF00578405. [DOI] [PubMed] [Google Scholar]
- Sandberg A, Abrahamsson B, Regârdh C-G, et al. Pharmacokinetic and biopharmaceutic aspects of once daily treatment with metoprolol CR/ZOK: a review article. J Clin Pharmacol. 1990;30:S2–S16. doi: 10.1002/j.1552-4604.1990.tb03490.x. [DOI] [PubMed] [Google Scholar]
- The Association of Black Cardiologists (ABC) Candesartan Study Group. Evaluation of candesartan cilexetil in black patients with systemic hypertension: The ABC Trial. Heart Dis. 2000;2:392–9. [PubMed] [Google Scholar]
- TOPROL-XL® (metoprolol succinate) Extended Release Tablets professional information brochure. AstraZeneca LP; 2005. [Google Scholar]
- Turnbull F, Neal B, Algert C, et al. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–35. doi: 10.1016/s0140-6736(03)14739-3. [DOI] [PubMed] [Google Scholar]
- Wikstrand J, Westergren G, Berglund G, et al. Antihypertensive treatment with metoprolol or hydrochlorothiazide in patients aged 60 to 75 years. JAMA. 1986;255:1304–10. [PubMed] [Google Scholar]
- [WHO] World Health Organization, International Society of Hypertension Writing Group. World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–92. doi: 10.1097/00004872-200311000-00002. [DOI] [PubMed] [Google Scholar]